
Abstract
Background: The purpose of the study was to evaluate the outcome of flexor digitorum longus (FDL) transfer to the dorsum and to identify a possible continued role for this transfer in conjunction with additional surgeries for second metatarsophalangeal joint (MTPJ) instability. Methods: We carried out a retrospective analysis on patients with second MTPJ instability for which the FDL transfer was done as the primary procedure between 1996 and 2001. The patients were examined for functional status, residual pain, and satisfaction. Results: A total of 64 feet (59 patients) were evaluated, with an average followup period of 45.2 (16 to 82) months. A cross-over second toe deformity was present in 56 feet (87%) with a stage II deformity being the most common (18 feet). There also were seven feet with vertical subluxation. An additional second metatarsal Weil osteotomy was done in 29 feet (45%), a proximal interphalangeal (PIP) joint resection arthroplasty in 22 feet, and a PIP joint fusion in nine feet. At final followup of the 59 feet that were physically examined, 22 (37%) had residual second MTPJ dorsiflexion contracture and 16 feet had persistent medial deviation. The second toe was stable to stress manipulation in 46 feet (78%). The mean toe pulp to ground distance on standing was 3 mm, and strong toe grasp was possible in 45 feet. There were 20 complications in 64 feet. Twenty-five patients (29 feet) were very satisfied, 15 satisfied with minor reservations, six with major reservation, and 14 patients were unhappy with the outcome. The American Orthopaedic Foot and Ankle Society functional score was on average 82 points (47 to 100) at final followup. Conclusion: Although the function of the second toe improved in most patients as a result of pain relief, a substantial number of the patients in this study remained dissatisfied because of residual stiffness of the toe. The flexor tendon transfer remains an important procedure in correction of second toe instability but must be used with a full understanding of potential complications and patient dissatisfaction.
INTRODUCTION
Instability of the metatarsophalangeal joint (MTPJ) of the second toe caused by the rupture of the plantar plate is a challenging entity to treat. Considerable controversy exists in the literature regarding operative correction. 3,4,6,10 The transfer of the split flexor digitorum longus (FDL) tendon to the dorsum of proximal phalanx, which has been used for treating flexible clawtoe deformity, 9,14 has become increasingly popular to treat various instabilities of the second MTPJ. However, few reports on this subject examine patient outcomes and satisfaction after this procedure. 4,8,10,15 More recent reports have suggested the important role of a shortening osteotomy of the metatarsal with or without a tendon transfer. 16 Our anecdotal results of flexor-to-extensor tendon transfer seemed to be associated with far more morbidity than indicated in the literature. 4,5,15 The purpose of this study was to evaluate the outcome of this treatment and to identify any possible continued role for this transfer in conjunction with additional surgeries for the management of second toe MTPJ instability.
MATERIALS AND METHODS
We retrospectively reviewed 59 patients (64 feet) undergoing treatment for second MTPJ instability for which a modification of the FDL transfer was the primary procedure between 1996 and 2001. 2 Institutional Review Board approval and informed consent were obtained for this study. The patients' charts were reviewed for demographic information, severity and variety of symptoms, associated deformities, and procedures done for the second toe and associated additional procedures, such as hallux valgus correction and interdigital neuroma excision. We specifically identified the exact pathology (vertical or transverse plane instability), the grade of instability or dislocation at the MTPJ, and associated deformities necessitating correction, specifically on the second toe.
A total of 59 patients (64 feet; five bilateral) were examined, with an average followup of 45.2 (16 to 82) months, including five patients (five feet) who were evaluated by phone interviews. There were 50 women and nine men, and the average age of the patients at the time of the surgery was 59.5 (32 to 82) years. Right and left feet ratio was 40:24.
A cross-over second toe deformity was present in 56 feet (87%), with a stage II deformity (moderate deviation) in 18 feet, stage 1 (synovitis/mild deviation) in 10 feet, and stages III (overlap hallux) and IV deformities (total dislocation) in 14 feet each. 10 Seven feet had vertical subluxation or dislocation, and one had lateral deviation. Hallux valgus was present in 35 feet (54.7%), and hallux varus in three feet. Preoperatively, MTPJ pain was present in the second toe in 54 feet (84%), metatarsalgia of the second toe in 27 feet (42%), MTPJ swelling of the second toe in 19 feet, and neuritis in four feet. Callosities also were present in 22 feet. The causes of the second toe instability were evaluated, and although a definite pathology was not identified, there were the following associations, hallux valgus (27 feet), idiopathic instability (15 feet), a long second metatarsal (13 feet), acute trauma with no associated deformity (five feet), hallux varus (three feet), and postoperative deformity in one foot. 3,13
Conservative treatments such as orthotic arch supports or a looped toe splint were applied in 33 feet, a metatarsal pad was used in nine feet, and a cortisone injection was used in 17 feet. 7 Split FDL tendon transfer to the dorsum of the toe was done in all patients. The ends of the split FDL tendon were held with hemostat clamp and looped superficial to the extensor tendon and extensor hood, creating a knot on the dorsal aspect of the toe. 2 To produce ideal tension on the transferred tendon for optimal correction and to prevent over-tightness of the MTPJ, the knot was pulled under tension with the MTPJ in approximately 30 degrees of dorsiflexion and the ankle in neutral dorsiflexion. The tendon was secured with several sutures both to itself and to the extensor hood.
Additional surgery, including a complete dorsal capsulotomy of the MTPJ (63 feet), extensor digitorum longus (EDL) lengthening (49 feet), and collateral ligament release (54 feet), were done as required. 1 An oblique osteotomy of the second metatarsal head (Weil) was done in 29 feet (45%), a proximal interphalangeal (PIP) joint resection arthroplasty in 22 feet (34%), and a PIP joint fusion in nine feet (14%). At the time of surgery, if persistent subluxation or instability of the MTPJ was identified, the toe was immobilized with a 0.062-in Kirschner wire introduced across the MTPJ and removed between 2 and 3 weeks at which time range-of-motion (ROM) exercises of the joint were initiated. The MTPJ was stabilized with a Kirschner wire for an average of 2.5 weeks postoperatively in 49 feet (76%). 3,6 Hallux valgus surgery was performed concomitantly in 25 feet (39%) and included a distal chevron osteotomy (five feet), a Ludloff proximal metatarsal osteotomy (10 feet), a modified Lapidus procedure (six feet), and others (four feet). Interdigital neuroma resection was done simultaneously in 10 feet (15%), in the second web space in nine feet and third web space in one foot.
At final followup, the patients were carefully examined for their functional status, residual pain, stability and recurrence of the deformity, and satisfaction, specifically with regard to the second toe. The American Orthopaedic Foot and Ankle Society (AOFAS) forefoot score was additionally used. 12
Statistical Methods
Statistical analysis was done with the SPSS statistics program (Version 10.1, SPSS Inc., Chicago, IL), and the Student t-test was used to determine whether the toes treated with toe flexor-to-extensor tendon transfer and the Weil metatarsal head osteotomy had significantly better outcomes (AOFAS score) compared to the toes with flexor tendon transfer only. We also used a chi-square test to evaluate whether there were associations between preoperative toe deformities and postoperative MTPJ contractures.
RESULTS
At followup, residual second MTPJ pain was identified in 17 feet (27%) and was noted to be mild in seven, moderate in eight, and severe in two feet. After surgery, second MTPJ synovitis was found in 10 feet, second web space neuritis in eight feet, and second metatarsalgia in six feet. Of the eight feet with second web space neuritis, three had undergone prior neuroma surgery with the initial flexor tendon transfer. Of the 59 feet that were physically examined, 22 feet (37%) had residual second MTPJ dorsiflexion (DF) contracture (mild 15, moderate five, severe two), while 14 feet had PIP joint contracture (mild eight, moderate three, severe three), and 17 feet (29%) had distal interphalangeal (DIP) joint hyperextension deformity (mild 14, moderate three). Persistent medial deviation of the second toe was found in 16 feet (27%), and this deviation was mild in 12 feet, and moderate and severe in two feet each. Lateral deviation also was found in three feet (Figure 1). There was no statistically significant association between preoperative second toe deformity and the postoperative MTPJ dorsal contracture (p > 0.05).
The mean passive second MTPJ dorsiflexion angle with the ankle in neutral was 35 degrees, and 50 degrees with the ankle in 30 degrees of plantarflexion. A vertical stress test was done to examine the second MTPJ stability, and 46 of 59 feet (78%) were found to be stable, while 13 feet (22%) had persistent instability (11 mild, 2 moderate). The mean toe pulp to ground distance on standing was 2.9 mm (0 mm: 23 feet, 1 to 3 mm: 13 feet, 4 to 7 mm: 16 feet, 8 to 13 mm: seven feet), and strong toe grasp was possible in 45 feet (Figure 2).
As for morphologic improvement, the patients thought that the shape of the second toe improved in 33 feet (67%, 33 of 49), stayed the same as before in 10 feet, and became worse in six feet. Although additional forefoot surgery was done, this study focused only on the second toe and the evaluation and patient satisfaction were specifically directed. Twenty-six patients (29 feet, 45%) were very satisfied, 15 patients (15 feet, 23%) satisfied with minor reservation, six patients (6 feet, 9%) satisfied with major reservation, and 12 patients (14 feet, 22%) were unhappy with the outcome of treatment. Forty-one patients (45 feet, 70%) noted that they would have the surgery again under similar circumstances, and 40 patients (44 feet, 69%) would recommend the surgery to a friend, while two patients could not decide on the recommendation. The AOFAS functional score (59 feet) was an average 81.9 (47 to 100) points at final followup, which also was focused only on the second toe.
The average AOFAS scores between the toes with the Weil osteotomy and the toes without the Weil osteotomy did not show any significant difference (p > 0.05). There were 15 complications, which included recurrence of deformity (nine), toe infection (five), and second web space neuritis (one).
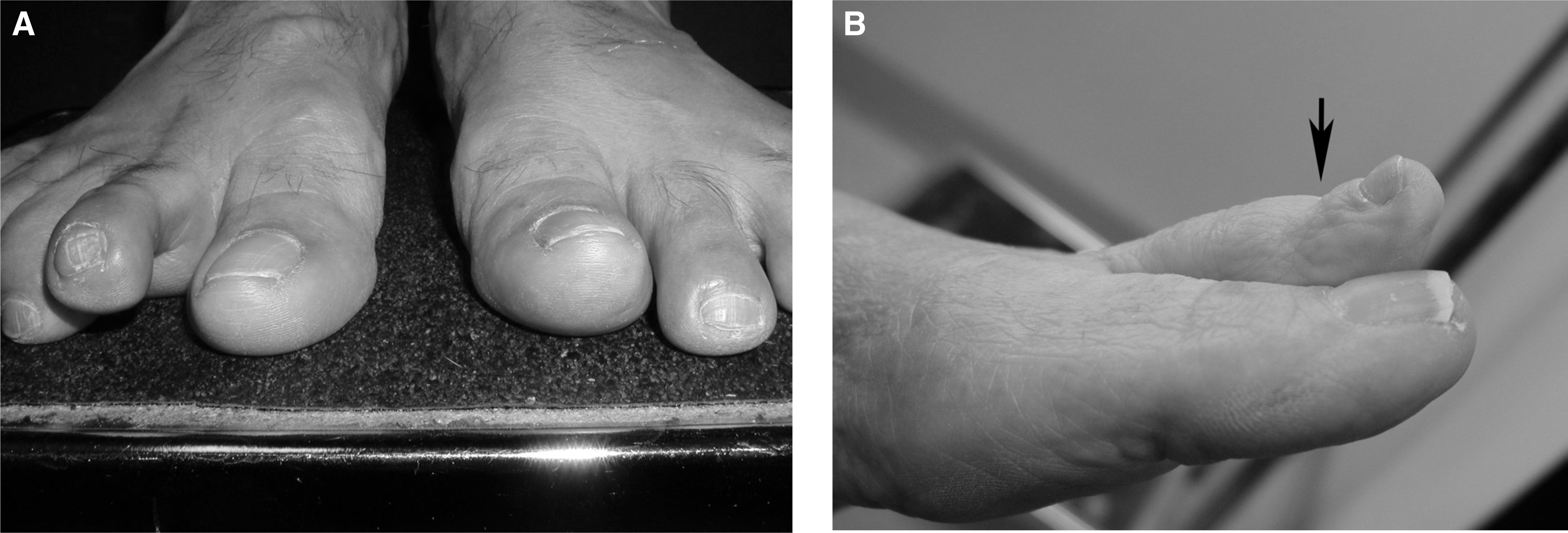
Residual second toe deformity

The mean toe pulp to ground distance on standing was measured at final followup to evaluate residual toe elevation.
DISCUSSION
Although the pathophysiology of second toe MTPJ instability is not entirely clear, it has been reported to be caused by factors such as second metatarsal overload, 11 a long second metatarsal, 3,6 and trauma, and these findings correlated with our group of patients. The literature supports a high association of hallux valgus with second MTPJ instability, 15 and the question arises as to the need for correction of asymptomatic hallux valgus albeit minor in the presence of second toe deformity. In our series, concomitant hallux valgus deformities were corrected but generally only in the presence of bunion pain, while Gazdag and Cracchiolo 8 recommended correction of an asymptomatic bunion that prevented adequate second toe correction. It is likely, however, that even asymptomatic hallux valgus deformity may require correction in the presence of a subluxated and deformed second toe unless the toe is amputated.
The association of second web space neuritis with second toe deformity and subluxation is controversial. In general, the neuritis may represent traction on the nerve as a result of the MTPJ subluxation. Although not confirming the presence of a pathologic neuroma, when confronted with a patient with distinct pain in the MTPJ as well as the web space, we attempted to confirm the diagnosis of interdigital neuritis preoperatively by injecting the affected web space with 1 cc of lidocaine. The incidence of concurrent second web space interdigital neuritis of 10% may seem high; however, for each patient in this series the resected nerve was sent for pathologic examination and confirmed as such in each instance. At final followup evaluation, we carefully documented the presence of the combined interdigital neuritis and differentiated them from MTPJ synovitis or metatarsalgia. The high incidence of neuritis (eight of 64 feet) after surgery was a notable concern, including three patients who had resection of an interdigital neuroma simultaneously.
Our results reflected that achieving physiologically normal alignment of the second toe was realistically difficult. Thirty-seven percent of patients had residual second MTPJ dorsiflexion contracture, while 32% also showed persistent medial or lateral deviation of the second toe. It also is important to note that we examined the DIP joint hyperextension deformity, caused by loss of the DIP joint flexor function. We also checked the MTPJ dorsiflexion angle with the ankle in 30 degrees of plantarflexion (PF), to reproduce the DF angle that is typically required during the late stance phase of gait. As for the MTPJ stability to vertical stress manipulation, the stiffness caused by scar tissue may have been partly responsible for the stability of the MTPJ, since some second toes with residual radiographic subluxation of the MTPJ were still found to be quite stable to stress testing. 8
An alternative tendon transfer for managing transverse plane instability is the extensor digitorum brevis (EDB), which has been reported to be more appropriate for stages I and II crossover toe deformities. 10 Although the EDB procedure was used concurrently for other patients who were not compared with this cohort, it is not clear whether the flexor-to-extensor tendon transfer is better for more advanced deformities. It is also not clear whether the Weil osteotomy of the second metatarsal alone (performed in 45% of these patients) would be sufficient to stabilize the MTPJ. Common sense would dictate that if a toe is unstable, a shortening osteotomy alone may not be sufficient to control this instability. However, this was not a concept that we could prove, since it was not compared with a group of patients who were only treated with osteotomy for a similar deformity. Before the use of the Weil osteotomy, we performed a collateral ligament release and Kirschner wire fixation to keep the toe aligned, but this was not successful in most patients even with a more prolonged period of Kirschner wire immobilization, with frequent recurrence of the varus deformity. One interesting fact in these patients, however, was the presence of radiographic subluxation in some asymptomatic patients after the Weil osteotomy, and it is possible that scarring associated around the MTPJ may have contributed to the stability as well as the tendon transfer.
It is important to note that the evaluation of the results in this study was focused solely on the second toe, and although not all patients had excellent results from the hallux valgus correction, these did not factor in the outcome reported here.
One of the reasons for patient satisfaction in this series was the relief from the synovitis caused by stretching of the capsule and the associated plantar plate injury, as well as relief of dorsal PIP toe pain. Functional improvement and increased activity levels were mainly due to relief of pain (MTPJ pain, metatarsalgia, PIP dorsal rubbing pain), and not from restoration of the toe function. Many patients with poor results (low AOFAS score) had postoperative MTPJ pain and residual MTPJ contracture to some degree, but more frequently pain. Although the functional assessment score was relatively high (82 points), a high percentage (32%) of the toes still had persistent medial or lateral deviation, which also correlated with previous reports of a high incidence of residual toe deformity. 8 As far as patient dissatisfaction is concerned, contracture and stiffness of the toe were more of a problem than pain. Although pain relief after surgery was profound in most, many of these patients were still dissatisfied with a poor looking and poor functioning straight stiff toe that they described as a “dead toe” or a “dead stick,” and indeed 32% of the patients replied that the toe did not improve or got worse morphologically after surgery.
The toes did not bend at the DIP joint because of the FDL transfer, and the remaining flexor function did not seem to be sufficient for certain activities, including wearing certain types of shoes and performing certain exercises, such as yoga, and some patients who were active runners complained of soreness. This toe stiffness was exaggerated when the patients tried to grasp an object with the toes or tried to wear sandals. Moreover, residual toe elevation from the dorsal incision scar contracture aggravated the aesthetic appearance, increasing the patient's dissatisfaction. The satisfied patients (68%) as a group had a well corrected and stable second toe with minimal dorsal toe elevation or mediolateral deviation, minimal toe discomfort, and good toe grasp power.
Although the AOFAS score at final followup was high, a high percentage of patients (22%) were dissatisfied with the outcome of surgery, and clearly this score did not correlate well with the outcome of treatment, nor did it reflect the true functional status of the second toe with MTPJ instability. Thirty percent in our series lacked toe-to-ground contact with toe grasp, while Thompson and Deland 15 reported 100% postoperative toe-to-ground contact. About 32% were dissatisfied or satisfied with major reservation with a relatively low satisfaction rate compared to the previous reports. 4,8,15 Coughlin reported a high satisfaction rate (71%) among athletes, while Thompson and Deland reported a 92% satisfaction rate in their series, 5,15 which we could not support in this study. Clearly, a limitation of the findings of this study were the secondary procedures carried out with the toe flexor-to-extensor transfer, which makes clinical outcome assessment of the flexor tendon transfer as a specific procedure difficult.
To minimize the residual toe elevation, adequate EDL lengthening and dorsal capsular and ligamentous release should be emphasized. Interestingly, for some patients, the residual toe elevation deformity, though cosmetically disappointing, was perceived as somewhat advantageous in wearing high heel shoes, but this cannot possibly be a positive finding in which some toe dorsiflexion is required to slide the foot into the toe box.
Although the function of the second toe improved in most patients as a result of pain relief, a substantial number of the patients in this study remained dissatisfied or satisfied with major reservations because of residual stiffness of the toe, loss of active flexion, and generalized dysfunction of the toe. The flexor to extensor tendon transfer may have some relevance in correction of second toe instability but must be used with caution and a full understanding of potential complications and patient dissatisfaction. Clearly, the isolated second toe deformity does not have a simple solution, and more extensive study of this subject is warranted.