
Abstract

INTRODUCTION
Osteomyelitis is notoriously difficult to treat, with poor antibiotic penetration, persistence of microorganisms, and a tendency towards acute exacerbation and recurrent flares. The prolonged use of parenteral antibiotics is associated with prolonged hospitalization and undesirable side effects. Buchholz and Gartmann 3 first described the successful use of gentamicin impregnated polymethylmethacrylate (PMMA) in the treatment of infected total hip arthroplasty. Klemm 10 used gentamicin-PMMA beads as a local treatment for chronic osteomyelitis. Treatment of osteomyelitis with gentamicin-PMMA beads allows primary wound closure and has the advantages of increased patient comfort with better compliance, avoidance of prolonged systemic antibiotics with their inherent side effects, and short hospitalization with reduced cost. 2,9 Intermediate term or permanent implantation sometimes is indicated. The problem of device-associated infection has not been thought to be relevant to antibiotic beads. Gentamicin-PMMA beads retrieved from two patients with foot osteomyelitis showed evidence of bacterial adherence with development of gentamicin resistance.
CASE REPORTS
Two patients with acute osteomyelitis of the foot were treated with operative debridement and short-term implantation of mini gentamicin-PMMA beads. Patient A had rheumatoid arthritis and developed first metatarsal osteomyelitis. Patient B had a recent fifth metatarsal head ulceration leading to osteomyelitis (Figure 1). The initial bone fragment cultures yielded gentamicin sensitive Staphylococcus epidermidis (minimal inhibitory concentration, [MIC] of 0.03 mg/L and 2 mg/L). Both patients responded well to local antibiotic treatments, and the gentamicin-PMMA beads were retrieved after 2 weeks of implantation as recommended. Scanning electron microscopy (SEM) of the retrieved beads revealed multiple bacterial clusters within the crevices of the beads (Figure 2). The beads were ultrasonicated to dislodge the bacteria for culturing. Both specimens yielded viable Staphylococcus epidermidis, which now had a gentamicin MIC over 128 mg/L, much higher than the original Staphylococcus epidermidis isolated from the bone fragment culture. The markedly elevated MIC indicated a possible emergence of a highly gentamicin-resistant Staphylococcus epidermidis strain.
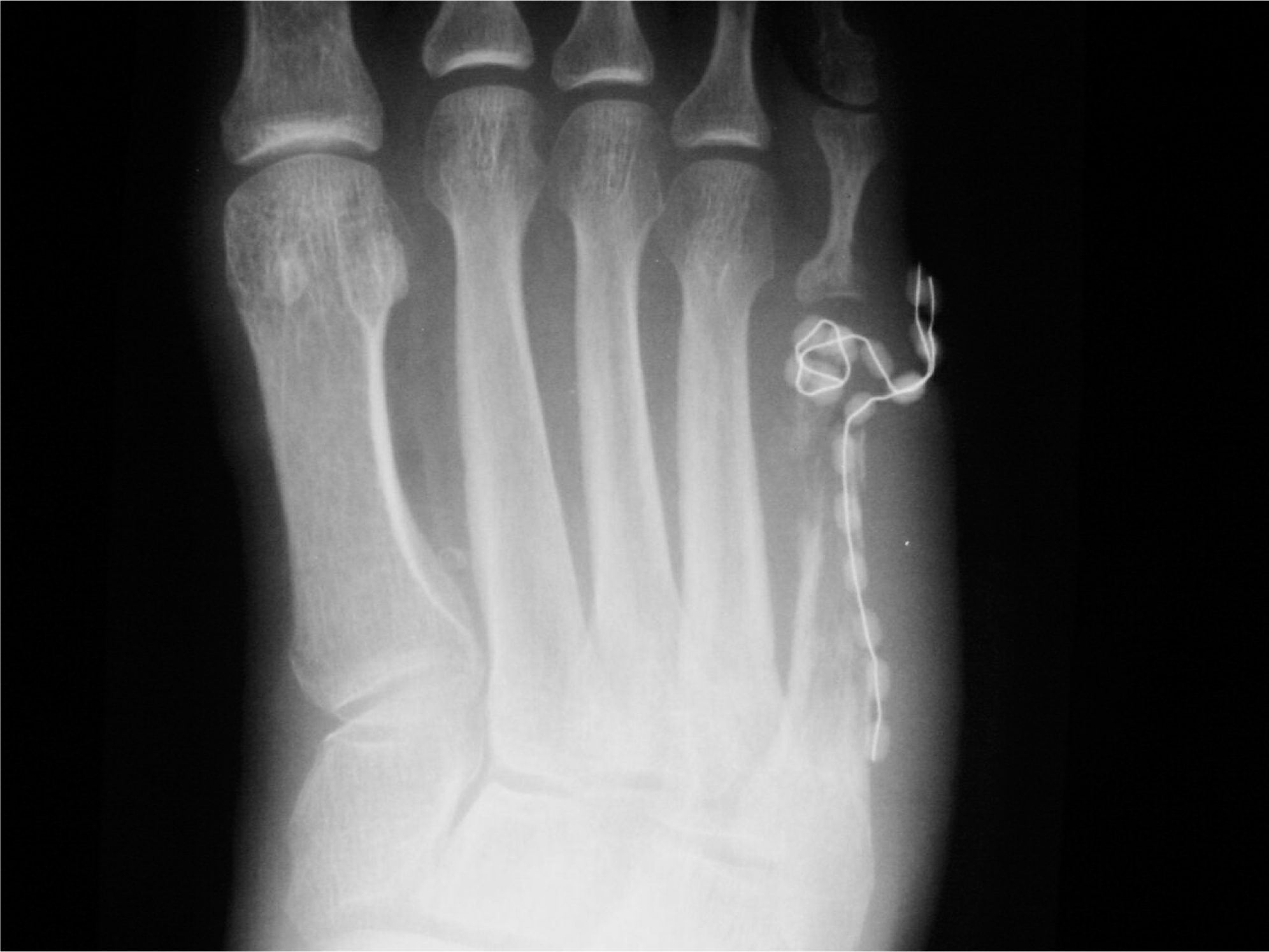
Radiograph showing osteomyelitis of fifth metatarsal with two chains of mini-gentamicin beads implanted.

DISCUSSION
Gentamicin-PMMA beads are especially useful in the treatment of osteomyelitis, because the bioavailability of systemic antibiotics to the infected bone is low due to poor perfusion. Good clinical results have been shown. 2,9 The PMMA acts as a carrier for the slow local release of gentamicin antibiotic. After the implantation of gentamicin-PMMA beads, a peak local gentamicin concentration 200 times higher than after parental injection of 80 mg gentamicin was measured, and six to eight fold higher antibiotic concentrations were detected in cortical bone and in cancellous bone. 18 In vitro elution studies showed prolonged release of gentamicin, which is bactericidal to common pathogenic organisms even on the 80th day. 18 The serum and urine concentration remained low, thus minimizing the risk of ototoxicity and nephrotoxicity. 4 Gentamicin has a broad spectrum of bactericidal activity. Staphylococcus species are defined as sensitive to systemic gentamicin therapy if the MIC is 4 mg/L or less and resistant if the MIC is 16 mg/L or above, as determined in agar dilution, according to the National Committee of Clinical Laboratory Standards. 11 The local antibiotic concentration achieved by gentamicin beads is a hundred times higher than the MIC and 20 times higher than the minimal bactericidal concentration (MBC) of common microorganisms found in osteomyelitis. 6,11 Even those microorganisms categorized as ‘resistant’ to systemic therapy are eradicated. Such high concentrations cannot be achieved by parenteral administration of gentamicin.
In most patients with osteomyelitis, the implanted beads are removed at 10 to 14 days by pulling on the last bead which is left protruding from the skin. Infection arrest rates of 85% to 90% have been reported. 2,9 In cases of recurrence after gentamicin beads use, redebridement and placement of new beads can be considered. 9 Intermediate term or permanent implantation sometimes is indicated in selected patients with localized osteomyelitis, large dead spaces that need to be filled, poor soft-tissue coverage, and high surgical risks. 5,9 Henry reported a higher remission rate with increased duration of gentamicin bead placement without an increased risk of complications. 5 Acquired gentamicin resistance over the years has not been observed. 5,6 Antibiotic impregnated devices are used to decrease device-associated infections. 7 Since antibiotic is continuously eluded from the gentamicin beads, it is not believed to promote infection, as seen in other implant materials. This complacency is disputed by the demonstration of bacterial clumps by SEM on gentamicin beads recovered after 2 weeks. The increases in MIC and minimal bacterial concentration (MBC) of the recovered Staphylococcus epidermidis further exemplified the problem.
Staphylococcus epidermidis is an adherent organism. The rapid adherence of bacteria to a foreign body surface followed by cell proliferation and intercellular adhesion results in formation of a biofilm, which consists of multilayered cell clusters embedded in amorphous extracellular substances (slime). The biofilm protects the embedded microorganism against host defense mechanisms and against antibiotics. 12,14,17 Often it is difficult to eliminate the staphylococci from the infected polymer surface. Previous in vitro studies have shown that PMMA (without antibiotics) provided a surface for bacterial growth. Increased resistance of bacteria after adherence was thought to be related to slime protection. 1,12 A study done with tobramycin and vancomycin impregnated PMMA showed that the organism remained sensitive to the antibiotics eluded. 8 Four cases of small colony variants of Staphylococcus aureus after gentamicin bead placement for osteomyelitis were reported by von Eiff C et al. in 1997. 16 All four patients had recurrences of osteomyelitis. He, therefore, alerted physicians to look for small colony variants in case of treatment failure. We demonstrated emergence of gentamicin-resistant Staphylococcus epidermidis from originally sensitive strains after gentamicin bead placement for 2 weeks in two patients with osteomyelitis. The porous surface of PMMA with crevices is ideal for adherence and colonization. Our findings suggested that bacterial adherence to the gentamicin-PMMA beads and prolonged exposure to gentamicin resulted in the emergence of highly resistant strains. Resistance may occur by selective growth of resistant strains or by induction of mutation from sensitive strains into highly gentamicin resistant strains. The second mechanism is more likely, because with selective growth the first culture should also yield the resistance strain.
Modification of the polymers to obtain anti-adhesive or anti-infective surfaces may help to solve the problem of bacterial adherence and biofilm formation. Incorporation of antibiotics or other antimicrobial agents into the polymers to produce anti-proliferative, colonization-resistant devices have been used to prevent polymer-associated infections. 7 Unfortunately, as shown in our two patients, the release of gentamicin did not protect the gentamicin-PMMA beads from colonization. Whether incorporation of a second antimicrobial agent onto the gentamicin beads is a feasible and effective way to achieve bacterial elimination needs to be explored. The development of biodegradable materials as drug carriers may lead to biodegradable antibiotic beads, which would obviate the need for removal and would not act as a nidus of infection. 13,15
CONCLUSION
Emergence of highly resistant Staphylococcus epidermidis after gentamicin-PMMA beads implantation for osteomyelitis indicate possible adherence and survival of gentamicin sensitive strains despite the high local antibiotic concentration and induction of mutation into highly resistant strains. The resistant Staphylococcus epidermidis protected within the beads may be a cause for treatment failure or late recurrence. Culture results should be interpreted with care. Debridement and implantation of a new chain of gentamicin-PMMA beads in case of recurrence may not be able to eradicate the highly resistant organism and alternative therapy should be considered. All gentamicin beads which have served their purposes should be removed and long-term implantation avoided.