
Abstract
Background: The purpose of this study was to evaluate the results of operative treatment of recurrent peroneal tendon dislocations followed by accelerated rehabilitation incorporating early range of motion and intermittent immobilization. Methods: Four female and nine male athletes with an average age of 24 years had objective clinical evidence of peroneal tendon dislocation (14 ankles). Operative treatment involved removing a bone flap from the distal posterior fibula, deepening the posterior fibular groove, and reattaching the bone flap within the deepened groove. The superior peroneal retinaculum also was reconstructed. Postoperatively, a removable boot was worn for approximately 4 weeks, when it was replaced with a stirrup brace. Results: At an average followup of 35 months, no recurrent subluxation or dislocation of the peroneal tendons had occurred. All patients were able to return to sports by 3 months after surgery. Nine of the 14 ankles regained normal range of motion, and the remaining five were within 5 degrees of the opposite side. Four patients were completely pain free, and nine patients had mild occasional pain that did not limit their activities. Eight patients returned to preinjury sports participation, and five patients elected to participate in sports at a level lower than they had before surgery for reasons not related to their ankle injury. Conclusions: This procedure was reliable for preventing recurrent peroneal tendon instability. Range of motion was nearly normal, immobilization time was minimal, and all patients returned to daily activities and sports within 3 months of surgery.
INTRODUCTION
Chronic peroneal tendon subluxation can be a disabling condition for an athlete. 2 The structure of the fibula itself may contribute to this chronic condition. The peroneus longus and brevis tendons descend along the fibula and follow the posterior fibular groove of the lateral malleolus. The combination of the posterior fibular groove and the superior peroneal retinaculum secures the peroneal tendons to the posterior fibula and prevents dislocation of the tendons anteriorly over the lateral malleolus. If the superior peroneal retinaculum is attenuated or ruptured or if the posterior groove is shallow, flat, or convex, the peroneal tendons are more likely to subluxate. 7,8,9
Chronic peroneal tendon subluxation is the result of an acute injury that occurs when the ankle is dorsiflexed (most commonly) or plantarflexed, and the peroneal muscles contract to create a force that everts the foot against resistance. The combination of these motions results in the rupture of the superior retinaculum allowing the peroneal tendons to dislocate anterolaterally over the lateral malleolus. 2,8,9 Swelling, ecchymosis, and tenderness posterior to the lateral malleolus may be noted after peroneal tendon subluxation. 2,5,9
The optimal treatment for acute peroneal tendon dislocation remains controversial. However, for chronic, recurring subluxation or dislocation, operative intervention often is required. Numerous operative procedures have been advocated for the chronically unstable tendon, including rerouting the tendons, 2,6,9 reinforcing or reconstructing the peroneal retinaculum by soft-issue procedures 2,6 and deepening the fibular groove with bony procedures. 9
The outcomes of operative treatment such as soft-issue reconstruction and fibular osteotomies have been more successful than nonoperative treatment. 2 In one operative procedure, 9 osteotomy of the distal posterolateral fibula is done to deepen the fibular groove, resulting in a bone flap that remains attached to the posteromedial fibula. We used a modification of this procedure that includes complete removal of the cortical bone flap, deepening of the posterior fibular groove, and reattachment of the cortical bone flap to the base of the fibular groove.
Most authors recommend a period of nonweightbearing cast immobilization after surgery to ensure healing of the fibular osteotomy and superior peroneal retinacular reconstruction. 3,6,7,8 Our postoperative treatment included intermittent immobilization with a walking boot instead of cast immobilization. This accelerated rehabilitation, allowed for early range of motion, and immediate weightbearing.
The purpose of this study was to determine if this technique provided adequate stabilization of the peroneal tendons to allow early return to functional activity and maintenance of range of motion.
MATERIALS AND METHODS
Patients
From 1991 to 1998, 185 athletic patients were treated for recurrent lateral ankle sprains or peroneal tendon pathology. Of these, 17 patients were treated operatively for recurrent peroneal tendon dislocation or subluxation. Of these, one was lost to followup, one had concurrent lateral ankle reconstruction, and two were not considered athletes, leaving 13 athletes (14 ankles) who fit our inclusion criteria (Table 1). In the nine males and four females, seven left ankles and seven right ankles were involved. The average age at the time of surgery was 24 (range 13 to 47) years.
Each patient provided informed consent for the study and operative treatment, and the protocol for surgery and rehabilitation was approved by the Institutional Review Board of Clarian Health, the Methodist Hospital of Indiana.
Inclusion Criteria
Preoperative Evaluation and Treatment
Sports activity at the time of initial peroneal tendon dislocation was recorded (Table 2). On clinical preoperative examination, all patients had demonstrable peroneal tendon dislocation or subluxation, demonstrated either actively by the patient or passively by the examining physician by plantarflexing and everting the ankle while pushing the tendon anteriorly over the lateral border of the fibula.
Anteroposterior, lateral, and oblique weightbearing radiographs were obtained of each involved ankle. At initial evaluation, each athlete was counseled regarding the high incidence of failure with nonoperative treatment, but all opted for at least a short course of nonoperative treatment. The nonoperative treatment consisted of cold compression therapy, a U-pad felt wrap with a stirrup brace, and immobilization in a walking boot. All 13 athletes experienced recurrent subluxation or dislocation after an average of 4 months (15 weeks to 12 months) of nonoperative treatment and therefore opted for operative intervention.
Operative Technique
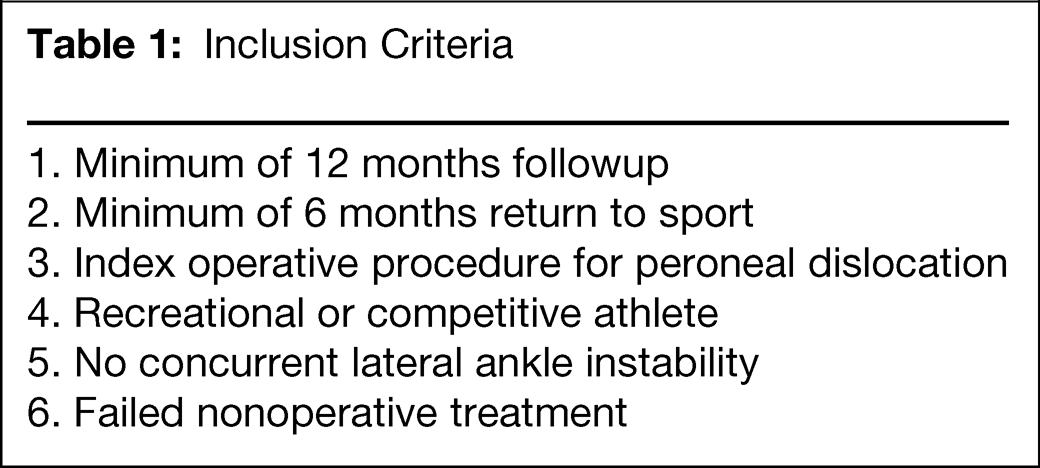
The procedure was done with a regional ankle block and intravenous sedation (10 patients) or with general anesthesia (four patients). The patient was placed in a lateral decubitus position (10 patients) or prone (four patients). A tourniquet with cotton padding was placed on the calf and inflated to 275 mmHG. The ankle block was placed at a level above the tourniquet to decrease tourniquet pain. A posterolateral curvilinear incision was made along the course of the peroneal tendons, and the peroneal tendon sheath and superior peroneal retinaculum were incised in line with the incision just off the posterior border of the fibula. The tendons were dislocated, and a 1.5-mm drill and small osteotome were used to remove a corticocancellous flap of bone from the posterior fibular sulcus (Figure 1). No attempt was made to hinge the posterior bone flap.
Sport activity at the time of peroneal tendon dislocation

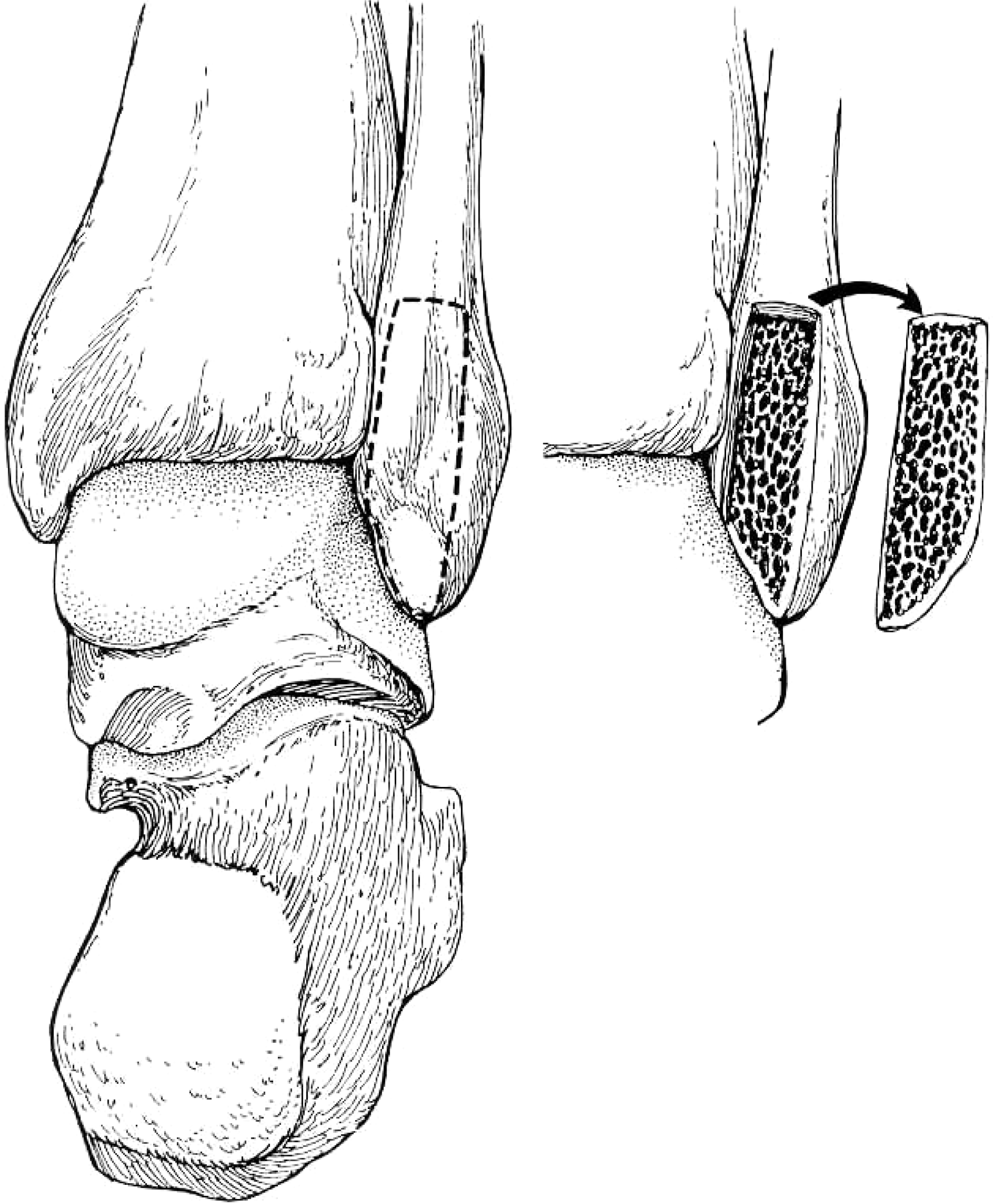
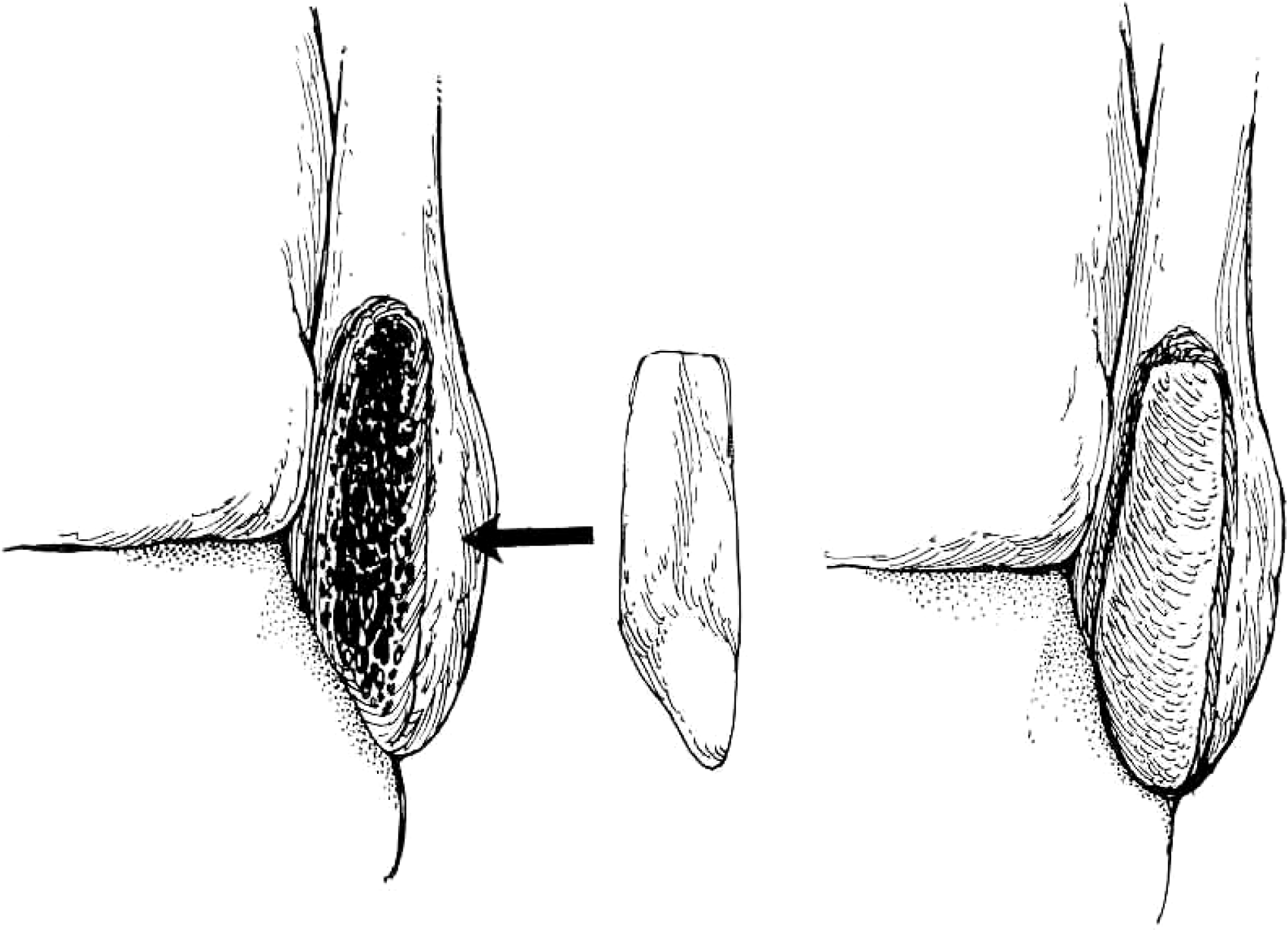
The distal posterior sulcus was deepened with a 4-mm burr so that the peroneus longus and brevis tendons sat completely within the deepened groove, with the posterior border of the tendons flush with the posterior border of the fibular cortex. The cancellous bone flap was then replaced within the deepened groove with the serosal surface toward the peroneal tendons to provide a smooth gliding surface and secured with resorbable suture (Figures 2 and 3). The lateral border of the fibula was roughened with a 4.0-mm burr, and the superior peroneal retinaculum was reattached to the fibula with absorbable, braided 2-0 Ethibond sutures (Ethicon, Cincinnati, OH) through drill holes. The remaining retinaculum was imbricated into the posterior border of the fibula, recreating the retinacular roof. The ankle was moved through a full range of motion to ensure that there were no restrictions.
One patient had a lateral process fracture that required concomitant open reduction and internal fixation. Another patient had a longitudinal tear of the peroneus longus tendon, which was repaired at the time of the grove deepening and retinacular reconstruction.
Corticocancellous bone window removed from the posterior fibula.
Groove deepening and cortical bone serosal surface placed in the depth of the groove.
Postoperative Evaluation
Each patient was evaluated clinically during a followup office visit. The followup evaluation was done by independent observers (a physical therapist for strength and range of motion and a research assistant for administering the questionnaire and assessment of complications and return to sports). Postoperative radiographs were obtained and American Academy of Orthopaedic Surgeons (AAOS) Lower Limb Core Module and Foot and Ankle Module 1 were completed at this time. Range of dorsiflexion, plantarflexion, inversion, and eversion were measured with a goniometer by the principal investigator (DP). Dynamometer testing was performed at 60°/sec, 120°/sec and 180°/sec to evaluate strength (Cybex, CSMI, Boston, MA) in dorsiflexion, plantarflexion, inversion, and eversion and was compared to the opposite ankle. Duration of use of crutches, walker boot, and stirrup brace, and duration of recovery period before return to sports, were recorded.
Postoperative Rehabilitation
A cold pack (Aircast® ankle Cryo/Cuff®, Aircast Inc., Summit, NJ) inside a removable walking boot (Aircast®, Foam Walker, Aircast, Inc., Summit, NJ) was applied at the end of the operative reconstruction. Initial nonweightbearing crutch use to decrease the risk of swelling was tapered off beginning 2 or 3 days after surgery. At the first postoperative visit (1 week after surgery), active and active-assisted range-of-motion exercises, desensitization exercises (cross-frictional massage), and stationary bicycle riding with the boot in place were begun. Range-of-motion exercises included plantarflexion and dorsiflexion with inversion. Dorsiflexion with eversion was not allowed during the first 4 weeks after surgery. Three weeks after surgery, the athlete was allowed to begin biking while wearing a stirrup brace (Active Ankle®, Louisville, KY). Four weeks after surgery, the athlete began to taper out of the boot into a stirrup brace over 10 to 14 days, began stair-climber workouts while wearing the stirrup brace, initiated toe-raise strengthening and proprioception retraining exercises and was allowed to perform active dorsiflexion with eversion exercises for peroneal strengthening. Six weeks after surgery, the athletes began running and functional progression exercises while wearing the stirrup brace. After completing the functional progression, the athlete was permitted to resume his or her individual sport.
Groove deepening and retinacular reconstruction for peroneal dislocation.
RESULTS
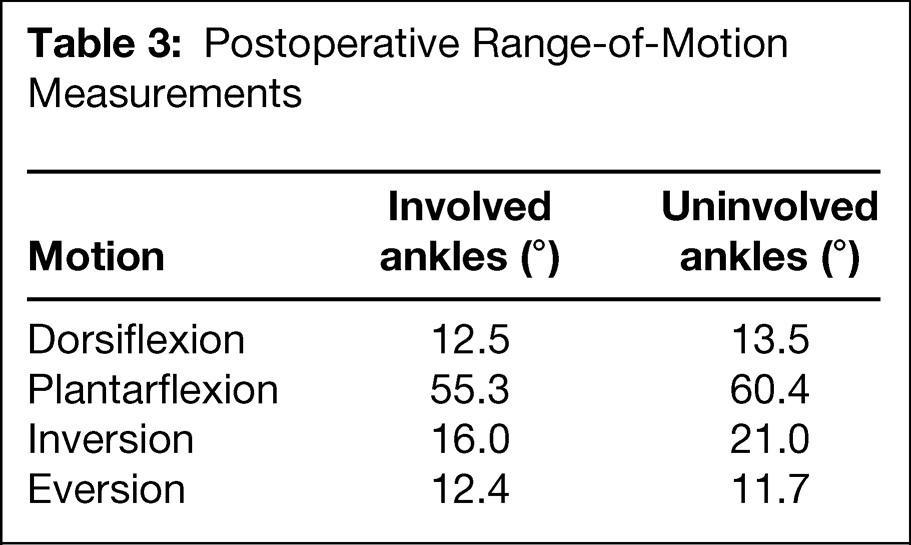
At an average of 35 (16 to 98) months after surgery, there were no recurrent peroneal dislocations or subluxations. All athletes were free of local swelling and tenderness at last followup. Radiographs demonstrated no spurring, arthritic changes, bony avulsions, or abnormalities referable to the operative procedure. The ankle and subtalar joint range-of-motion measurements were near normal (Table 3). On average there was a 1-degree loss of dorsiflexion, a 5-degree loss of plantarflexion, and a 5-degree loss of inversion in the involved ankle compared to the uninjured ankles. The measurements for eversion indicated that the involved ankles had similar eversion as the uninvolved ankles. There was no statistical difference (p > 0.05) in range of motion in any direction measured.
Postoperative Range-of-Motion Measurements
At final followup evaluation, no athletes complained of peroneal tendon discomfort or weakness. The AAOS Lower Limb Core Module Foot and Ankle Module 1 mean pain score was 95 (80 to 100) out of 100. Four athletes had no pain, and nine had occasional mild pain that did not limit their activities. No athlete complained of discomfort that limited activity or performance. The mean AAOS Lower Limb Core Module and Foot and Ankle Module core function score was 100 ± SD out of 100 (95 to 100).
Dynamometer Strength Testing After Surgery
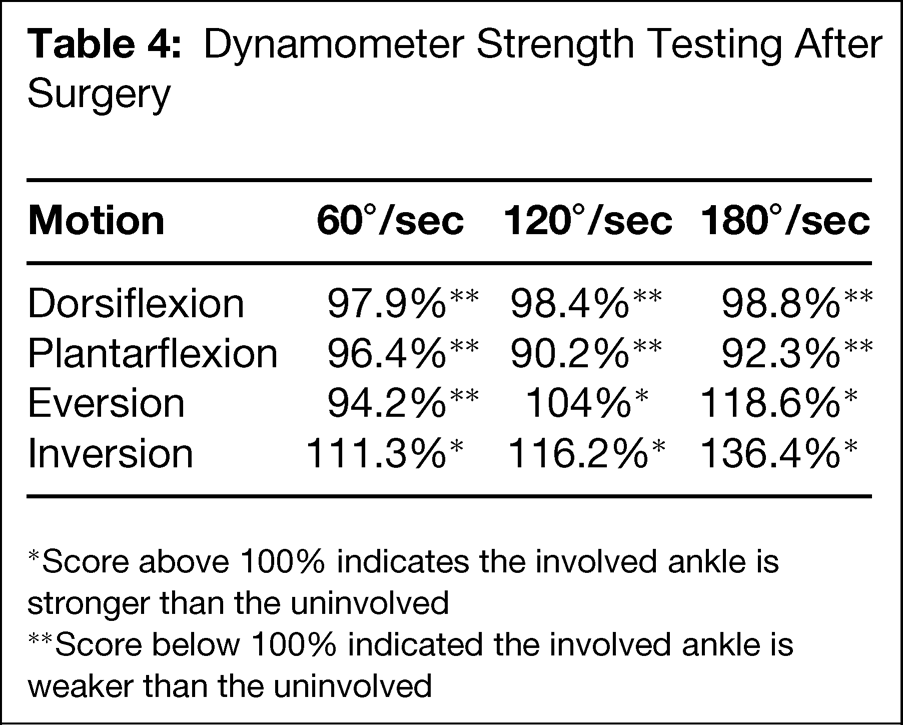
Score above 100% indicates the involved ankle is stronger than the uninvolved
Score below 100% indicated the involved ankle is weaker than the uninvolved
No athlete had evidence of peroneal muscular atrophy or complained of weakness. Isokinetic strength testing demonstrated that the involved ankle regained nearly normal strength compared to the uninvolved ankle (Table 4).
The average total time on crutches was 15 (7 to 30) days, and the average total time for boot usage was 5 (2 to 6) weeks. The stirrup brace was worn for an average of 5 (2 to 12) weeks. All athletes returned to participation in sports; eight to the same level as before their injury and five to a lower level for reasons not related to their ankles. The average time to return to sports was 3 (1.3 to 7) months after surgery.
The average tourniquet time was 38 minutes, and there were no tourniquet-related complications. There were no wound healing problems, infections, nerve injuries, or painful scars. No athlete complained of giving way or ankle instability.
DISCUSSION
We modified the fibular groove deepening procedure 9 and combined it with a soft-tissue reconstruction of the superior peroneal retinaculum. The results showed that this is a simple and reproducible procedure that provides excellent stability, allows early range of motion and has a low risk for complications.
Complete removal of the bone flap allows removal of remaining cancellous bone attached to the flap and gives a symmetric, deep groove in which both tendons rest completely, reducing the risk for recurrent dislocation. We have had no bony complications from detachment of the bone flap. The inherent stability provided by the symmetric, deepened groove allowed functional bracing rather than casting, and the patients were able to begin range-of-motion exercises immediately after surgery.
Moreover, preserving the serosal surface within the fibular groove provided a smooth surface for tendon gliding. This may provide improved nutrition for the tendons, and the deeper groove may maximize the stability of the tendons within the fibular groove. Furthermore, placing the serosal surface back within the groove may lessen the risk of scarring and adhesions of the peroneal tendons, evidenced by the nearly normal motion after surgery.
Although some authors have used soft-tissue reconstruction alone for treatment of chronic peroneal tendon dislocations, 2 we combined the soft-tissue procedure with the modified groove deepening to close the ceiling over the deepened groove. The soft-tissue reconstruction involved imbrication of the superior peroneal retinaculum by bony reattachment to the posterior border of the fibula. The lateral fibula was roughened to allow the retinaculum to scar down to the bony fibula and obliterate the false pocket created by the chronic tracking of the dislocated peroneus longus tendon. The superior peroneal retinaculum can be augmented by sewing local periosteum over the soft-tissue reconstruction if the retinacular tissue is tenuous. Combining the soft-tissue reconstruction of the superior peroneal retinaculum with the deep symmetric fibular groove resulted in no postoperative dislocations in our patients at an average followup of 35 months.
The outcomes of this operative procedure for peroneal tendon subluxations are promising. All of the postoperative radiographs appeared normal, the AAOS Lower Limb Core Module and Foot and Ankle Module scores 1 indicated that the patients experienced little or no pain after surgery and rehabilitation and were able to perform activities of daily living and sports.
The range-of-motion measurements of the operatively treated ankles were almost equal to the measurements of the uninvolved ankles, indicating full return to mobility. Results of isokinetic dynamometry tests showed little difference in strength between the involved and uninvolved ankles. The early mobilization may have contributed to the excellent strength and early return to full activity and sports.
There were no significant complications from this procedure. We were careful to make our incision anterior to the sural nerve to decrease the risk of sural nerve injury or entrapment in scar. We also were aggressive with postoperative cross-frictional massage to decrease the risk of scar buildup and to help desensitize the nerve. The use of early range-of-motion exercises likely reduced the risk of stiffness and scar. The ankle block was effective in eliminating the pain from the tourniquet by blocking above the tourniquet.
The results of this operative technique and immediate mobilization compare favorably to outcomes reported in the literature. None of the athletes treated with this operative technique had recurrent dislocations or subluxations and all were able to return to sports. This is similar to results reported previously, 4,9 but with an earlier (average 5 months) return to sports.
Limitations of this study include the case-controlled design and the lack of a control group, making comparisons to other treatments difficult. The number of subjects in the study is limited because peroneal tendon subluxation is not a common finding. Furthermore, we did not obtain preoperative subjective questionnaires and were thus unable to compare preoperative and postoperative scores.