
Abstract
Background: The modified Jones procedure is the traditional operative procedure for correction of a clawed hallux, although the deformity may be caused by over-pull of one of three different muscles. In this study we present the radiographic and functional outcomes of flexor hallucis longus (FHL) tendon transfer as treatment for clawed hallux. The transfer is performed by drawing two thirds of the FHL tendon up through a drill hole in the proximal phalanx and then suturing it medially back to the remaining third. Methods: We retrospectively identified 19 patients (22 feet) who had FHL tendon transfer for correction of clawed hallux over a period of 5 years. Followup was an average of 51.0 (range 6 to 74; ± 3.8) months after the procedure. Outcome and patient satisfaction were determined using the Long-Form Musculoskeletal Function Assessment (MFA) score. Patients were asked whether they were satisfied, somewhat satisfied, or dissatisfied with the overall outcome and were asked about shoewear limitations. Preoperative and postoperative radiographs were evaluated in 15 patients (17 feet). We measured the hallux valgus and interphalangeal (IP) angles on the anteroposterior (AP) radiographs. On the lateral view we measured the angle of the IP joint, the metatarsophalangeal (MTP) joint, and the talometatarsal angle. Statistical analysis was done using a repeated measures ANOVA (p < 0.05). Results: On the lateral radiographs, the hallux IP joint angle (p < 0.0012; n = 15) and hallux MTP joint angle (p < 0.0265; n = 15) were significantly reduced postoperatively. On AP radiographs, the hallux valgus angle (p < 0.0334) was significantly reduced; however, the IP angle and the talometatarsal angle were not significantly different after surgery. Patients had an average MFA score of 14.6 (±3.8 standard error, range 1 to 35; n = 19). Thirteen patients were fully satisfied and six were somewhat satisfied with the overall result of the surgery. Four patients thought that their hallux limited the types of shoes they could wear, while 15 did not. Conclusion: It has been shown that clawed hallux can result from excessive motor function in one of three muscles: FHL tendon, peroneus longus (PL), and extensor hallucis longus (EHL). This study suggests that transfer of part of the tendon of the FHL is an effective alternative operative procedure for correction of clawed hallux.
INTRODUCTION
Clawed hallux is a deformity of the great toe generally attributed to muscular imbalance 4,5 and intrinsic muscle weakness. 1,6 Clinically, clawed hallux, or claw toe, is observed as first metatarsophalangeal (MTP) joint extension combined with interphalangeal (IP) joint flexion. The modified Jones procedure has been traditionally used for correction of clawed hallux. This procedure involves the transfer of the extensor hallucis longus (EHL) tendon to the neck of the first metatarsal of the hallux with fusion of the IP joint.
Many studies have speculated upon the mechanism and muscle groups primarily involved in the imbalance causing clawed hallux. Giannini et al. 5 in a 1985 study stated that the flexor hallucis longus (FHL) muscle and extensor hallucis brevis (EHB) muscle are contributory and aggravating factors for the deformity but are not directly responsible. Recently, however, Olson et al. 11 quantitatively demonstrated the effects of excessive force of three extrinsic muscles of the first ray on cadaver feet and found that the EHL and FHL muscles are primarily responsible for the angular changes resulting in clawed hallux, with the peroneus longus (PL) muscle contributing to increased plantar pressure beneath the first metatarsal. These findings suggest that successful corrective procedures for clawed hallux depend on manipulation of the EHL, FHL, or PL, or a combination of these muscles. EHL transfers, i.e. the Jones and modified Jones procedures, have been well described. 1,2,4,5,6,10,12 Transfer of the PL to the peroneus brevis (PB) is mentioned as a procedure concomitant to the modified Jones procedure. 1 However, FHL tendon transfer as a correction for clawed hallux has been cited in textbooks but not the journal literature. 7,8 Furthermore, outcomes of this procedure have not been presented in the literature to date. Since the cause of the deformity is multi-factorial, alternative treatments might be of value. Although the EHL tendon transfer is an effective procedure, it does take away the EHL as a motor unit to the hallux weakening extension. A previous study of 81 feet after a modified Jones tendon transfer found that in 48 feet catching of the great toe when walking barefoot was a problem, and 21 feet had transfer lesions; other complications included metatarsalgia, hallux flexus, hallux limitus, and asymptomatic nonunion of the IP joint. 1 The purpose of this study was to assess and analyze the outcomes of FHL tendon transfer for correction of clawed hallux deformity.
MATERIALS AND METHODS
All patients treated with FHL tendon transfer by two surgeons at a tertiary referral system were reviewed. Inclusion criterion was FHL tendon transfer to the proximal phalanx for correction of clawed hallux. Thirty-two patients qualified for the study, 12 were unreachable and one chose not to participate in the study; 19 patients participated. Subjects were contacted by telephone and gave oral and written consent for participation in the study, as approved by the appropriate Human Subjects Research Committee. Some participants chose to complete the survey by mail.
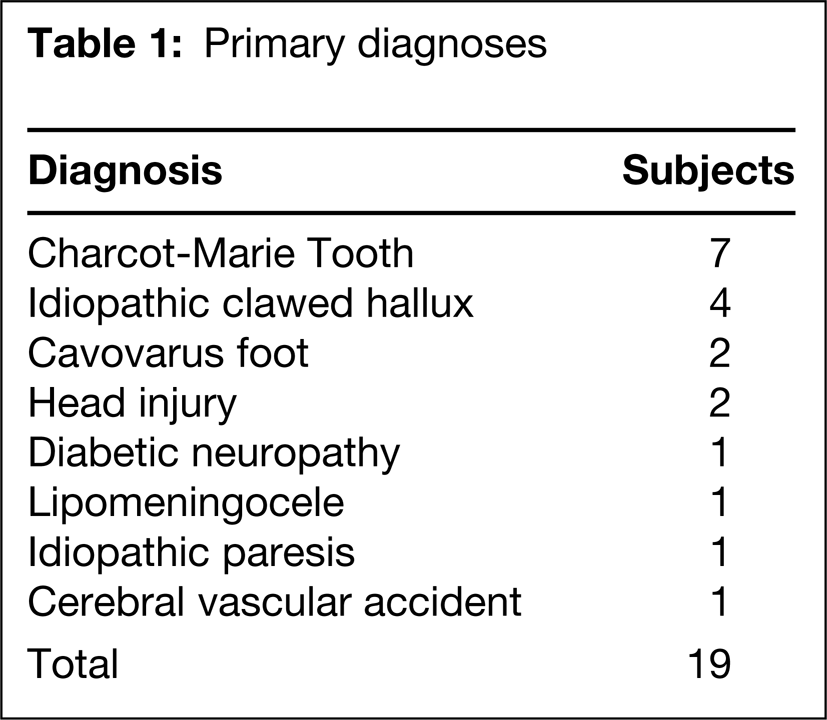
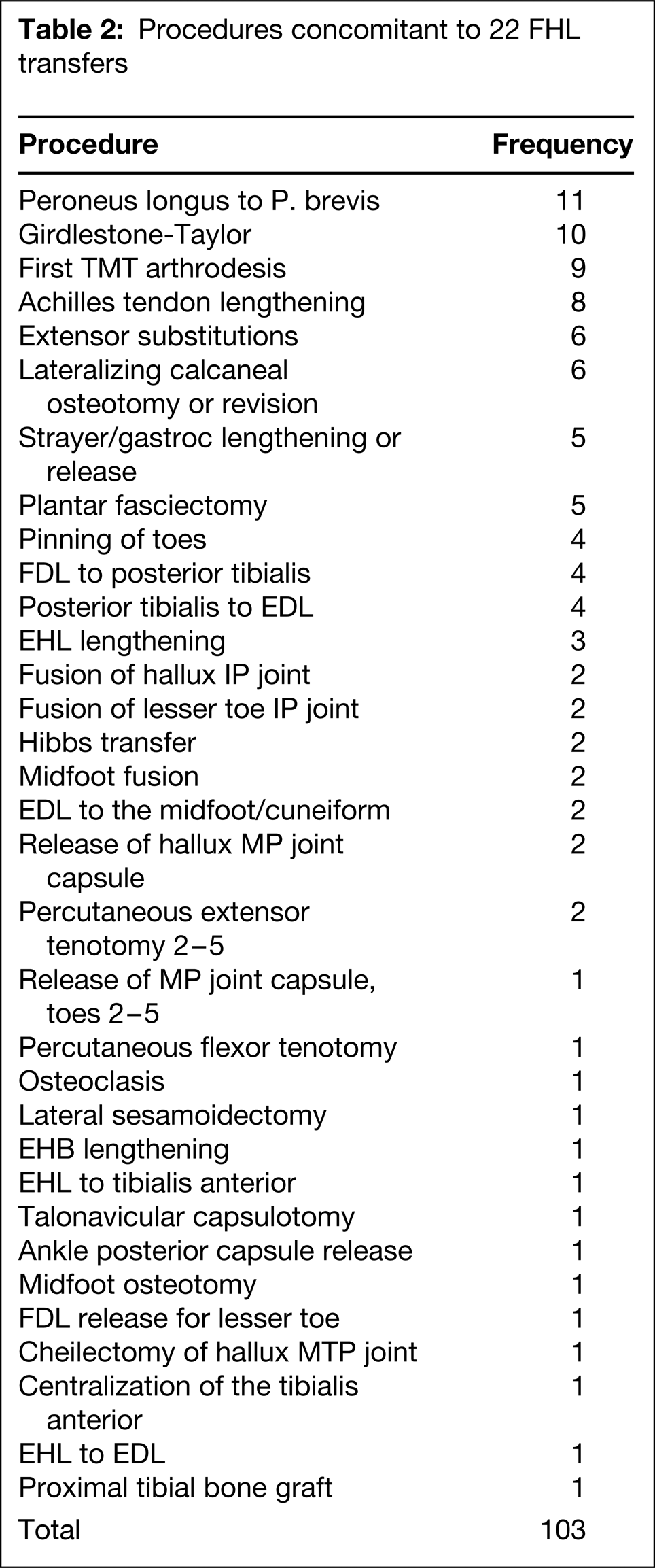
There were 19 subjects (22 FHL tendon transfers); 11 were men and eight were women. The average age at operation was 46.9 (range 16 to 80; ±3.8 standard error [SE]) years. The left foot was corrected in eight, the right foot in eight, and both feet in three subjects. Associated diagnoses with the clawed hallux are shown in Table 1, with the most common being Charcot-Marie Tooth disease in seven. Subjects had between one and 11 procedures (an average of 4.7 procedures) performed concomitant with the FHL tendon transfer, which are listed in Table 2. In two subjects the IP joint was fused.
Primary diagnoses
Procedures concomitant to 22 FHL transfers
Followup averaged 50.1 months (range 6 to 74 months; ±13.8 SE) after the procedure. Functional outcome was assessed using the Long-Form Musculoskeletal Function Assessment (MFA) validated survey. 3,9 The MFA score is determined by a questionnaire consisting of 100 self-reported health items, whereby a score of zero indicates the best possible outcome on a scale from zero to 100. The control population of middle-aged individuals has a mean score of 9.3, while a group of subjects with trauma or soft-tissue injury of the lower extremity reported a mean score of 28.4. 9 Additionally, the MFA describes patient functioning in terms of a “bother index” in each of the following 10 categories: mobility, hands, housework, self-care, sleep or rest, recreation, relationships, thinking or concentration, life changes and feelings, and work activities. The bother index ranges from one (“not at all bothered”) to five (“extremely bothered”). All subjects completed the survey; 12 over the phone and seven returned their responses through the mail. Subjects also were asked whether or not they were pleased with the overall result and whether they were limited in the types of shoes they could wear because of their hallux.
Radiographic outcome was determined for 13 subjects (15 feet) from preoperative and postoperative weightbearing lateral and anteroposterior (AP) radiographs by an independent physician who did not perform the surgery. Four feet had to be excluded from radiographic analysis because they were missing postoperative radiographs, and one patient's radiographs had been destroyed at the time of followup; additionally, the two subjects who had their IP joints fused were excluded. All measurements were taken using a goniometer. We measured the hallux valgus and IP angles on the AP radiographs. Axes were drawn through the first metatarsal and proximal and distal phalanges by first identifying the metaphyseal-diaphyseal junctions and then drawing a line through the midway points. On the lateral view we measured the angle of the IP joint and the MP joint. Axes through the first metatarsal, and proximal and distal phalanges were created by connecting two points made midway through the joint articular surfaces.
The talometatarsal angle was measured from lateral radiographs for 15 feet.
A repeated measures ANOVA was used to compare preoperative and postoperative radiographic data, with a p value of less than 0.05 considered significant.
OPERATIVE PROCEDURE
After anesthesia was administered, a medial incision was made from the hallux MTP joint to the IP joint. The plantar hallucal nerve was identified and retracted plantarly, and the IP capsule was released when necessary to correct deformity. The FHL tendon was identified, then the sheath was opened and divided distally to the distal phalanx. The tendon was clamped and divided from its insertion into the distal phalanx; it was then split into one-third and two-thirds, with the one-third section sutured to create a loop and the two-thirds lateral section kept intact and threaded with 2–0 resorbable suture. 7
A midline 3.5-mm drill hole was made through the proximal phalanx from plantar to dorsal approximately 1.0 cm distal to the joint; a curette was used to slightly widen the hole when necessary. Next, the two-thirds portion of the FHL tendon was passed through the proximal phalanx using a Keith needle until the toe was in a neutral position with the foot in neutral at the ankle. The suture weave on the two-thirds portion was sutured into the one-third loop of the FHL on the medial side of the toe. Both loops of the tendon were then secured into the surrounding soft tissue.
After the operation, the foot was generally immobilized in a neutral position in a splint for 2 weeks, then weightbearing was allowed as tolerated for 4 weeks in a walking boot. Subjects with additional procedures required nonweightbearing for up to 6 weeks.
RESULTS
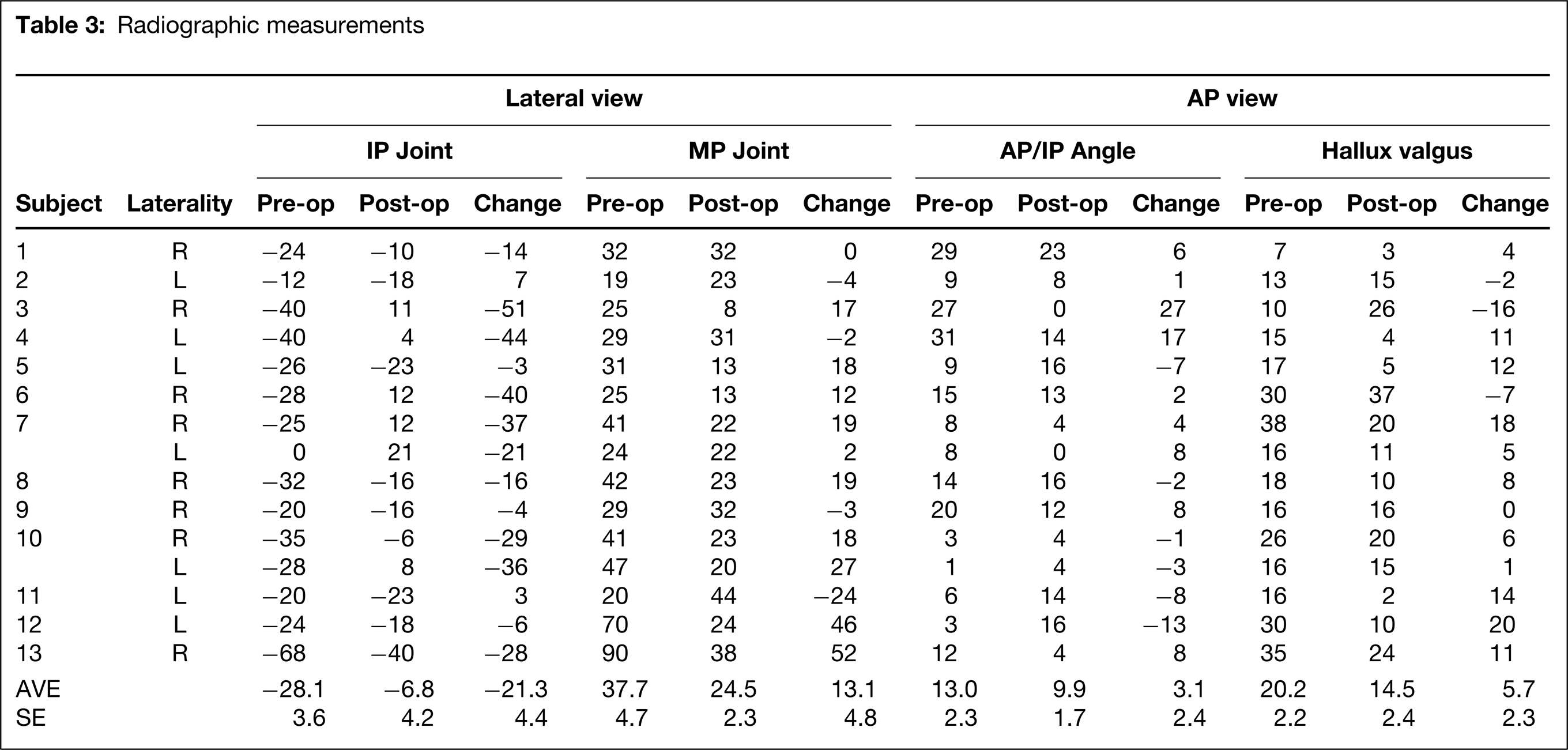
The radiographic results for each patient are shown in Table 3. The hallux IP joint angle from the lateral radiographs was significantly reduced postoperatively (p < 0.0012; n = 15), with an average reduction of 21.3 (± 4.4 SE) degrees; as seen in Figure 1, the average preoperative value was 28.1 (±3.9 SE) degrees of plantarflexion and postoperatively was 6.8 (±4.5) degrees. The hallux MTP joint angle also was significantly reduced (p < 0.0265, n = 15), with an average reduction of 13.1 (±4.8 SE) degrees. Preoperative (mean 37.7 ± 5.0 degrees SE) and postoperative (mean 24.5 ± 2.5 degrees SE) lateral MTP joint angle averages are shown in Figure 2.
Radiographic measurements
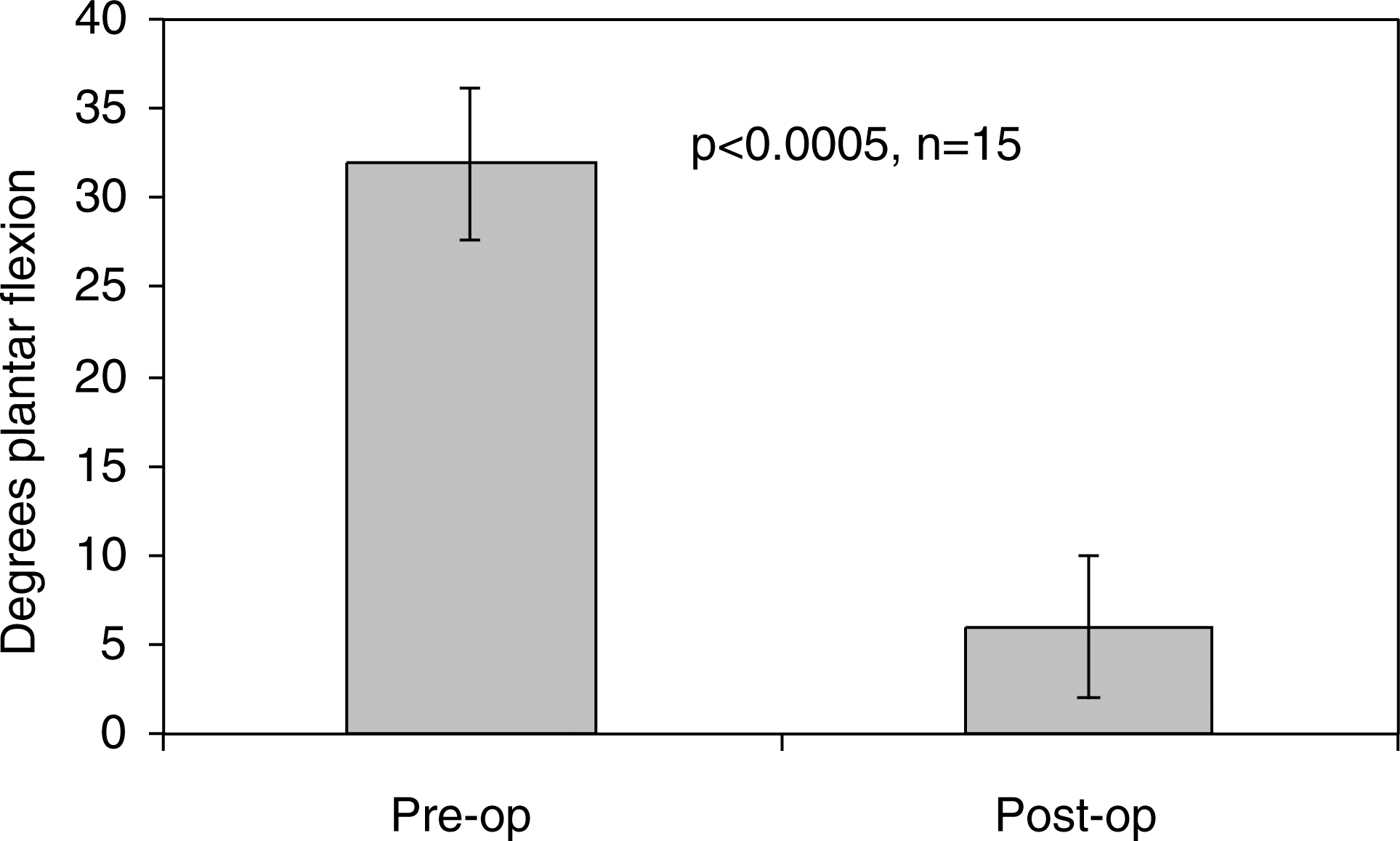
IP joint angles before and after surgery measured on lateral radiographs (degrees plantarflexion ± SE).
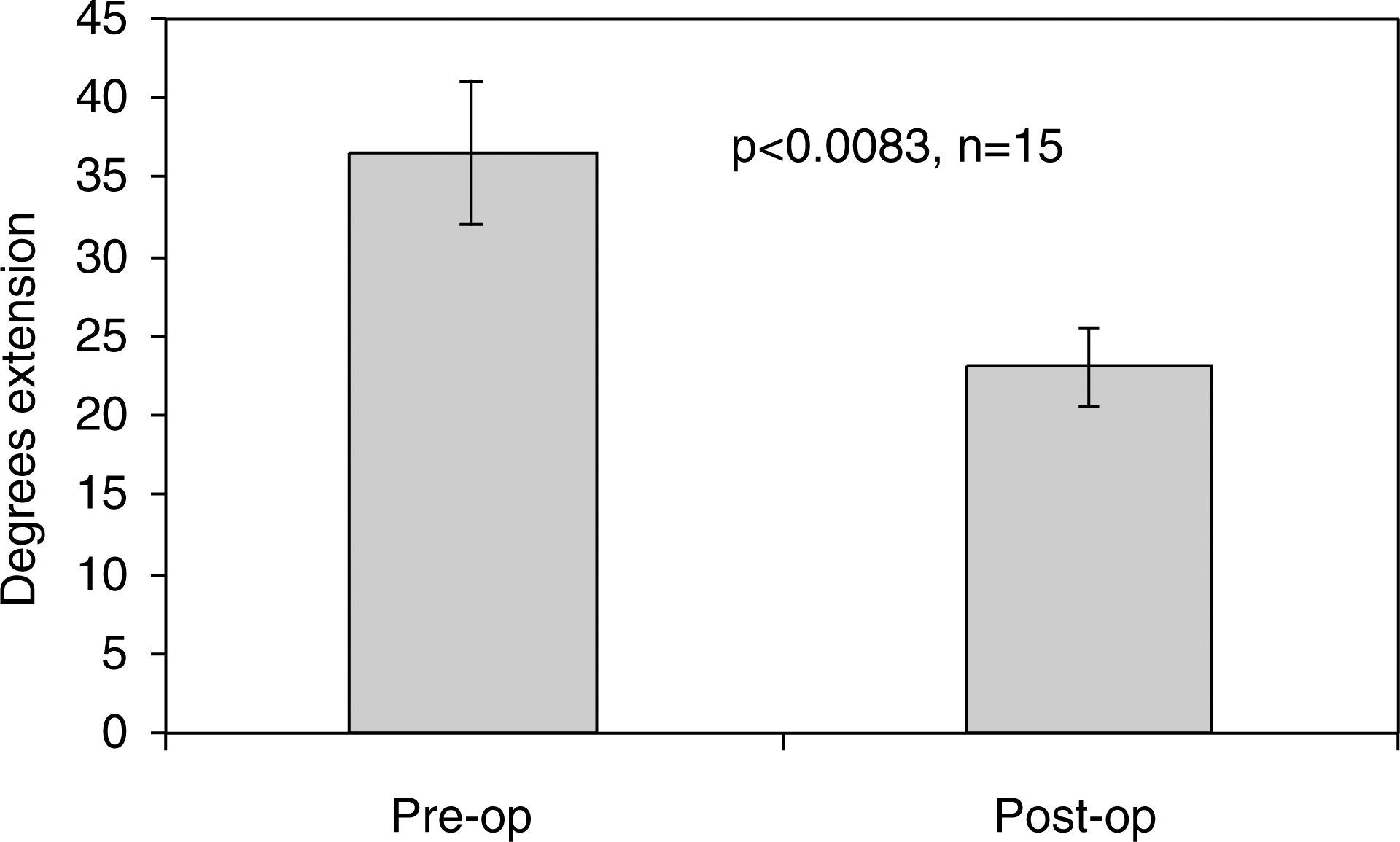
MTP joint angles before and after surgery measured on lateral radiographs (degrees extension ± SE).
On the AP radiographs, the hallux valgus angle was significantly reduced (p < 0.0334; n = 17). The average hallux valgus angle went from 18.9 (±2.3 SE) degrees to 13.8 (±2.3 SE) degrees after the surgery, with an average reduction of 5.1 (±2.2 SE) degrees. The IP angle measured on the AP radiographs had an average preoperative angle of 13.6 (±2.2 SE) degrees and postoperative angle of 10.3 (±1.7) degrees, with an average reduction of 3.3 (±2.4 SE) degrees, which did not signify a significant difference with the numbers available (p < 0.1797; n = 17).
The lateral talometatarsal angle did not show significant difference with the numbers available after surgery (p < 0.8780, n = 15).
Patients had an average MFA score of 14.6 (range one to 35; ±3.8 SE) on a scale from zero to 100, with a score of zero representing optimal function and the best possible outcome. Average bother index scores for each category ranged from 1.1 to 2.6 (whereby one equals “not at all bothered” and three equals “somewhat bothered”), with the most bothersome categories being mobility and hand activities, and the least bothersome being relationships, thinking and concentration, and job activities. Six of the subjects were working at the time of the survey.
Thirteen patients were satisfied and six were somewhat satisfied with the overall result of the surgery. Four patients reported that their hallux limited the types of shoes that they could wear, while 15 said that their toe did not. The most common complication was stiffness of the hallux MTP joint in four patients. No infections, fractures or other complications were identified in these 19 patients.
DISCUSSION
While FHL tendon transfer has been used for several years as an alternative to the modified Jones procedure for correction of clawed hallux, this procedure has not been presented in the peer-reviewed literature to date. Furthermore, there have been no reported studies presenting outcomes of FHL tendon transfer for correction of clawed hallux.
Correction of clawed hallux is most easily assessed by the IP and MTP joint angles from a lateral perspective. Clawed hallux is clinically observed as first MTP joint extension combined with IP joint flexion. Our data show significant reduction in the IP and MTP joint angles.
Our results suggest that the FHL tendon transfer yields high patient satisfaction, comparable to the modified Jones procedure. Thirteen patients (68%) were completely satisfied and six (32%) were somewhat satisfied with the overall result of surgery; none of our subjects were dissatisfied. In contrast, studies on the modified Jones procedure have reported dissatisfaction rates from 9% to 21%.1,2,4,5,10,12 This positive result was also reflected in the subjects' low MFA and bother index scores.
One difficulty with administering the MFA for this study was that the patients had a hard time distinguishing the role of the hallux in their daily activities. Many of these patients had progressive and degenerative diseases that had been affecting their function before and since their surgery for correction of clawed hallux. All patients had concomitant procedures done at the time of the FHL tendon transfer, which further complicated analyzing the results. Additionally, several of the questions assessed functionality unrelated to the surgery and the lower extremities; for example, some of the subjects' MFA scores increased due to problems with their hands. Our analysis of the MFA results would be stronger if we had preoperative MFA scores for comparison.
Our study also would have been strengthened with clinical followup evaluation, which was not practical because many of our subjects lived out of state. Further outcome studies using clinical evaluation would be beneficial.
It has been shown that clawed hallux can result from excessive motor function in one of three muscles: FHL, peroneus longus (PL), and EHL. 11 While the traditional correction for clawed hallux is the modified Jones procedure with an EHL tendon transfer and IP joint arthrodesis, this study suggests that transfer of the FHL tendon is an effective alternative operative procedure. The results of this study indicate reduction of the clawed hallux deformity and high patient satisfaction after an FHL tendon transfer. Furthermore, this alternative procedure has the additional benefits of not weakening extension or removing the EHL muscle-tendon unit as a motor to the hallux, and not requiring fusion of the IP joint.