
Abstract
Background: Long-term followup (over 5 years) of staged reconstruction for chronic ruptures of both peroneal tendons using a Hunter rod and the flexor hallucis longus (FHL) tendon is presented. Methods: Seven patients with chronic ruptures of both peroneal tendons who had at least two previous surgeries that failed were treated with excision of the remaining portion of the peroneal tendons and implantation of a Hunter rod to the insertion of the peroneus brevis. Patients performed passive range of motion exercises for 3 months before removal of the Hunter rod and transfer of the FHL into the newly formed sheath, attaching it to the insertion of the peroneus brevis on the fifth metatarsal. The patients' ages ranged from 30 to 57 (average 38) years. All were women. All had at least two previous failed procedures (range two to six). The average time from initial injury to the index surgery was 4.6 (range 2 to 7) years. Patients were evaluated by physical examination and a questionnaire. The average range of followup was 8.5 years (range 143 to 167 months). Results: All wounds healed without complications. One patient (a workers' compensation patient) had continued complaints of pain and ambulated with a molded ankle-foot orthosis (MAFO). The remaining six patients reported complete relief of symptoms and returned to full preinjury levels of activity. One patient required a Broström ankle ligament repair 2 years after tendon transfer for a new injury but has remained pain free for the last 62 months. There were five excellent, one good, and one fair result. All patients stated they would repeat the surgery. Conclusion: Staged reconstruction with excision of the remaining portion of the peroneal tendons and reconstruction with a Hunter rod and FHL transfer has been shown to be an effective long-term treatment for chronic peroneal tendon ruptures.
INTRODUCTION
Pathology of the peroneal tendons has been cited as a cause of chronic lateral ankle pain. 1–6,12–14,25,35,36 Fissuring and longitudinal splitting of the peroneus brevis and longus tendons have been reported as an etiology of chronic ankle pain and functional instability. When recognized early, direct repair usually is possible with good results. 1,3–5,8,13,14,17,25,36 However, when these lesions become chronic or involve both tendons, the results of surgery are less favorable. We evaluated the results of a staged reconstruction in seven patients who had ruptures of both peroneal tendons and in whom a minimum of two previous attempts at surgical repair failed.
Evaluation by MRI demonstrated chronic thickening, fissuring, and stenosis of the remaining peroneal structures. This presented two problems for salvage: the loss of an adequate tendon sheath and the lack of adequate remaining tendon tissue. Borrowing from techniques in the hand literature, these tendons were reconstructed using a staged procedure of excising the remaining tendon, placing a Hunter rod to form a new tendon sheath, 10,41 and transfer of the FHL into the newly formed sheath 3 months later.
METHODS AND MATERIALS
Between 1988 and 1997, seven patients were evaluated for chronic tendon pathology involving both the peroneus longus and brevis tendons. All patients had undergone at least two prior surgical procedures on their peroneal tendons (range two to six previous procedures). The average time from initial injury to this procedure was 4.6 (range 2 to 7) years. Patients ranged in age from 30 to 57 years, with an average age of 38 years. All were women (Table 1).
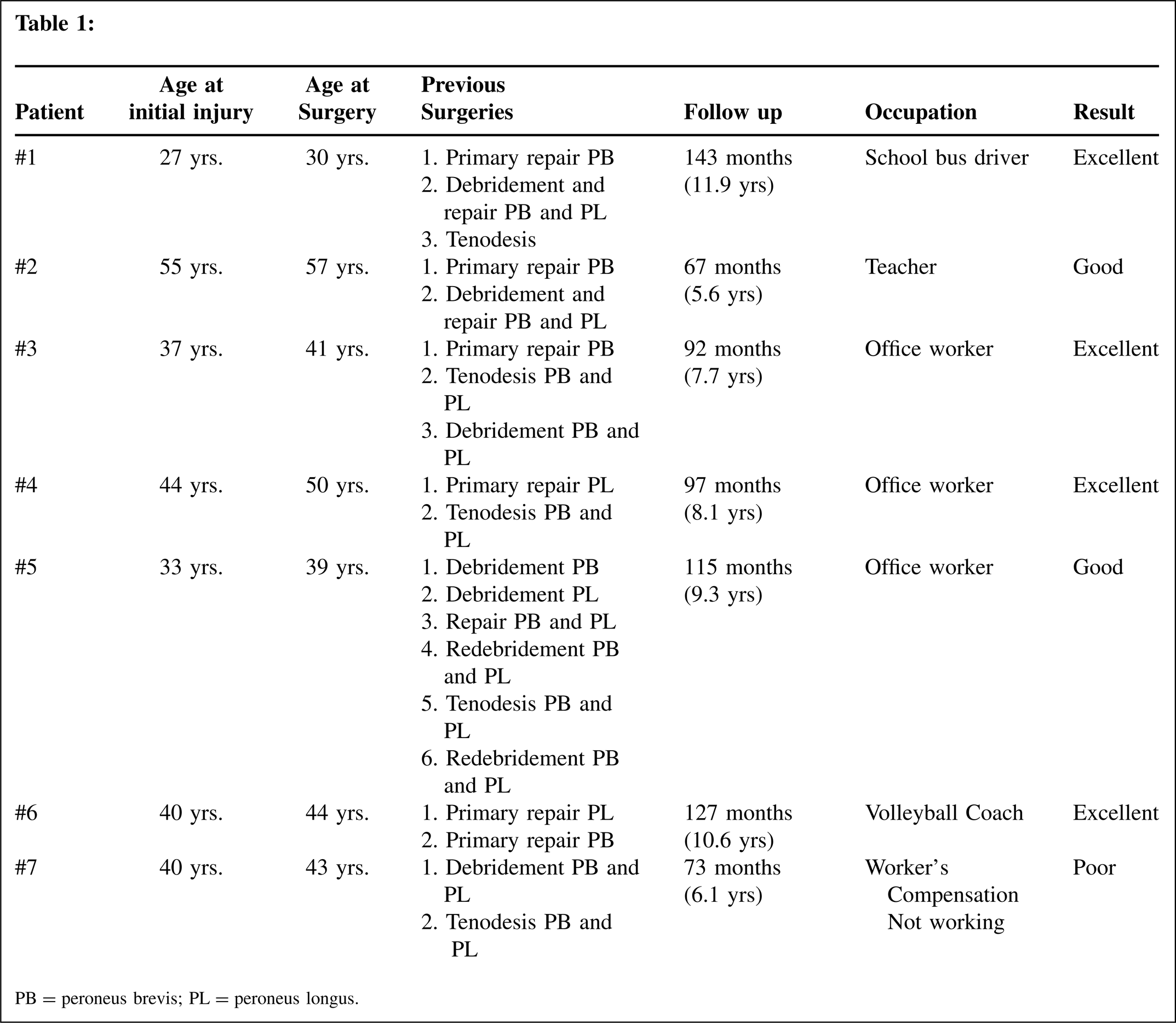
PB = peroneus brevis; PL = peroneus longus.
All patients complained of chronic lateral ankle pain, swelling, and functional instability. All patients required the use of an ankle support and had decreased, painful inversion and eversion when compared to the contralateral leg. Radiographs revealed no arthritic changes in the ankle or hindfoot. MRI revealed significant thickening, scarring, and stenosis of the peroneal tendons (Figure 1). In most patients, it was not possible to clearly define the morphology of the individual tendons as a result of the previous surgical procedures and progressive tendinosis.

Operative Technique
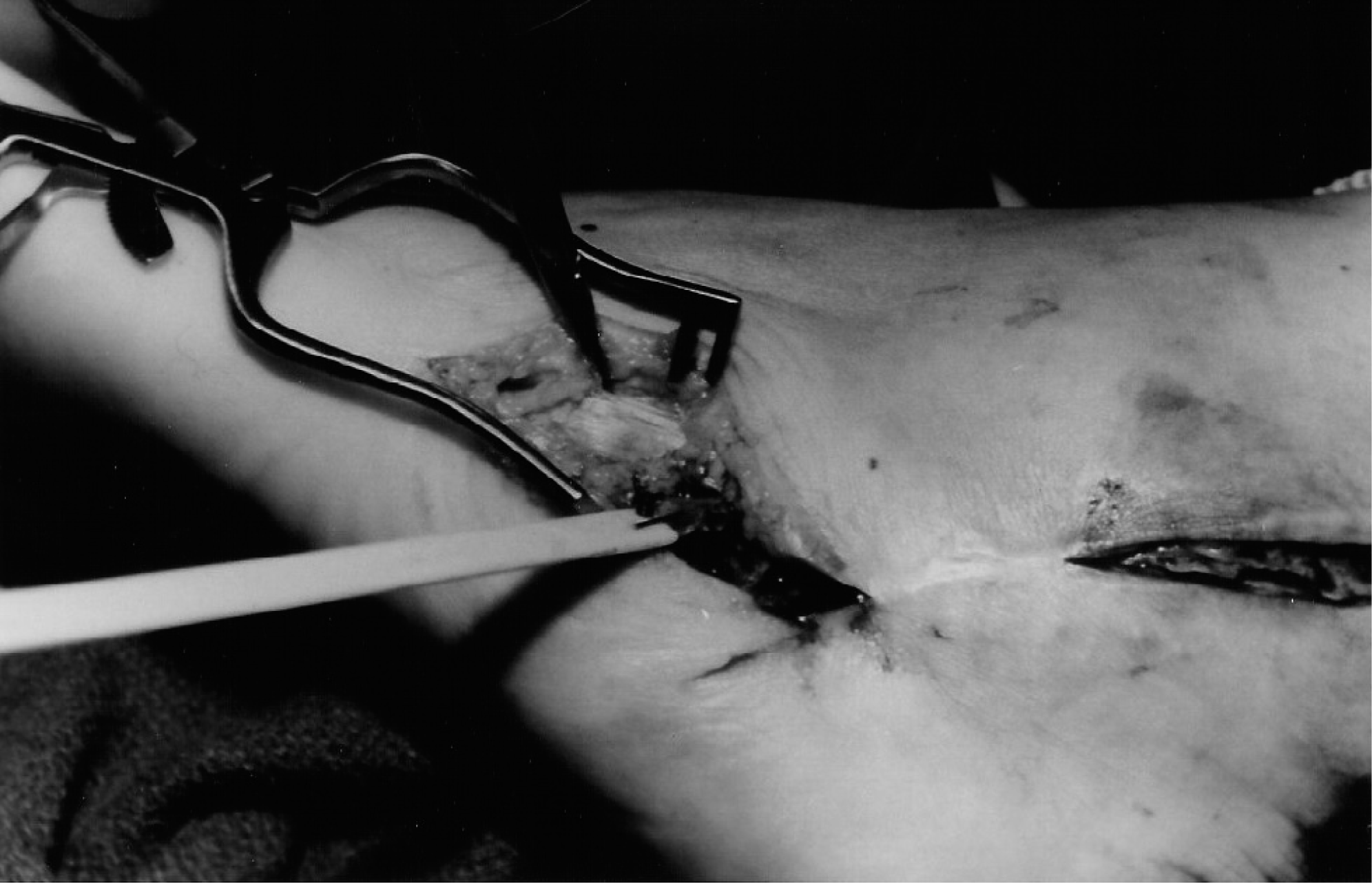
The first stage of reconstruction consisted of debridement of the remaining peroneal tendon tissue and tendon sheath and implantation of a 6-mm Hunter rod into the bed of the peroneal sheath (Figure 2). The Hunter rod was sutured to the remaining stump of the peroneus brevis tendon distally and the proximal end was allowed to remain free in the sheath (Figure 3). The sheath was then trimmed of any redundancy and closed over the Hunter rod. Postoperatively, the patients were allowed bear weight as tolerated in a removable short-leg walking boot. They were instructed to remove the boot four times a day and perform active and passive range of motion exercises of the ankle and hindfoot in all planes of motion.

Appearance of the peroneal tendons at the time of debridement in preparation for insertion of the Hunter rod.

At 3 months, a transfer of the FHL tendon was done. Harvesting of the FHL was done as previously described (Figure 4). 37,38 Once the FHL was harvested, a small incision was made at the proximal aspect of the previously made lateral incision overlying the proximal aspect of the Hunter rod, staying proximal to the lateral malleolus. The FHL was transferred from medial to lateral into this incision (Figure 5). The proximal portion of the Hunter rod was identified, and the FHL was attached to the rod (Figure 6). A small distal incision was made over the distal suture site of the Hunter rod and the remaining portion of the peroneus brevis tendon. The Hunter rod was released from this suture site and then pulled distally, allowing the FHL tendon to slide into the newly formed tendon sheath (Figure 7). The FHL was then attached to the remaining stump of the peroneus brevis tendon using a Pulvertaft weave.
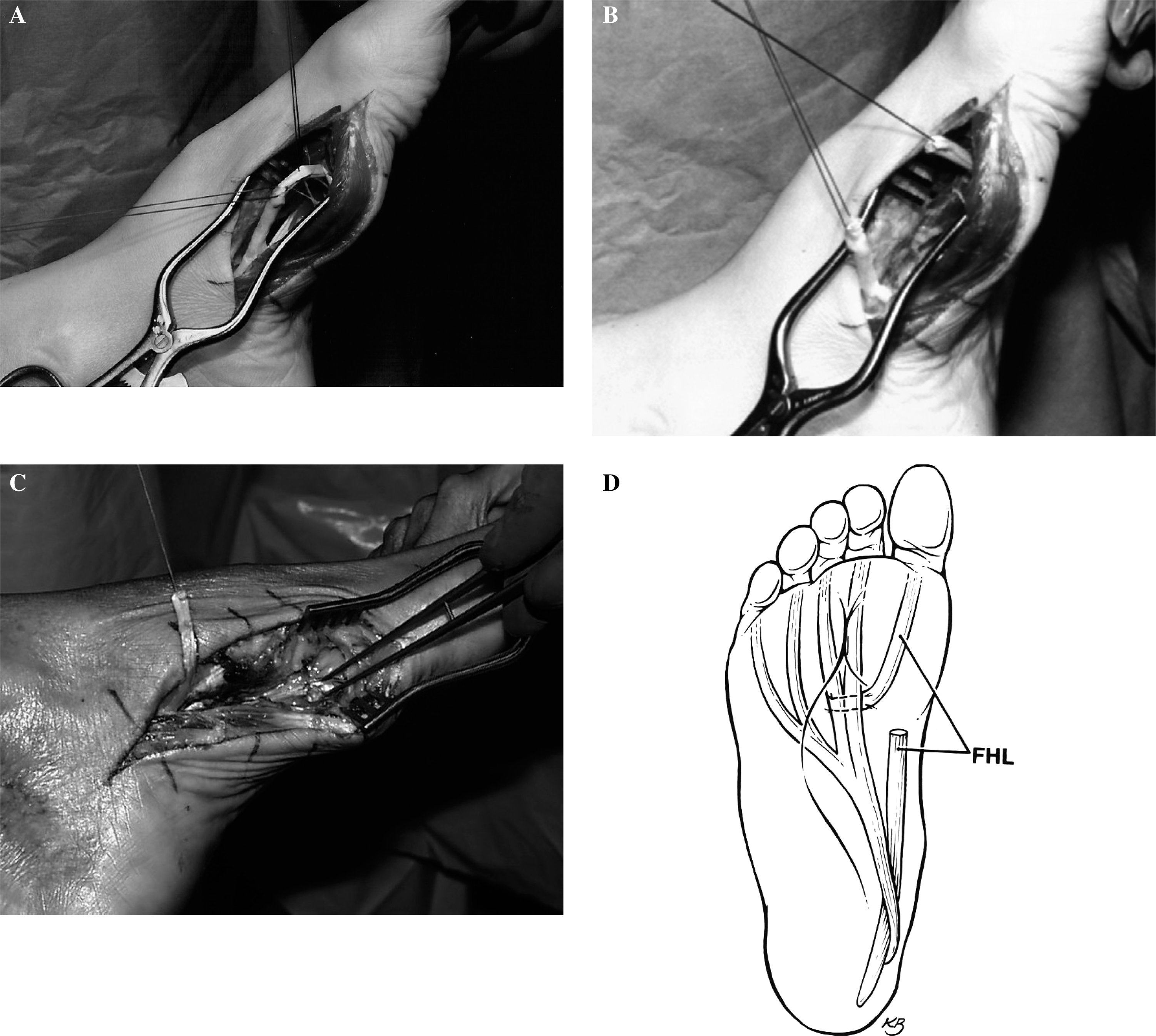

The FHL tendon has been transferred to the proximal lateral incision. Note the length of available tendon for transfer. Care is taken not to open the newly created sheath of the peroneal tendons.

The proximal pole of the Hunter rod is identified. The FHL will be attached to the proximal end of the Hunter rod and then pulled through the new sheath.
The Hunter rod has been pulled through the new sheath and the FHL sutured to the distal stump of the peroneus brevis tendon.
Postoperatively, the patients were allowed partial weight-bearing for 3 weeks and then advanced to full weightbearing in a removable walking cast. They were instructed to begin active and passive range of motion exercises of the ankle and hindfoot in all planes of motion. Home strengthening exercises were begun at 6 weeks, and the patients were advanced to an ankle stirrup at 8 to 10 weeks based on their strength. All patients had formal physical therapy for functional rehabilitation of the ankle starting at 8 weeks.
RESULTS
There were no wound complications. At average followup of 8.5 (range 5.5 to 11.9) years, six patients reported complete resolution of pain. The patient with pain was the one workers' compensation patient in the group. This patient was the only patient requiring the use of an ankle support (molded polypropylene ankle foot orthosis), all other patients walked without assistive devices. The same six patients had symmetric, painless range of motion bilaterally at the ankle, subtalar, and transverse tarsal joints. Four had symmetric 5/5 motor strength of the peroneals on manual muscle testing. Two had 4+/5 motor strength, and the one workers' compensation patient had 3/5 strength. All patients except the one workers' compensation patient could perform single-heel rise and walk on their tiptoes without instability or pain. One patient required a Broström ankle ligament repair 2 years after surgery after a new injury. She remained free of pain at 62 months after surgery.
All patients except the workers' compensation patient returned to full-time employment, one as a school bus driver, one as a college volleyball coach, one as a high school teacher, and three as office workers. These six patients were satisfied with their results and stated that they would have the surgery again and would recommend the surgery to a friend. Based on this evaluation, the authors rated the results as five excellent, one good, and one poor result.
DISCUSSION
Chronic lateral ankle pain can have many different etiologies. Peroneal tendon pathology has been identified as a major cause. 2,3,15,20,21,24,25,26,28–30,32–34,39 The etiology of longitudinal fissures of the peroneal tendons has not been clearly identified, and several theories have been postulated. 15,19.,25 Histologic evaluation of these splits has shown chronic wear with cystic and myxoid degeneration of the tendon. Frey and Shereff 9 proposed a zone of critical hypovascularity as a source of tendon splitting. 9 However, Sobel, et al. 31,32 have shown no correlation between the sites of tendon splitting and hypovascularity. They believe that there is a mechanical impingement from the fibular groove. 31,32 Other authors suggested incompetence of the peroneal retinaculum, the presence of a sharp posterior fibular ridge, or dynamic compression between the peroneus longus and brevis tendons. 6,7,23,30,32–34,36
When recognized early, many authors have reported good results by direct repair of the tendons. 1,3–5,8,13,14,17,25,36 The difficulty arises when these repairs do not work. Our patients had at least two previous surgical procedures and all attempts at primary repair and anastamosis of the peroneus brevis and longus tendons failed. They presented with advanced pathology of both tendons. This represents a small subset of patients with peroneal tendon pathology seen in our practice, and there are no current studies in the literature on the incidence. These patients were young (average age 38), and our goal was to find a means of achieving dynamic stabilization of the ankle with restoration of peroneal tendon function. All patients in this series had been told they would need either full-time bracing or surgical fusion of their hindfoot. We thought that for reconstruction it would be important to create a viable tendon sheath that allowed free movement of the new tendon with re-establishment of the stability of the peroneal retinaculum and to find a suitable motor unit to provide a dynamic replacement for the peroneal tendons. Because of the history of multiple surgical procedures and the length of time between the initial injury and the presentation to our office, we thought the peroneal muscles would have atrophied, resulting in decreased excursion and would not be a reliable source of a viable motor unit.
The use of a Hunter rod would recreate a viable tendon sheath; the principle of implantation of a silicone rubber rod and subsequent reimplantation of a tendon transfer has been well-documented with studies demonstrating a mesothelial cell lined pseudosheath. The fluid formed resembles synovial fluid and lubricates the gliding motion of the newly transferred tendon. 10,11,16,40
Based on the success of the use of FHL transfer in the treatment of chronic Achilles tendon repair, we thought this would be a suitable motor unit. 37,38 The FHL has a strength percentage of 3.6 and could be a substitute for the peroneus brevis muscle-tendon unit which has a strength percentage of 2.6 as determined by Silver et al. 27 The length of the FHL tendon provides adequate tissue for transfer. The FHL is an in-phase muscle with an axis of contracture similar to the peroneal muscle-tendon unit as it arises off of the posterior fibula. 18 Previous work using the FHL for Achilles tendon reconstruction demonstrated minimal donor morbidity. 37,38
This technique uses the insertion of the FHL into the residual stump of the peroneus brevis tendon and obviously does not allow restoration of function of both peroneal tendons, only the peroneus brevis tendon. In our patients, the distal portion of the peroneus longus tendon was too enmeshed in scar to serve as a viable insertion point for the FHL tendon. We thought that further dissection into the plantar lateral aspect of the foot to retrieve the distal portion of the peroneus longus tendon would create greater morbidity than benefit. Therefore, the decision was made to rely on the distal stump of the peroneus brevis tendon as the insertion point of the FHL. At followup we did not find any measurable morbidity from the loss of active peroneus longus tendon function. None of the patients developed varus or cavus deformity to indicate there was overpull of the posterior or anterior muscle-tendon unit. The reason for this is unclear. We believe that the remaining distal portion of the peroneus longus tendon being scarred down produced a tenodesis effect that counteracted the pull of the invertor tendons.
The biggest weakness of this study was its retrospective review. This is an infrequent problem and the collection of data extended over 6 years with only seven patients. No standardized preoperative collection of objective and subjective data was done other than the information being gathered by the senior author (KLW) in his assessment of the patients clinically. Therefore, we did not think that we could accurately apply any specific measurement tool to our results that would be statistically valid. We chose to rely on patients physical examinations and subjective responses at the time of followup. We recognize that this does not provide statistically significant data, but with our small sample size statistically significant data would have been unlikely.
Nonetheless, with the available number of patients, we believe the clinical results and patient satisfaction level demonstrate that staged reconstruction of chronic degeneration of both peroneal tendons with a Hunter rod and FHL tendon transfer provides a satisfactory result for this difficult clinical problem. Six of our seven patients were pain free at average followup of 8.5 years and were working full time without complaints.