Abstract

INTRODUCTION
Arthrodesis of the first metatarsophalangeal (MTP) joint is commonly used in the treatment of severe hallux rigidus, 4 and recurrent hallux valgus, 3,5 providing good results. 1 It is important to position the proximal phalanx properly when performing an arthrodesis. Too much plantarflexion leads to overloading of the great toe, ulceration, interphalangeal joint osteoarthritis and difficulty executing the toe-off phase of stance. Patients tolerate excessive dorsiflexion poorly because of dorsal impingement and difficulty with footwear. Both, however, are recognized complications of first MTP joint arthrodesis.
Techniques that can be used for revision of an excessively dorsiflexed arthrodesis include a dorsal opening wedge osteotomy packed with bone graft before fixation with a small fragment plate or crossed screws, a plantar closing wedge osteotomy, a crescentic osteotomy, 2 or trapezoid osteotomy. All of these techniques require technical expertise to attain an appropriate MTP joint dorsiflexion angle.
Dorsal opening wedge osteotomy fixed with a small fragment block plate is a technically less demanding procedure than other common techniques and reliably allows accurate reduction and stable fixation for revision of first MTP joint arthrodesis.
Dorsal opening-wedge, plantarflexion osteotomies were done on one woman and one man who had sagittal plane dorsiflexion malunions of the first MTP joint. Both patients complained of excessive dorsiflexion producing dorsal impingement and difficulty in finding comfortable footwear. The male patient was 63 years old; his primary arthrodesis was done 18 months earlier with a single screw technique. The female patient was 48 years old; her primary arthrodesis was fixed with screws 19 months before revision surgery. Both had uncomplicated unions of their primary arthrodesis.
The patients were followed between 16 weeks and 6 months postoperatively, the endpoint for followup being clinical and radiographic union and patient satisfaction.
OPERATIVE TECHNIQUE
The incision incorporated the scar from the primary arthrodesis. A full-thickness skin flap was raised, and subperiosteal dissection exposed the arthrodesis site. The screws used in the initial fusion were removed. An osteotomy was made with a power-saw from dorsal to plantar, taking care to preserve a plantar cortical bridge. A fine osteotome was passed into the osteotomy site in a dorsal to plantar direction, and a second fine osteotome was introduced parallel to this. The osteotomy site was carefully opened using the osteotomes as levers around the plantar cortical hinge. The dorsal base of the opening wedge was measured once the corrected MTP joint angle was achieved, and the appropriate sized plate was selected, and applied adjacent to the osteotomes, which were then removed, the osteotomy being held open by the block. Correction was confirmed before final fixation of the plate with bi-cortical screws (Figure 1). The wedge was packed with morsellized bone graft harvested from the calcaneus or medial cuneiform.

Inraoperative photograph of small fragment plate in place.
The wound was closed in two layers with absorbable suture. A plaster cast with a toe extension was worn for 6 weeks, after which a firm-soled shoe was used. The wound was inspected at 2 weeks. Radiographs were taken immediately after surgery and at 6 weeks.
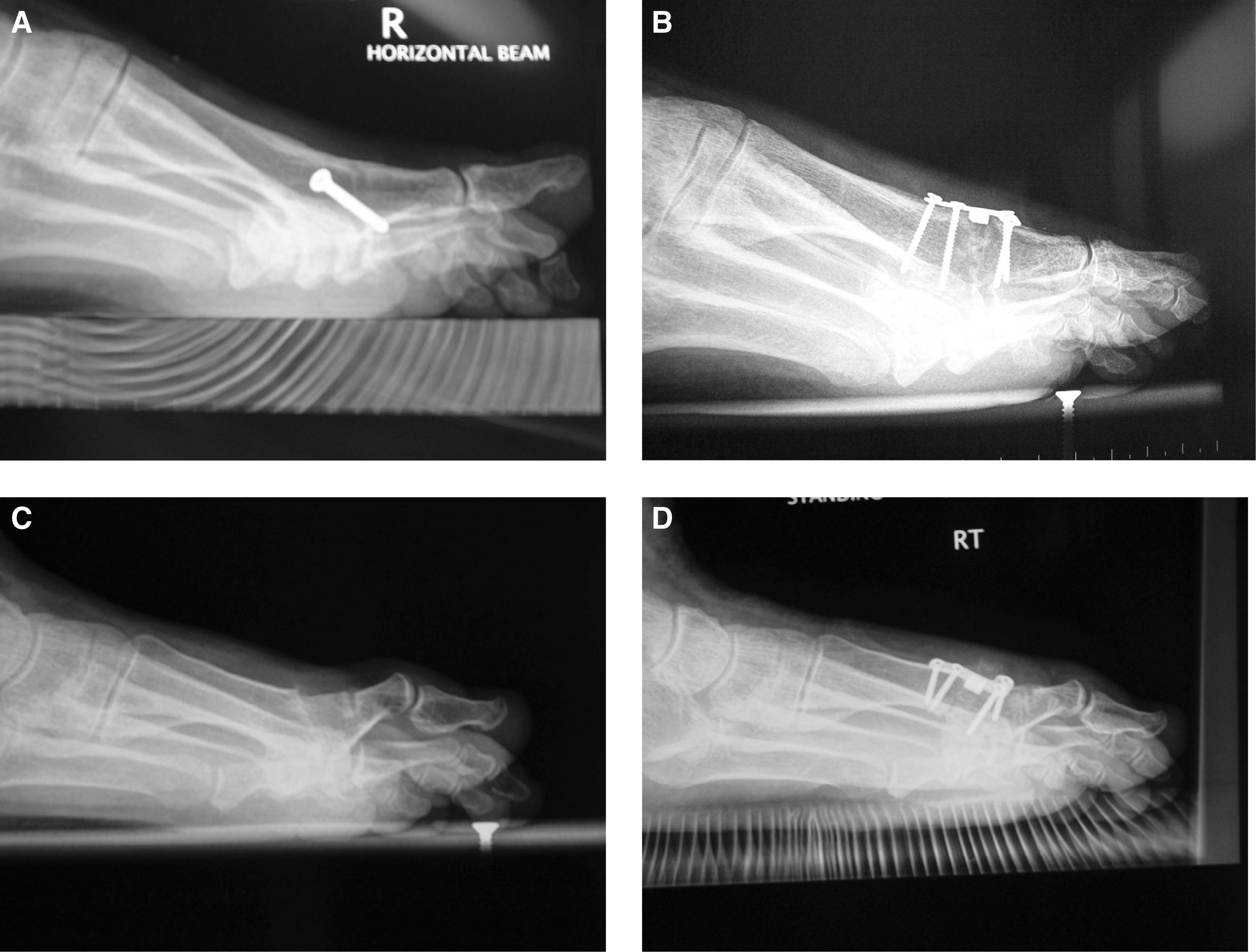
There was radiographic evidence of union in both patients at 6 weeks, with no wound complications, no implant failure, or loss of initial fixation, the plate and screws were not palpable. Postoperative MTP angles in the sagittal plane (Figure 2) were 17 degrees (31 degrees preoperatively) and 12 degrees (32 degrees preoperatively). Both patients reported subjective improvements in the position of the hallux and there was resolution of their symptoms. They were both able to wear normal footwear with no requirement for orthotic support. Both patients returned to work 8 weeks after surgery.