
Abstract
Background: Conventional treatment for tibiotalar joint arthritis relies on arthrodesis or prosthetic arthroplasty. Fresh osteochondral allografting is an alternative procedure to replace diseased articular cartilage. Methods: Eleven patients (average age 43 years; range 18 to 65 years) had fresh osteochondral grafting of the tibiotalar joint. The diagnoses were posttraumatic arthritis in seven ankles, osteoarthritis in two, and an osteochondral defect in two. Precise cuts were made using the Agility® (DePuy, Warsaw IN) ankle arthroplasty jigs. Bipolar replacements were used in nine ankles and unipolar in two. Results were evaluated using outcome scores, physical examinations, and standing ankle radiographs.Results: At a minimum followup of 24 (average 33; range 26 to 45) months, six of the 11 ankles had successful grafting procedures. The average AOFAS score preoperatively improved from 55 to 73 postoperatively (p = 0.01). The patients' pain, gait, and walking surface scores were all significantly improved (p < 0.05). Of the five failures three underwent successful repeat allografting and one was revised to a total ankle arthroplasty, and one has had no further surgery. The ankle range of motion arc was 30 degrees or more in six ankles. Additional surgery included five talofibular joint debridements, three repeat graftings, two hardware removals, and one conversion to a prosthetic ankle replacement. There was one intraoperative fibular fracture and one superficial wound infection. The serum of 10 patients tested positive for cytotoxic HLA antibodies postoperatively. Radiographs revealed moderate and severe joint degeneration in six ankles; however, this did not necessarily correlate with a poor outcome. Poor results tended to occur in ankles with a graft-host size mismatch or graft thickness of less than 7 mm. Conclusion: Fresh osteochondral transplantation for tibiotalar joint arthritis is a promising alternative to arthrodesis and prosthetic replacement. Early results demonstrate successful outcomes and good pain relief in over half the patients in this series.
INTRODUCTION
Arthritis in the tibiotalar joint of young or active individuals remains a challenge in modern orthopaedic practice. The goal of treatment is to provide a well functioning ankle that can endure a wide range of activity. The experience with total ankle arthroplasty has demonstrated early loosening and poor long-term outcomes. 22,24 Arthrodesis provides satisfactory relief of pain but creates undesirable functional limitations and leads to the development of arthritis in adjacent joints. 8,27,29,30,35,38
The use of fresh osteochondral allografting as an alternative procedure to replace diseased or damaged articular cartilage has been well documented for several decades. 2,3,6,7,9,11,13–15,28,31,33,34,39 Studiesonallogenic cartilage transplantation have shown this tissue to be immunologically competent and have demonstrated a high percentage of surviving chondrocytes several years after implantation. 10,25,26,32,36 Tissue matching between the host and donor grafts is not required because the matrix that surrounds the chondrocytes protects them from the immunocompetent host cells. 25,26 Although the potential for disease transmission exists with the use of any allogenic tissue, the risk with osteochondral allografts is low when adequate precautions are taken. 4
A recent study by Kim et al. 19 examined the results of fresh tibiotalar osteochondral allografts in seven patients with post-traumatic ankle arthritis. Four of the seven had good or excellent results, and three had poor results, all of which were attributed to technical errors that resulted in poor graft fixation and nonunion. They also described a revised surgical technique using the Agility® (Depuy, Warsaw IN) ankle arthroplasty cutting jigs and alignment system to allow more precise size matching and improved fit. This resulted in improved stability and incorporation of the graft.
The purpose of the present study was to determine the short-term results in the largest series thus far of fresh osteochondral allografts for tibiotalar joint arthritis using the revised operative technique as described by Kim et al. 19
MATERIALS AND METHODS
A fresh osteochondral allograft program was established at our institution in 1983 after institutional review board approval. Between 1999 and 2001, 11 patients (six females and five males) had fresh osteochondral allograft transplant into the tibiotalar joint with the use of the Agility® (Depuy, Warsaw, IN) total ankle instrumentation (Table 1). Bipolar (both surfaces) replacements were done in nine ankles and unipolar (one surface) in two. The senior two authors (MB and WB) performed all surgeries as a team. The average age of the patients was 43 (range 18 to 65) years. The diagnoses were post-traumatic arthritis in seven ankles, osteoarthritis in two, and an osteochondral defect in two. Conventional means of controlling pain had been unsuccessful in all patients. Informed consent was obtained from all patients after extensive discussions about the various risks, benefits, and alternatives to fresh osteochondral allografting.
Patients were evaluated before surgery by means of physical examination, weightbearing radiographs, and the American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot score. 20 At a minimum of 24 (average; range 26 to 45) months after surgery, all patients were contacted and examined clinically, and weightbearing radiographs of the ankle were obtained. Patient outcomes were evaluated with the AOFAS hindfoot score, the Foot Function Index (FFI) score, and the Short Musculoskeletal Function Assessment (SMFA) questionnaire. 5,43 Two patients (cases one and eight) who could not return for followup because of geographical constraints were examined by a local orthopaedist, and the questionnaires and radiographs were returned by mail.
Followup radiographs were evaluated for graft nonunion, fragmentation, collapse, resorption, and degenerative changes. Joint degeneration was recorded as mild, moderate, or severe. Radiographs were classified as mild when more than 50% of joint space was maintained, with no subchondral sclerosis or osteophytes. Moderate changes involved collapse of more than 75% of the joint space, mild subchondral sclerosis, and one or two osteophytes. Severe degenerative changes involved complete loss of joint space, subchondral sclerosis, and multiple osteophytes. 2,12
The transplanted graft was considered to have failed when the patient required additional surgery (repeat allografting, total ankle arthroplasty, or arthrodesis) or had severe degenerative changes on followup radiographs and an AOFAS score of less than 70. Patients who had surgery for simple arthroscopy, hardware removal, or joint debridement, were not considered to have grafts that failed.
Preoperative and postoperative AOFAS scores were analyzed using paired t-tests. Pain, activity limitations, walking distance, walking surfaces, gait abnormality, sagittal and hindfoot motion, alignment and stability, and preoperative and postoperative AOFAS scores also were compared using paired t-test analysis. Statistical significance was set at p < 0.05.
Serum anti-HLA antibodies were measured before surgery and 6 months after surgery to monitor the immunologic response to the allografts. The significance of a response and its effect on outcome were examined. Osteochondral allografts were obtained from fresh cadavers of individuals meeting the criteria of the American Association of Tissue Banks. 18 A regional tissue bank supplied the grafts for all patients. Allografts were harvested within 24 hours of death and were transplanted fresh within 7 days from the time of procurement, except for the last two patients in the series (24 days). Because of heightened screening measures, grafts can no longer be released in less than 3 weeks. 46 The average age of the donors was 27 (range 16 to 45) years, and all were matched to the same sex host except in case one. Grafts were placed in sterile plastic bags and immersed in Ringer's lactate solution containing 1 gm cephalothin and 10 mg of gentamicin per liter. The sterile plastic bags were placed in sterile jars and stored at 4 degrees C until they were used. Specimens were cultured and tested for antibodies to HIV, syphilis, and hepatitis.
The patients were matched with a donor allograft on the basis of size. No tissue or blood type matching was done. The mediolateral width of the talus, 0.5 cm below the talar dome, on the anteroposterior (AP) weightbearing ankle radiograph after correction for magnification, was used to size-match the host to the graft. A match was considered to be a size difference of 1 mm or less. Candidates were then placed on a waiting list until an appropriate size donor became available.
The technique of implanting fresh osteochondral allografts in the tibiotalar joint involves two surgical teams, one for the graft preparation and the other for the recipient surgery. The operative procedure used was that described by Kim et al. 19 and Tontz et al. 44 Equinus contracture was treated with either a percutaneous Achilles tendon lengthening or gastrocnemius recession. All ankles had more than 10 degrees of ankle dorsiflexion with the knee straight at the end of the procedure.
Demographic and clinical data
Denotes graft obtained from same donor.
Patients were restricted from weightbearing for 12 weeks, but range-of-motion exercises were started once the incisions were healed. Motion exercises were delayed for 6 weeks if the patient had Achilles tendon lengthening. At 3 months patients began protected weightbearing in a cam boot for 1 month. Full activity, with the exception of running, was allowed at 6 months.
RESULTS
Six ankles of the 11 ankles had successful grafting procedures (Figure 1). The average AOFAS score improved from 55 (range 36 to 70) preoperatively to 73 (range 41 to 100) postoperatively (p = 0.01) (Table 2). Clinical AOFAS scores were greater than 70 in eight patients. Pain, gait, and walking surface scores were all significantly improved (p < 0.05). The ankle range of motion arc was 30 degrees or more in these six patients. The average FFI and SMFA scores were 3.6 (range 0 to 7.4) and 18.1 (range 17.1 to 51.6), respectively, at the most recent followup.
Five allografts were classified as failures. Three of these ankles had repeat allografting. Case two had revision bipolar allografting at 33 months, with a successful result 12 months after repeat surgery. Case four had revision bipolar allografting for a failed unipolartibial graft at 20 months postoperatively and had a satisfactory result at 13 months after revision surgery. Case three recently had repeat bipolar allografting at 36 months and is satisfied with the outcome. One patient (case 11) had a total ankle prosthetic replacement at 18 months with a good result. Case 5 had a severe graft collapse at 12 months postoperatively but has required no further surgery. No ankle had an arthrodesis.
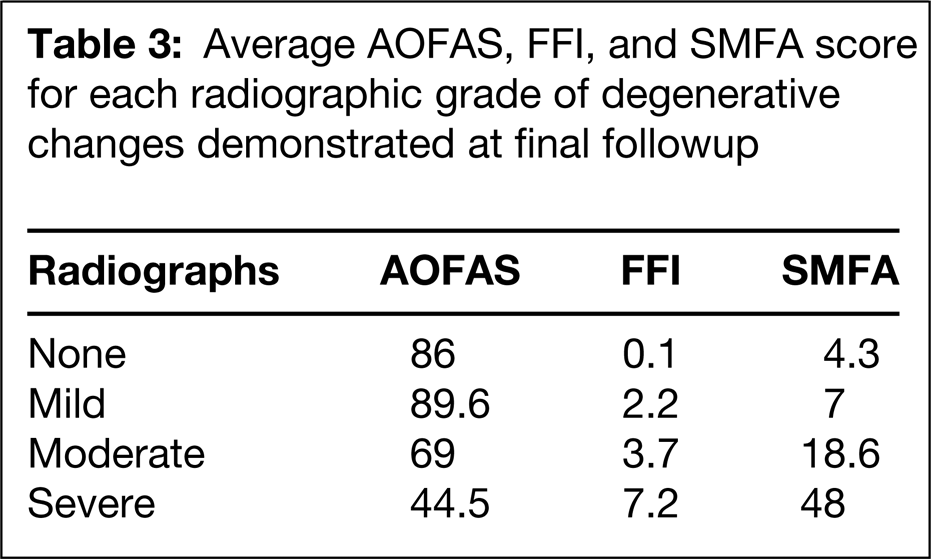
Complications included one intraoperative transverse fibular fracture created while making the transverse tibial cut with the cutting block and one superficial wound infection that resolved with oral antibiotics. Additional surgery was required in seven patients and included talofibular joint debridement (five patients) (Figure 2) revision bipolar allografting (three patients), hardware removal (two patients), arthroscopic ankle debridement (one patient), and total ankle arthroplasty (one patient). Radiographic union was present in all grafts by 3 months after surgery. Joint degeneration was classified as none in two, mild in three, moderate in four, and severe in two patients. Degenerative changes on radiographs were compared with the AOFAS, FFI and SMFA scores (Table 3). Although some patients with moderate degenerative changes had good outcome scores, generally the scores decreased in patients who were classified as having severe degenerative changes.
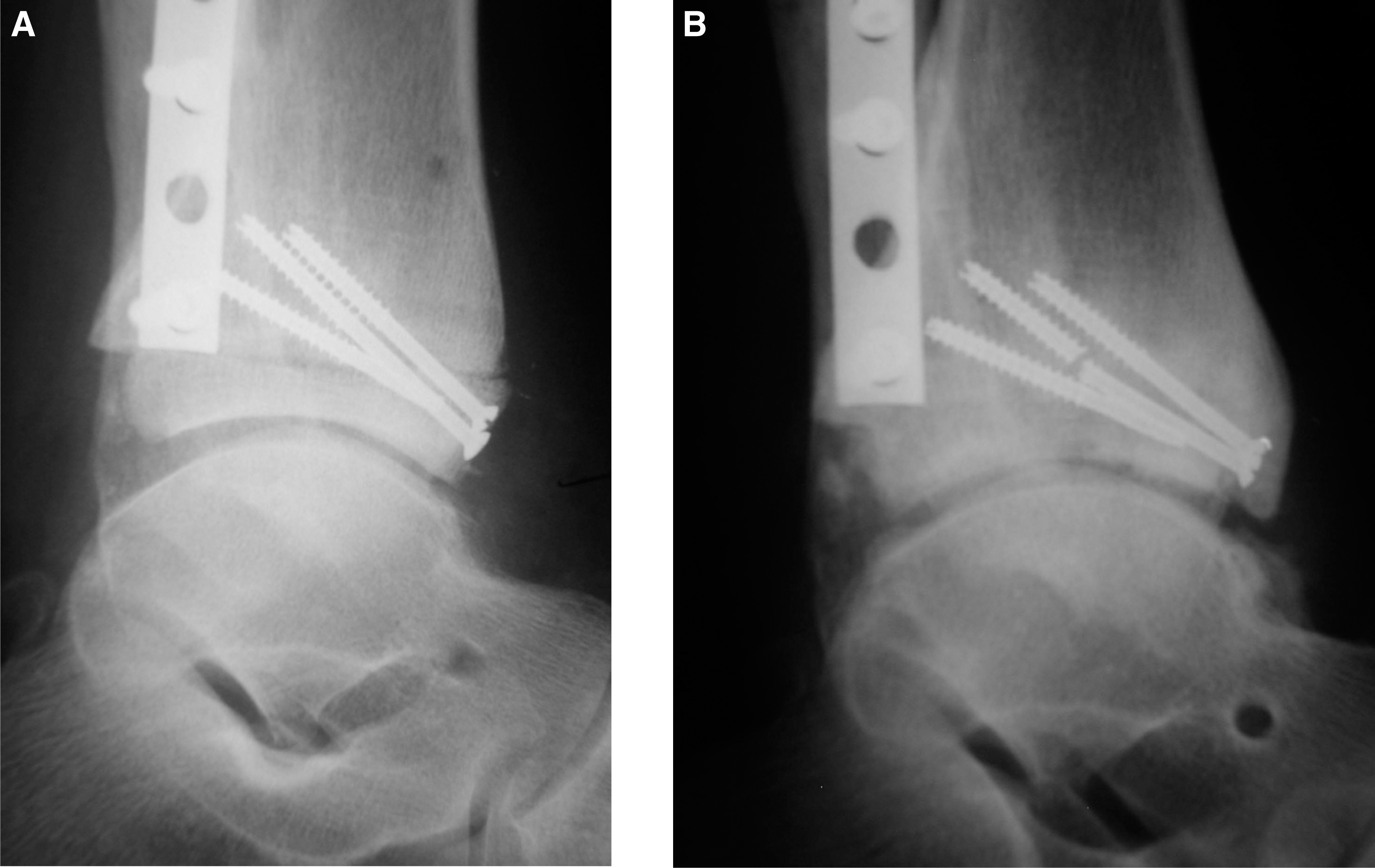
Cytotoxic serum HLA-antibodies were positive in all but one patient (case seven) at 6 months postoperatively. Case seven, a kidney transplant recipient, was taking immunosuppressant medications daily (cyclosporine and prednisone). Her radiographs showed no evidence of collapse and her outcome scores were excellent (Figure 3). Case eight received the opposite side graft from the same donor as case seven, and her radiographs displayed mild degenerative changes, but her result was excellent as well.
DISCUSSION
The treatment of tibiotalar arthritis in younger, active individuals remains a challenge. Traditionally, arthrodesis has given patients predictable pain relief at the cost of functional limitations and the risk of developing arthritis in adjacent joints. Hindfoot arthritis has been reported in more than 50% of patients at an average of 8 years after ankle arthrodesis and in nearly 100% at 20 years. 8,27,29,30,35,38 Recent advances in total ankle replacement are promising; however, the long-term results in younger patients remain unproven, and reoperation rates are high. 1,37,40 The usefulness of fresh allograft transplantation for the treatment of arthritic defects in the knee and hip joint is well established. 2,3,7,9,11–15,28,31,33,34,39 In the knee, single surface grafts have demonstrated 70% to 85% and bipolar replacements 50% to 60% success at up to 10-year followup.
In the present study, the largest to date on the use of fresh osteochondral allografting for the treatment of tibiotalar arthritis, early outcomes were successful in over half the patients. Although our outcomes were not as successful as historic controls involving arthrodesis or prosthetic arthroplasty, further refinement in osteochondral allografting as a treatment for arthritis should improve results. 8,22,24,27,29,30,35,38
Of the five ankles with failed allografts, three have undergone repeat grafting, one was converted to a total prosthetic arthroplasty, and one has had no further treatment. Although no ankles underwent conversion to an arthrodesis, Kim et al. 19 reported no difficulties in revision of two failed ankle allografts to arthrodeses. In this report, allografting may be a conservative procedure because it does not preclude repeat allografting, conversion to a total ankle arthroplasty, or tibiotalar arthrodesis.
The use of fresh osteochondral allografting as a biologic alternative for resurfacing the tibiotalar joint is based on two important properties of bone and cartilage. The use of fresh tissue assures the transplantation of a high percentage of surviving chondrocytes in the articular cartilage. 10 Living chondrocytes, in turn, support the intact cartilage matrix. A thin layer of subchondral bone is transplanted to provide a mechanism for graft fixation. The allograft bone is slowly incorporated and replaced by the host bone through a process of creeping substitution. Revascularization may take from 1 to 4 years, depending on the size of the allograft and the quality of the host bone. 31 During revascularization of the allograft the bony structure is weak and vulnerable to collapse.
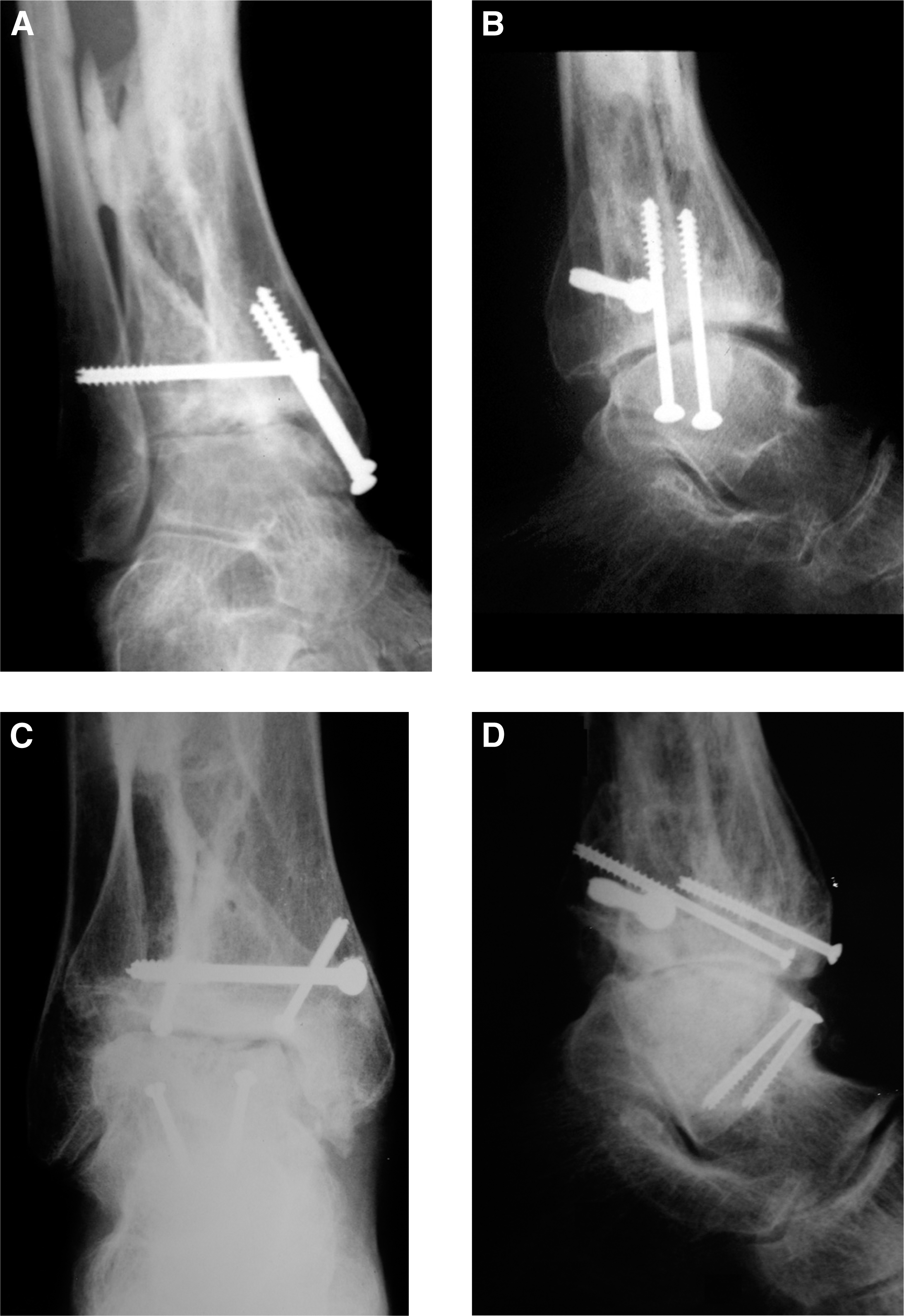
Case 1, a 45-year-old female with post-traumatic arthritis after treatment for an open distal tibial fracture.
Radiographic and outcome scores

Failures

Case 3, a 56-year-old female with painful talofibular joint arthritis at 9 months after total tibiotalar joint fresh allografting.
Average AOFAS, FFI, and SMFA score for each radiographic grade of degenerative changes demonstrated at final followup
The disadvantages of the fresh allografting technique include the difficulty in obtaining donor tissue and the logistics to safely harvest, screen, and transplant within an acceptable time. Chondrocyte viability studies have demonstrated 70% survival at 4 weeks when grafts are stored in culture media at 4 degrees C. 46
Transmission of disease from the donor to the recipient remains a significant concern despite adherence to the guidelines of the American Association of Tissue Bank. 18 Although we have had no documented occurrences to date, we counsel prospective recipients of fresh allogenic bone that the risks of disease transmission are similar to those of homologous blood transfusion. 4
Although it has been suggested that articular cartilage is relatively immunoprivileged, with the matrix protecting the chondrocytes from the immunocompetent host cells, the marrow elements within the transplanted bone are not. 25,26,42 Animal studies have suggested the need for cross matching donor and recipient tissues, 26 but the immunologic response to unmatched allografts has not yet been shown to be of clinical significance. 10 All but one (case six) of our patients tested positive for the serum HLA cytotoxic antibody. Interestingly, case six was on immunosuppressant medication daily for a kidney transplant. Her radiographs and clinical outcomes scores proved to be the most successful in the cohort of patients. Case seven received the opposite side from the donor, and although she had an excellent result overall, her radiographs demonstrated mild degenerative changes. Possible reasons for this could be that a perfect tissue cross-match occurred by chance, or the humoral antibody response plays a more important role than previously thought, or the effects of the immunosuppressant agents dampened her immune response to the graft. Although the current literature suggests that immunosuppressant medication is not required in patients receiving unmatched osteochondral allografts, our observation of case six leads us to speculate that the immune response may play a more important role in graft survival than previously thought.

Case 7, a 65-year-old female with painful ankle arthritis. She is also a kidney transplant recipient who takes immunosuppressant medications daily (cyclosporine and prednisone).
Reports on the use of fresh osteochondral allografts in the ankle remain few. Gross et al. 16 reported a series of nine patients with displaced osteochondritis dissecans lesions of the talar dome treated with fresh osteochondral allografts. All were single surface grafts of the talar side only. At an average followup of 11 years, six patients had successful outcomes and three were converted to arthrodeses. In the present study (case seven) one of two unipolar surface replacements was successful. The other (case five) was revised at 20 months to a bipolar graft with a good outcome at 1 year.
Kim et al. 19 examined the long-term outcomes of bipolar tibiotalar fresh osteochondral allografts in a small series of seven patients with posttraumatic ankle arthritis. Four of the seven had good or excellent results at an average followup of 12 years. Radiographs revealed joint space narrowing, osteophytes, and sclerosis even in those with good clinical outcomes. Two patients later had arthrodeses without difficulty. Complications were mostly related to technical deficiencies associated with graft implantation, including poor graft fit, graft subluxation, and nonunion. The use of cutting blocks and precise size matching helped reduce the number of technical errors.
Of the five graft failures in our series, two (cases two and four) had grafts less than 7 mm thick, resulting in early graft fragmentation and collapse (Figure 4). Both patients had repeat grafting with good results at 1 year. Case eleven had transplantation of a graft that was grossly undersized (Figure 5). The measurement preoperatively was 31 mm compared with the actual donor talus width of 29 mm. Case eleven was converted without difficulty to a total ankle arthroplasty and is now 7 months from surgery with a good result. Finally, cases three and five had graft failures despite what appeared to be technically well implanted, correctly size matched donors. Case five did receive a graft from the oldest donor in our series (45 years). Case three had repeat grafting at 36 months with good results at 6 months.
Five ankles required debridement of the talofibular joint because of continued lateral ankle gutter pain after surgery, a fairly high percentage in a series this size. Our technique does not include resurfacing of this joint. Currently, we make an effort at the time of surgery to remove any osteophytes in this joint after the graft is implanted. Some ankles may develop lateral ankle pain (calcaneofibular) as a result of the graft settling. It is well documented in the literature that allografts lose 1 to 2 mm of height, possibly more, depending on the stresses applied. 2,9,31,34,39 We believe the combination of talofibular arthritis and graft settling were the likely causes of the frequency of lateral ankle gutter pain that required debridement.
The ultimate fate of fresh osteochondral allografts for tibiotalar joint arthritis remains unknown. Because it is difficult to predict whether an allograft will alter the natural history of an arthritic joint, this procedure is considered an interim procedure before a likely arthrodesis or prosthetic replacement. The major advantage of this procedure is that it does not preclude repeat allografting or conversion to a total ankle arthroplasty or an arthrodesis. Revision operations after allografting are not as difficult technically as the literature suggests after failed ankle replacement surgery. 17,21,23,41,45 In contrast to a failed total ankle replacement, bone stock is maintained after allografting, and conversion to an arthrodesis, in theory, should not be as demanding.
Case 4, a 31-year-old male who had a unipolar fresh allograft replacement of the tibial plafond only.
Although seven of our 11 patients required further surgery, four of which were revisions or total ankle arthroplasty, we believe these numbers are not unreasonable given the relatively young age (average 42 years) of these seven individuals. A recent study of complications after total ankle arthroplasty found a higher revision rate in younger patients. 40 Their 5-year survival with reoperation as an endpoint was 54%. We believe our reoperation rate compares favorably with that in patients under 50 years who have total ankle arthroplasty.
We offer fresh osteochondral allografting as an alternative treatment for selected individuals with end-stage tibiotalar arthrosis. The ideal candidate is a young person with no deformity and good ankle motion who is not willing to accept the functional limitations that come with an ankle arthrodesis. Long-term results in other studies have proven the effectiveness of fresh osteochondral allografting as a biologic resurfacing technique for both focal and widespread articular cartilage disease. 16,19 Our modest success in over half of our patients, with significant improvements in pain relief, is similar to other studies of bipolar allografting. 9,14,34 We continue to view this procedure as an alternative to arthrodesis or arthroplasty in individuals with advanced arthritis. Further refinements in surgical techniques and better understanding of the biology of fresh osteochondral transplantation hold promise for improved clinical outcomes in the future.

Case 11, a 53-year-old female who underwent a bipolar fresh allograft replacement for posttraumatic ankle arthritis.