
Abstract

INTRODUCTION
Fractures of the body of the talus are rare, representing 0.1% to 0.3 % of all fractures and 18% of talar fractures. 1,4 Between 11% to 18% of all talar fractures occur with concomitant calcaneal fractures, 2 but the combination of fractures seen in this patient have not been reported in the literature. The outcome for this type of talar fracture often is poor, leading some to suggest primary tibiotalocalcaneal or tibiocalcaneal arthrodesis as treatment. 5 This case illustrates a good result with open reduction and internal fixation of the talar body.
CASE REPORT
A 22-year-old, non-smoking, male electrician was participating in motocross and jumping off a hill when he came off the back of his bike and fell approximately 20 feet landing on his feet. He was seen in the emergency room and was diagnosed with an ankle sprain and advised to have an orthopaedic evaluation the following week.
When he was examined 4 days later, he had surprisingly little swelling and no abnormalities on neurovascular examination. Plain radiographs and CT scans in an oblique axial plane perpendicular to the calcaneal posterior facet were obtained and showed the fractures of the talar body, calcaneus, and navicular (Figure 1). CT sagittal and coronal reconstructions were carefully reviewed before surgery to help delineate the three-dimensional nature of the fracture. The patient was advised of the severity of his injury and options were discussed. He chose to have open reduction and internal fixation understanding that arthrodesis might be necessary in the future.
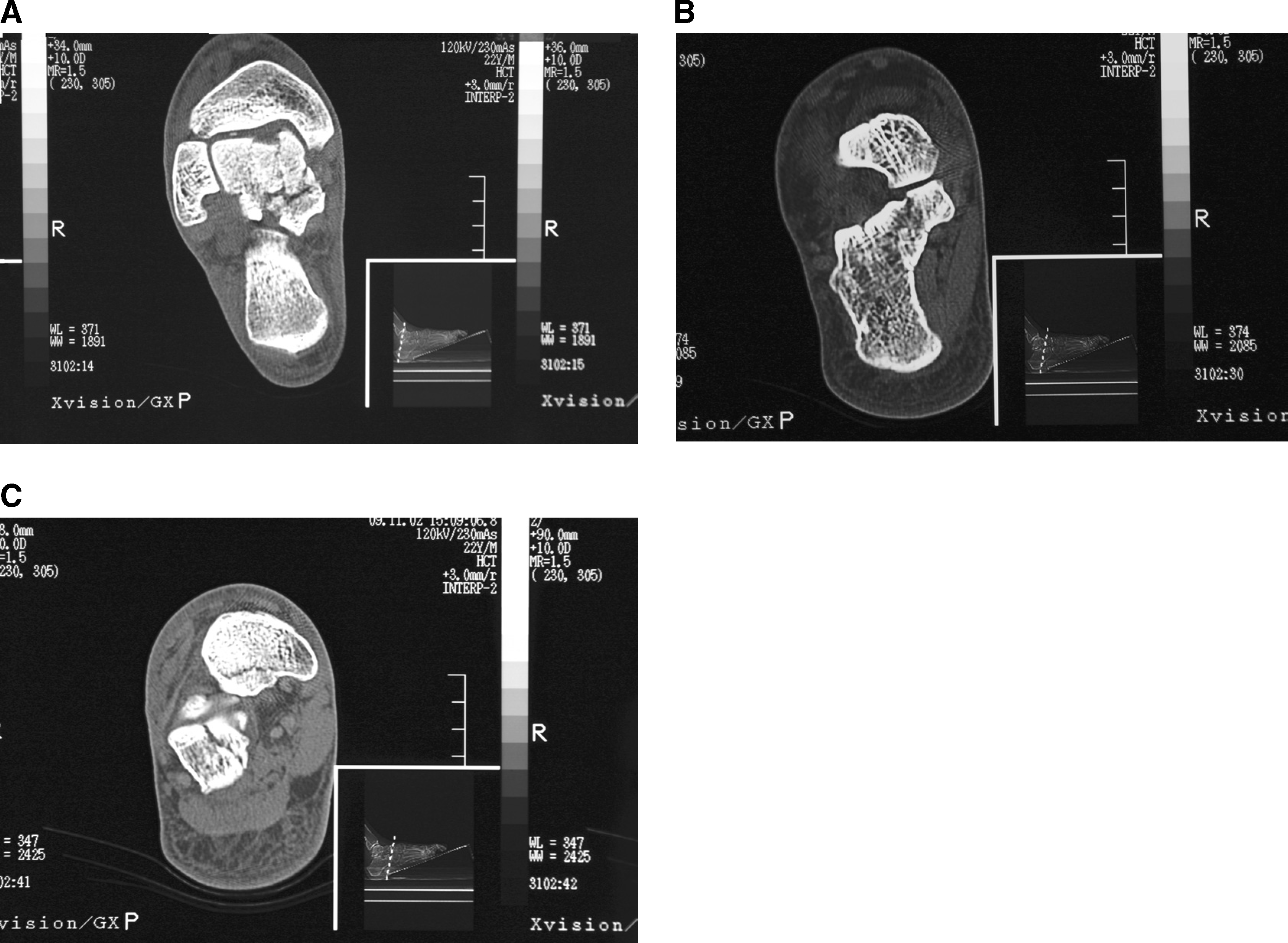
Axial CT images of the fractures.
Because he had such little swelling, he was taken to the operating room the next day. The navicular fracture was approached first using percutaneous techniques. With a 4-0 cannulated screw securing that fracture, the leg was exsanguinated and the tourniquet inflated. A long vertical incision was made over the medial malleolus with the inferior aspect curving anteriorly along course of the posterior tibial tendon, and full-thickness skin flaps were developed. Using image intensification, a 4-0 cannulated screw was then placed in the sustentaculum tali to secure these fragments. The entry point was carefully pre-drilled to avoid fragmentation. With that fracture stabilized, osteotomy and repair of the talus could be done.
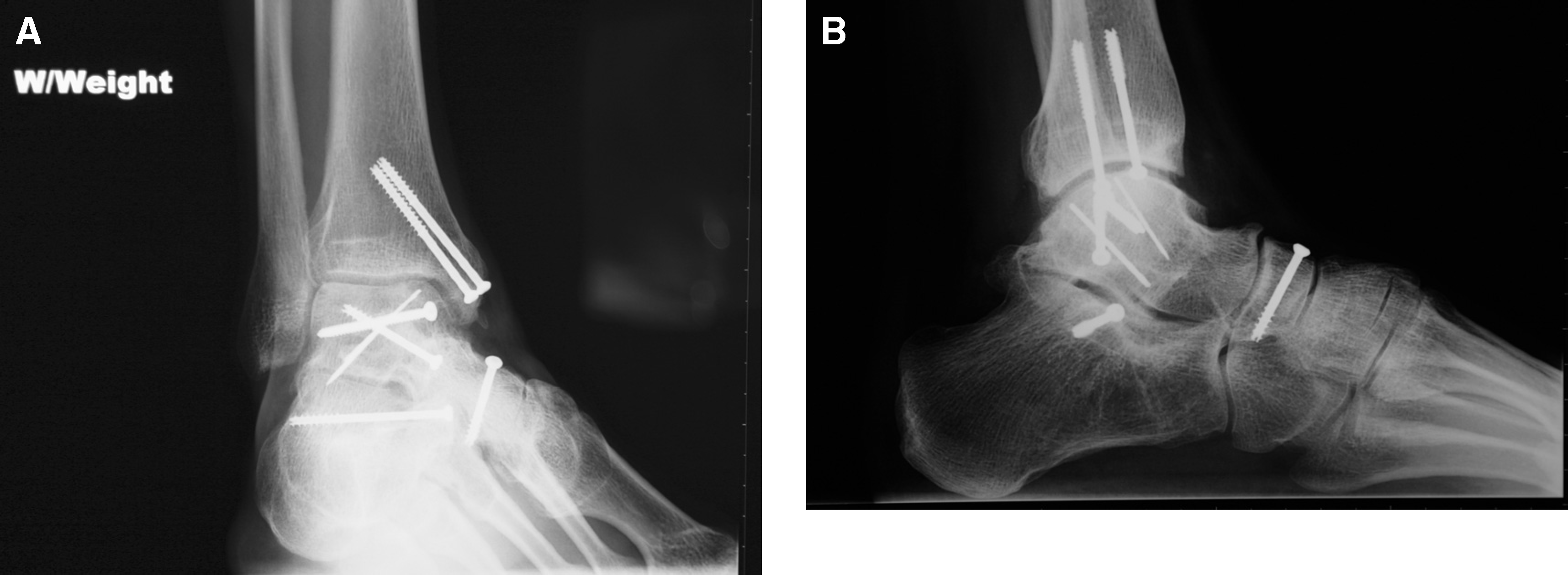
An oblique osteotomy of the medial malleolus was made, and gentle retraction was placed on the medial malleolar fragment to avoid damaging the blood supply in the deep deltoid. This revealed the complicated nature of the fracture pattern well. The large, central fragment was found to be depressed more than appreciated on the CT scan. Elevation of this fragment was a difficult, slow process with a dental pick and a Freer elevator. However, it was finally elevated 0.5 mm to 1 mm higher than its normal position to allow for some settling. The other fragments were reduced, and a 4-0 cannulated screw and a small fragment screw in compression mode were placed. The superomedial fragment was first reduced with a cortical screw, but the fragment was too small to allow sufficient countersinking to avoid the head being proud in the joint, so the fragment was secured with a Kirschner wire. With the major fragments reduced, the posterior fragment fell into good position so no further fixation was placed. Portable films were taken to confirm image intensification views and then the medial malleolus was reduced and fixed with 4-0 cannulated screws (Figure 2).

Intraoperative portable radiographs.
A bulky posterior plaster splint was applied, and the patient was monitored in the hospital overnight. Eight days after surgery, the stitches were removed and a removable cast boot was fitted. He began a home program for range of motion: ankle plantar/dorsiflexion at least 100 times and 20 circumductions in each direction each day. At his 6-week follow up he had a positive Hawkins sign on radiographs and he began formal physical therapy for ankle range of motion. At 9 weeks, the radiographs showed excellent healing response at the navicular and increased talar body radiodensity so partial weightbearing (up to 50 lbs) was begun. At 12 weeks, radiographs showed excellent healing, so full weightbearing was begun in a cast boot, and he was gradually weaned into a running shoe. At 16 weeks he was released to full activity.
At his 18-month followup visit, he reported that he had been able to return to his work as an electrician and to his recreational motocross activities. Squatting down for any length of time resulted in some pain over the anterior tibial tendon when he stood, but this resolved after he took a few steps. He also had discomfort if his motocross activities put a sharp dorsiflexion force on the forefoot. He was playing basketball as much as 3 hours each week without significant problems. Weightbearing films showed excellent maintenance of his tibiotalar and talocalcaneal joint spaces (Figure 3).
Eighteen-month weightbearing mortise
Physical examination showed a calf circumference on his injured side of 34 cm compared to 34.5 cm on the contralateral side. Ranges of motion in his injured and noninjured legs were, respectively, ankle dorsiflexion 7 and 10 degrees, plantarflexion 20 and 30 degrees, inversion 5 and 40 degrees, and eversion 0 and 5 degrees. He had symmetrical strength. His American Orthopaedic Foot and Ankle Society ankle-hindfoot score 3 was 82.
DISCUSSION
Crush injuries to the talus usually lead to poor outcomes. Since both the tibiotalar and talocalcaneal articulations are involved, arthritis, and reduced range of motion are common. In this patient the talar injury was combined with fractures of the calcaneus and the tarsal navicular. Fortunately, the calcaneal fracture was minimally displaced and involved only a small portion of the anterior aspect of the posterior facet. However, it seems reasonable to assume that both fractures contributed to his significant loss of subtalar motion. Whether the concomitant navicular fracture played a role in this loss of motion is unknown, but it seems unlikely.
In this patient, preoperative review of CT sagittal and coronal reconstructions was invaluable. Scrolling through the reconstructions on the monitor allowed the development of a mental three-dimensional picture of the fractures. The medial malleolar osteotomy provided excellent exposure of the articular surface and united uneventfully. It is interesting that the Hawkins sign was predictive of adequate blood supply in this crush injury, although it usually is used following talar neck fractures.
CONCLUSION
Although some have suggested that primary arthrodesis should be considered for this type of fracture, 5 open reduction and internal fixation should be considered for a healthy, active, nonsmoking patient. It seems very unlikely that this patient would have been able to return to his current level of activity with an arthodesis. With this severe injury, posttraumatic arthritis is possible, and our current followup is too short to make any predictions. However, if that becomes a problem in the future, the techniques used here do not eliminate the option of arthrodesis.