
Abstract
Background: Patients undergoing surgery on the foot and ankle who require immobilization are typically placed in splints or soft compression dressings after surgery to avoid complications associated with swelling. As swelling subsides, this temporary immobilization is removed and replaced with a short-leg cast, making an additional office visit necessary, which adds to the cost as well as patient discomfort. Methods: We apply a cast in the operating room using a special padding technique to accommodate postoperative swelling. It is supportive enough that it does not need to be replaced shortly after surgery. This cast was applied to 38 patients having surgery on the hindfoot or ankle between March, 2003, and February, 2004. Results: All patients tolerated the cast during the initial 2 weeks after surgery, and there were no complications. Conclusion: The purpose of this study was to describe the casting technique and document its safety for use immediately after surgery on the hindfoot and ankle.
INTRODUCTION
Selecting the best choice of postoperative immobilization after surgery on the foot and ankle is an important decision. Although cast immobilization usually is desired for stability, immediate postoperative casting can cause complications from increased compartmental pressure. 3 Excessive swelling within casts can lead to severe pain, pressure ulcers, and impaired wound healing and may contribute to development of compartment syndrome. 2 This may lead to high rates of early cast removal to avoid complications such as delayed wound healing, infection, and ultimately operative failure. Some studies have suggested that the only cast that is safe to use in the immediate postoperative period for ankle fractures is a cast that has been split and spread, because it is the only cast that accommodates swelling and tissue expansion. 4
To prevent serious complications, most foot and ankle surgeons initially apply splints or soft Jones-type dressings to accommodate postoperative swelling. 1 Most procedures performed on the foot and ankle are either done on an outpatient basis or the patients are discharged after just a few days in the hospital, prior to the time one would expect the normal postoperative swelling to have subsided. 1 Thus, removal of splints or soft-compression dressings requires an additional office visit to have the definitive cast placed. The need for early followup and cast change places an extra burden on surgeons and their staff and can be uncomfortable and inconvenient for the patient. All of this also adds extra costs to the perioperative period. We apply a cotton batting compression dressing covered with a fiberglass cast in the operating room immediately after hindfoot and ankle surgery that is safe to use after elective operations or acute trauma and eliminates the need for temporary splinting and early followup for cast placement. This technique is a modification of one that was developed and has been used by Jiun-Rong Peng, M.D. (Orange, California) for more than 20 years.
MATERIALS AND METHODS
Study Design
This study was approved by the Institutional Review Board at our medical center, and all patients provided informed consent. Patients who underwent surgery on the hindfoot or ankle, either electively or after a traumatic injury, between March, 2003, and February, 2004, were included in this study. All operations were performed by one of the two surgeons (AC and NFS) who participated in this study. Contraindications to this cast included lower extremity neuropathy, severe soft-tissue injury, or increased compartment pressures, although none of our patients were excluded because of these problems. All patients were fitted with the cotton-batting cast in the operating room immediately after surgery, and initial followup was at 2 weeks. The outcomes documented and study endpoints included severe pain; wound or tissue complication, such as infection, ulceration, delayed wound healing or excessive swelling; and the need to remove the cast early for any reason.
Technique of Application
Casts were applied while all patients were in the operating room immediately after completion of surgery, using the following procedure and materials (Table 1, Figure 1). First, a sterile dressing was placed over the incisions. A sterile tubular stockinette was then placed in the usual fashion. Next, two or three layers of Curity Lakeside Cotton (The Kendall Co., Mansfield, Massachusetts) were loosely applied over the stockinette to create a thick layer of padding from the metatarsophalangeal joints to a point just distal to the tibial tuberosity. It is very important that these layers of cotton batting be applied loosely to accommodate subsequent swelling (Figure 2). One or two six-inch Kerlix large rolls (The Kendall Co., Mansfield, Massachusetts) were then applied over the cotton batting applying moderate compression, starting distally and continuing proximally (Figure 3). Pressure was applied in an increasingly firm manner as the Kerlix was advanced, creating a pressure gradient directed proximally that favors decreased lower extremity swelling as described by Yu et al. 5 A standard number 10 blade scalpel was then used to completely release the Kerlix anteriorly over the ankle using a vertical cutting motion, which eliminates any pressure point (Figure 4 and 5). This completes the first layer of the cast.
List of materials One Sterile Tubular Stockinette
The Kendall Co., Mansfield, Massachusetts.
3M, St. Paul, Minnesota.

All of the materials needed to apply the cast are shown here. The cotton batting is an essential component of this cast and should not be substituted.

Several layers of cotton batting are rolled over the sterile tubular stockinette. This layer should be applied loosely to accommodate postoperative swelling.

The Kerlix roll is applied by starting distally and advancing in a proximal direction with increasingly firm compression. This technique creates a pressure gradient that helps reduce swelling.

The Kerlix layer is released over the anterior aspect of the ankle using a scalpel with a vertical cutting motion.

Complete release of the Kerlix over the ankle is essential to eliminate a potentially painful pressure point.
A single layer of six-inch Webril Undercast Padding (The Kendall Co., Mansfield, Massachusetts) was applied over the Kerlix using firm compression. This layer helps to facilitate cast removal. Finally, three rolls of five-inch Scotchcast Plus fiberglass casting tape (3 M, St. Paul, Minnesota) were applied directly over the Webril, completing the final layer (Figure 6). No cast was bivalved. The final result is a cast that is bulkier than standard casts because of the increased amount of padding; (Figure 7). Finally, the tourniquet was released and distal perfusion was assessed. Patients were instructed to remain nonweightbearing or partial weightbearing, and serial examinations were performed on hospitalized patients until discharge. The length of followup for purposes of this study was 2 weeks unless an end-point was reached sooner.

A single layer of Webril undercast padding is applied directly over the Kerlix, followed by several rolls of fiberglass casting tape. The Webril facilitates easy cast removal.

Appearance of the completed cast construct. Note that it is somewhat bulkier than usual because of the thick padding.
A total of 38 patients were treated with the cotton-batting cast during the study period (Table 2). There were 21 women and 17 men with a mean age of 55 (range 15 to 80) years. Thirty-three of these patients had elective procedures, while five had traumatic injuries. Four procedures were performed outpatient, while the remaining 34 patients spent an average of days in the hospital (range 1 to 17). There were a total of 16 operations on the hindfoot alone, 10 on the ankle, and 12 involving both the hindfoot and ankle. Operations ranged from ankle fusion to open reduction and internal fixation of fractures to repair of ruptured Achilles tendons.
Patient data
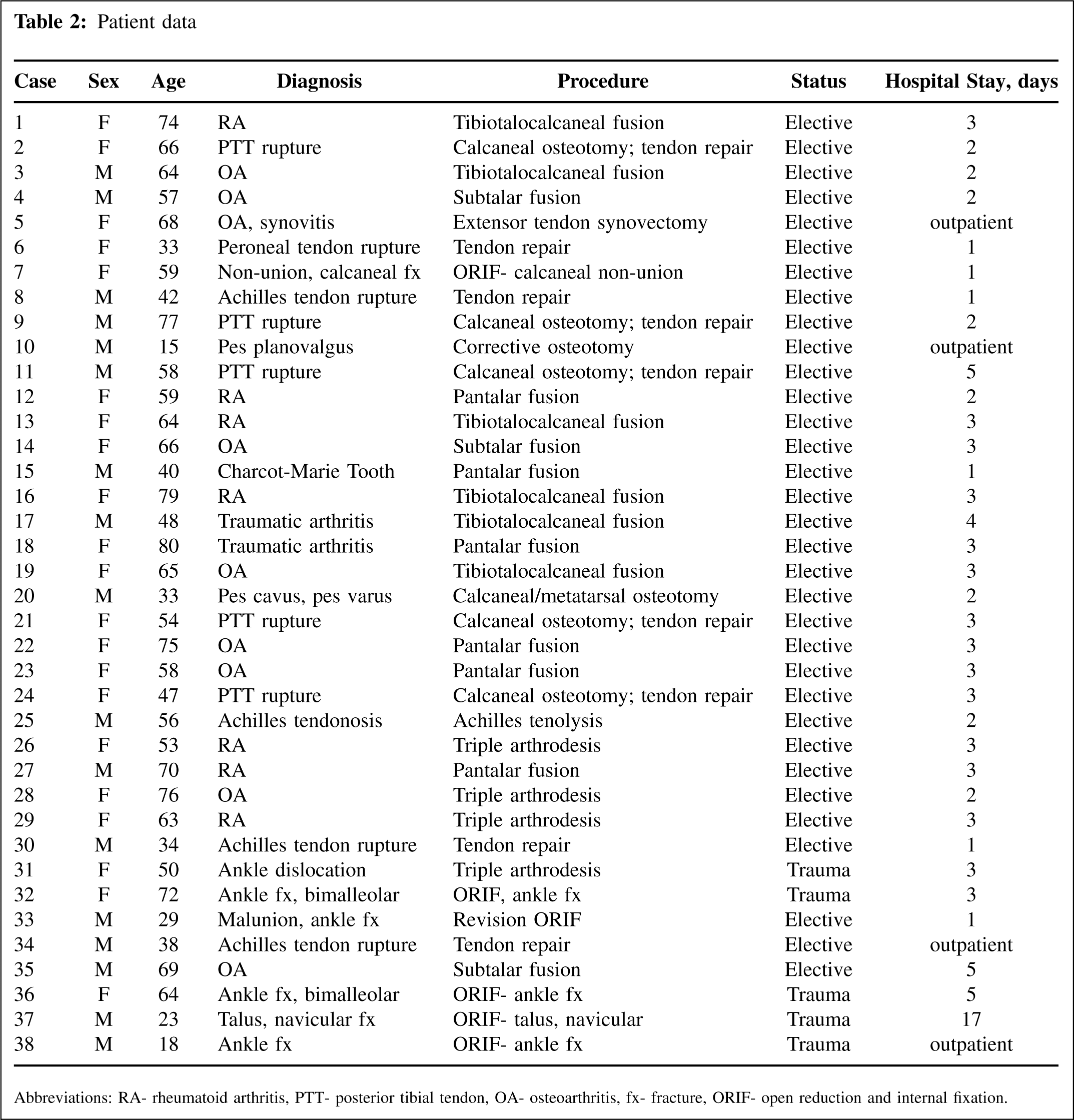
Abbreviations: RA- rheumatoid arthritis, PTT- posterior tibial tendon, OA- osteoarthritis, fx- fracture, ORIF- open reduction and internal fixation.
RESULTS
All patients in the study tolerated the cast for the 2-week postoperative period without the need for early cast removal. At the initial 2-week followup, all patients were personally examined by the surgeon who performed the operation (AC and NS). Several patients were noted to have typical mild to moderate swelling beneath the cast, but no complications were noted, and the cast seemed to accommodate the swelling well in all patients. There were no wound infections, no pressure ulcers, no wound dehiscence, and no signs of excessive swelling or compartment syndrome in any patients. There were no complaints of excessive pain, and there were no patients who required additional pain medication during the 2 weeks after placement of the initial cast. None of the patients in this study complained that the cast was uncomfortable or requested that it be removed early for any reason.
DISCUSSION
Despite continuous advances in surgical procedures to treat orthopaedic disorders, immobilization using a cast remains an integral and essential component of treatment. Casts are needed after surgery on the foot and ankle to maintain position and alignment and to prevent motion. However, typical casts are not suitable immediately after surgery because they are not able to accommodate significant swelling.
Some surgeons use a Jones dressing to avoid the postoperative problems caused by swelling and increased pressures beneath casts. The Jones dressing technique as reported by Brodell et al. 1 includes multiple layers of cast padding applied directly over the skin, followed by an elastic wrap, over which several additional layers of padding are applied with increasing pressure on the outer-most layers. For additional support, plaster splints are commonly applied, although Yu et al. 5 also reported successful application of both plaster and synthetic rolls over the Jones dressing for periods of up to 12 weeks without complications. In general, however, Jones dressings are removed and replaced after 3 to 5 days after surgery and are replaced with more durable short-leg casts. This makes an additional postoperative visit necessary and increases the costs associated with care, and may increase patient discomfort as dressing removal can be painful in the early postoperative period.
Another common solution to the problem of postoperative swelling is to apply a temporary plaster or fiberglass splint. Plaster splints are less expensive and easier to mold than fiberglass splints, but they are heavier, more difficult to apply, and become soggy when wet. Prefabricated splints made of plastic or fiberglass with foam or air cell linings also are available, although they generally provide less support than other splints and are more expensive. The principle behind all splints is to provide positional support without creating a restrictive space above the skin. This makes them a reasonable choice after surgery, but as with a Jones dressing, the patient must return soon after surgery to have a rigid cast applied, as long as significant swelling is not present. Again, additional costs are incurred, and the patient may experience additional discomfort.
The use of the cotton batting cast may be an effective, inexpensive method of producing sufficient immobilization after surgery. It is rigid enough to function as a cast but is designed to contain sufficient padding to accommodate any swelling that may develop. Our experience has shown this technique to be simple to apply, reliable, and safe for both elective and trauma surgeries on the foot and ankle. Because our inpatients spent an average of 3 days in the hospital, many of them would have required a new cast either on the day of discharge or just a few days later. Instead, we were able to monitor them in-house immediately after surgery, then safely discharge them without any cast change. This technique prevents the need for return visits shortly after surgery for replacement of the usual splint, and may be more cost effective since a temporary device is not needed and early followup is not necessary. There also are the theoretical benefits of patient comfort, skin care, and wound healing that may be derived from increased cast padding and decreased pressures within the cast, although this study did not consider those issues. It is important to note, however, that whenever there is any indication of a tight cast or increased compartment pressure, one should still be prepared to bivalve or remove this cast as necessary.