
Abstract
Background: The diagnosis of osteomyelitis of the foot in patients with diabetes mellitus remains a challenge. This study was conducted to evaluate bone infections using scintigraphy with instantly prepared single-vial kit, radio-labeled ciprofloxacin (Diagnobact TM) in comparison to a bacterial culture taken from the involved site. Methods: Twenty-five patients with type 2 diabetes mellitus having foot ulcers, including six with superficial ulcers and positive 99mTc-methylene diphosphonate (MDP) bone scan as a control, were subjected to 99mTc-ciprofloxacin scan and subsequent bacteriological culture. Results: 99mTc-ciprofloxacin scan was positive in 13 patients and negative in 12 patients, including the six with superficial ulcers. Bacterial culture was positive in 18 patients and negative in seven, including one with osteomyelitis on bone biopsy only. 99mTc-ciprofloxacin scan showed “true positive” results in 12, “true negative” in six, “false positive” in one, and “false negative” in six. The specificity and sensitivity of the test were 66.7% and 85.7%, respectively. The positive and negative predictive values and an accuracy of 92.8%, 50% and 72%, respectively. Staphylococcus aureus and Escherichia coli were the most frequently isolated organisms. Conclusion: 99mTc-ciprofloxacin is a sensitive and specific marker to diagnose bone infection in patients with diabetes mellitus, but care must be taken in case of fastidious organisms and ciprofloxacin-resistant bacterial flora in which false results may be obtained.
INTRODUCTION
India is the “diabetes capital of the world,” and at present has approximately 25 million patients with diabetes. 29 As in other developing countries, foot involvement is one of the most frequent problems in these patients, resulting in significant morbidity and mortality. 24 In earlier studies, we observed that foot sepsis contributed to 8% of in-hospital mortality. 2 , 33 The management and prognosis of affected feet in diabetes differ if there is underlying osteomyelitis with soft-tissue infection, as it runs a protracted course and requires prolonged antibiotic therapy. 20
Diagnosing osteomyelitis in the foot of a diabetic patient remains a difficult challenge. Routine radiographic techniques have low sensitivity. Furthermore, concomitant neuroarthropathy may hinder the radiological interpretations. 6 MRI is a sensitive but expensive method that is not available everywhere and cannot consistently differentiate soft-tissue infection from osteomyelitis. 32 Three-phase bone scans with 99mTc methylene diphosphonate (MDP) have 100% sensitivity but a low specificity when there is associated neuroarthropathy, traumatic fracture, or diabetic osteopathy. 10 Nuclear imaging with conventional agents like67 Ga-citrate, 99mTc or 111In-labelled leukocytes and new radiopharmaceuticals, such as radio-labeled monoclonal or polyclonal antibodies, are unlikely to meet the requirements for ideal imaging agents in such situations. 10 , 21 , 27 , 25 , 16 The inability to differentiate noninfective inflammation from infection by former agents and longer time of acquisition by the later agents are major limitations. Poor tissue perfusion from associated vasculopathy and high blood glucose levels impair the normal inflammatory response, wound healing, low granulocyte migration and, theoretically, poor distribution of radiopharmaceuticals. 22
Recent studies have reported high sensitivity and specificity of 99mTc-ciprofloxacin scan to diagnose bone and joint infections. 12 . 99mTc-ciprofloxacin meets most of the criteria described for an ideal infection imaging agent. It is less labor intensive, does not require blood handling during preparation, and unlike white blood cell-labeled agents is not taken up by normal bone marrow. 13 This prospective study assessed the efficacy of 99mTc-ciprofloxacin scan to establish the diagnosis of osteomyelitis in the foot of patients with diabetes.
MATERIALS AND METHODS
In this prospective study, 25 consecutive patients with type 2 diabetes mellitus having foot ulcer(s) with suspected underlying osteomyelitis were seen in the diabetic clinic of a tertiary care institute in north India from November, 2003, to May, 2004. The study was approved by the Institute's Ethics Committee, and informed consent was obtained from all patients. Inclusion criteria were type 2 diabetes mellitus of any duration and single or multiple foot ulcers or amputation stump ulcers with suspected osteomyelitis. Patients with a history of antibiotic, antimicrobial, or nonsteroidal anti-inflammatory drugs or steroid intake, or amputation or debridement in the previous 3 months were excluded. Those having limb-threatening or life-threatening infections requiring parenteral antibiotic and emergency debridement also were excluded. All patients were subjected to a detailed history, physical examination, relevant blood biochemistry, and appropriate radiographic investigations. Normal 99mTc-MDP bone scan rules out any infective or inflammatory process in the bone, hence there was no need of further investigations. A three-phase 99mTc-MDP bone scan was done in all patients and only those with positive MDP bone scan were studied further with 99mTc-ciprofloxacin scan and bacterial culture study for the involved site. Nineteen patients with deep ulcers (Wagner class III or more) with suspected osteomyelitis subsequently confirmed by bone biopsy, histopathology, or cultures were finally included in the study. Six patients with superficial ulcers with soft-tissue infection but no suggestion of bone involvement also had 99m Tc-ciprofloxacin scan before any intervention. These patients served as controls.
Radio Pharmaceutical
A single-vial kit of ciprofloxacin (Diagnobact™) obtained from the Institute of Nuclear Medicine and Allied Sciences (INMAS), Defense Research Development Council, New Delhi, India, was used for all the subjects. The preparation, radiochemical purity, animal experimentation, and the clinical utility of this radiopharmaceutical have been reported elsewhere. 15 . 99mTc-ciprofloxacin was prepared using a single-step method unlike the two-step method using stannus ion described previously. 29 The mixture was kept at room temperature for 15 minutes before use. Labeling efficiency of ciprofloxacin checked with chromatography was more than 90%. 99m Tc-MDP was prepared according to standard protocol and dose was approximately 700 Mbq (megabequerel).
Scintigraphic Imaging
Patients first had 99mTc-MDP scanning, followed by 99mTc ciprofloxacin imaging, with a gap of at least 3 days and at most 7 days between the scintigraphic procedures. Sequential scintigraphic images from areas of interest were obtained at 1, 4, and 24 hours after injection of 700 MBq of 99mTc-ciprofloxacin or 99mTc-MDP in at least two projections (dorsiplantar and lateral weightbearing). The acquisition parameters for each image were 500,000 counts in 256 × 256 matrix size. In all patients, 24-hour images also were taken, because radiotracer takes time to be washed out from the site of inflammation and target to nontarget ratio at 4 hours (T/N) is a less specific criterion. Images were recorded using a large-field-of-view (LFOV) camera fitted with a low energy, all purpose collimator (E-Cam, Siemens, Germany). Sites of osteomyelitis were determined from clinical examination, plain radiographs of the foot, as well as findings from positive 99mTc-MDP base scan taken in perfusion, blood pool, and delayed phases.
The scintigrams were visually evaluated by two nuclear medicine physicians independently (BRM and BS). In both 99mTc-MDP and 99mTc-ciprofloxacin scan, any area of abnormally increased tracer uptake in the suspected sites compared with surrounding healthy tissue or contralateral sites were noted. Increased or persistently increased activities of 99mTc-ciprofloxacin at 24 hours were taken as positive (Figures 1, 2, and 3). The scans were interpreted independently, and if there were disagreements in interpretation, the nuclear medicine physicians discussed their findings and reached a conclusion. Inconclusive data were excluded. At the time of interpretation, the readers were unaware of final diagnosis except the 99mTc-MDP bone scan report. All patients were monitored before, during, and after the nuclear scan. They were also told to report any adverse events during subsequent few days. Nineteen patients had bone biopsies with sterile technique to avoid chances of contamination. The specimens were subjected to both aerobic and anaerobic cultures and histopathology (Figure 4). In the other six patients with superficial ulcers who had 99mTc-ciproflaxacin scintigraphy, bone and soft tissue were taken for culture separately during debridement.
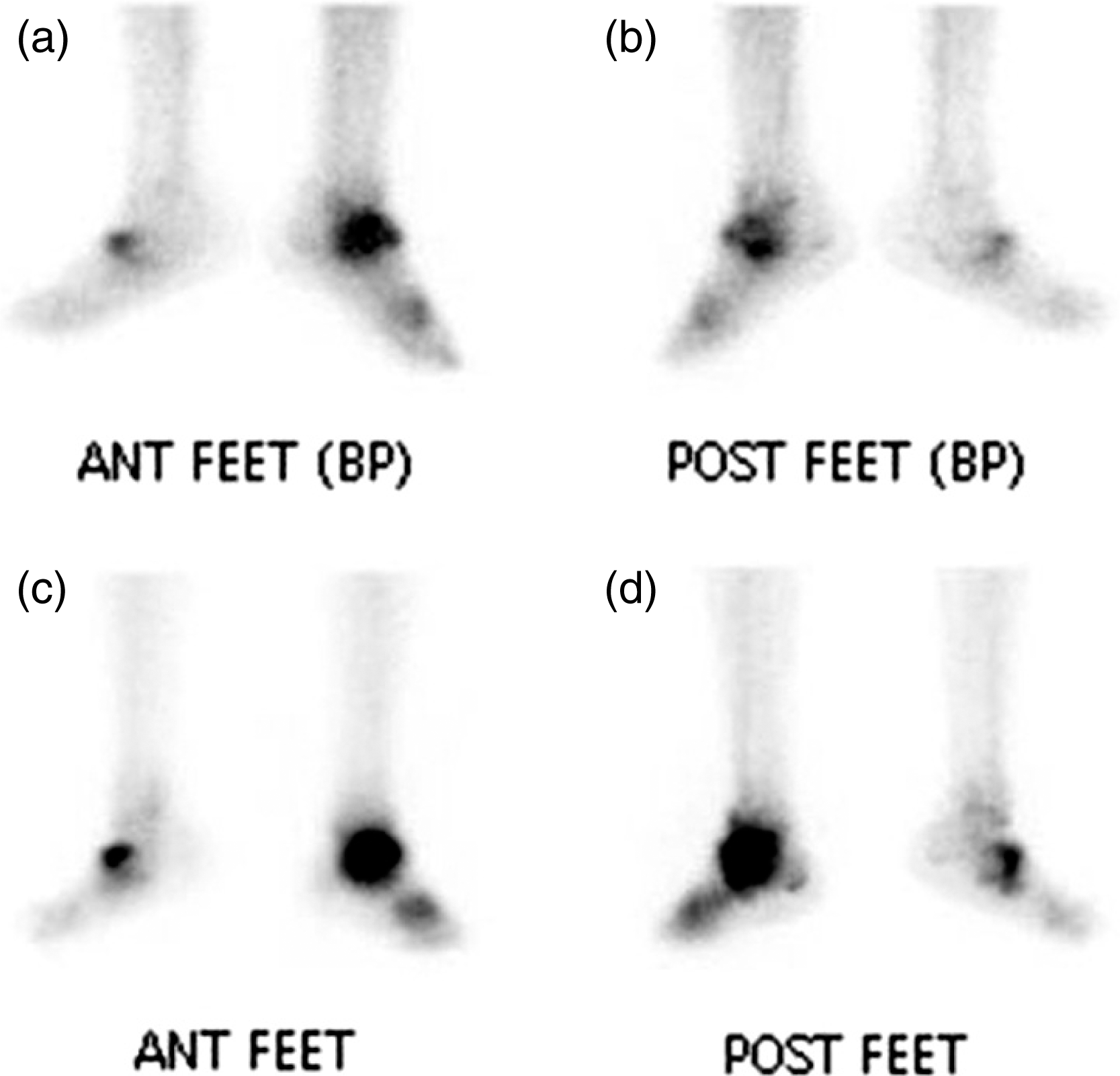
99mTc-MDP bone scan showing increased soft tissue (blood pool image, a—anterior, b-posterior) and bony uptake (delayed image c—anterior, d-posterior) of radiotracer.
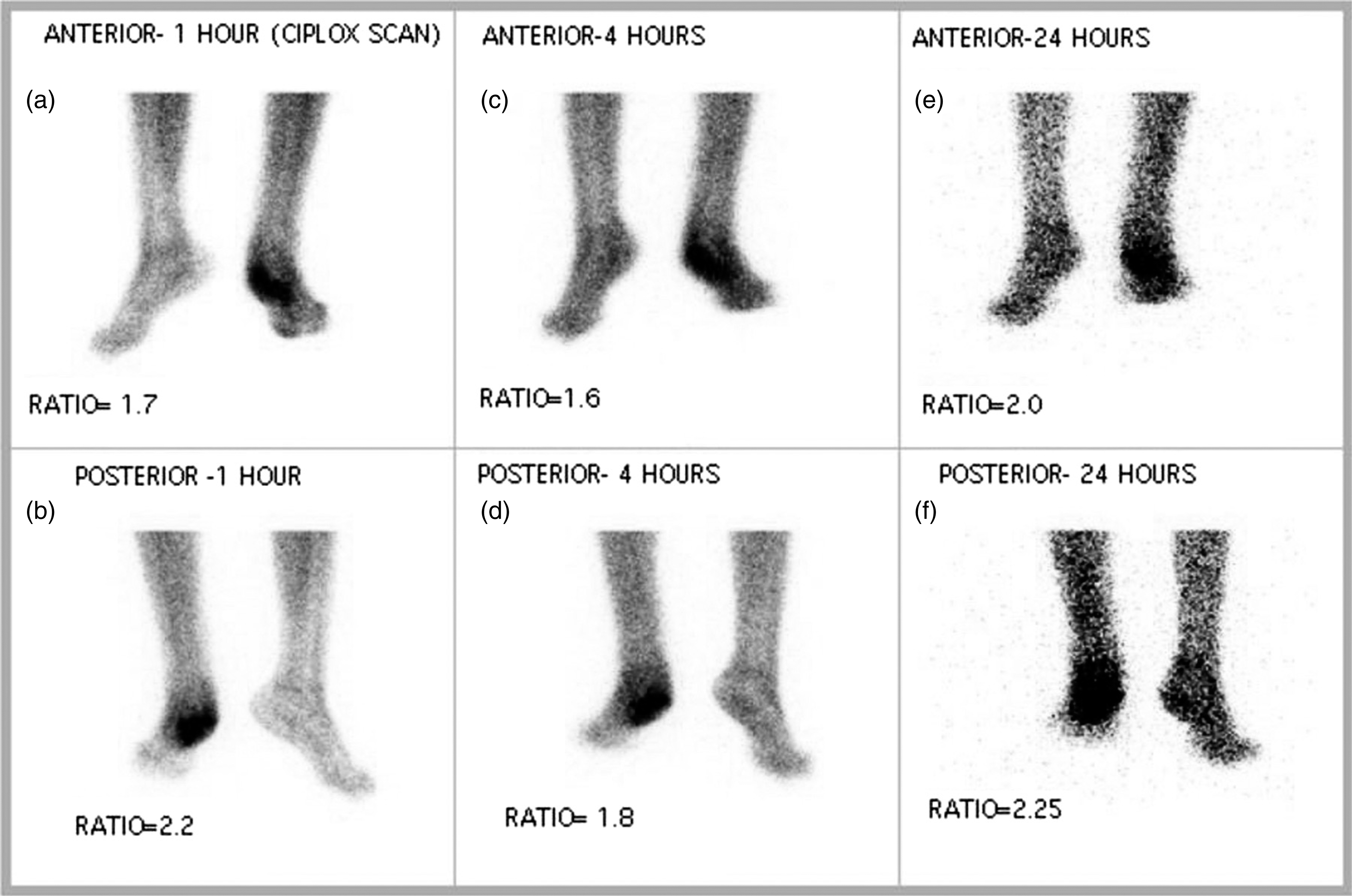
99mTc-Ciproflaxacin bone scan showing focal concentration of radiotracer at 1 hour (a, b), 6 hours (c, d) and 24 hours (e, f) in a patient with osteomyelitis.
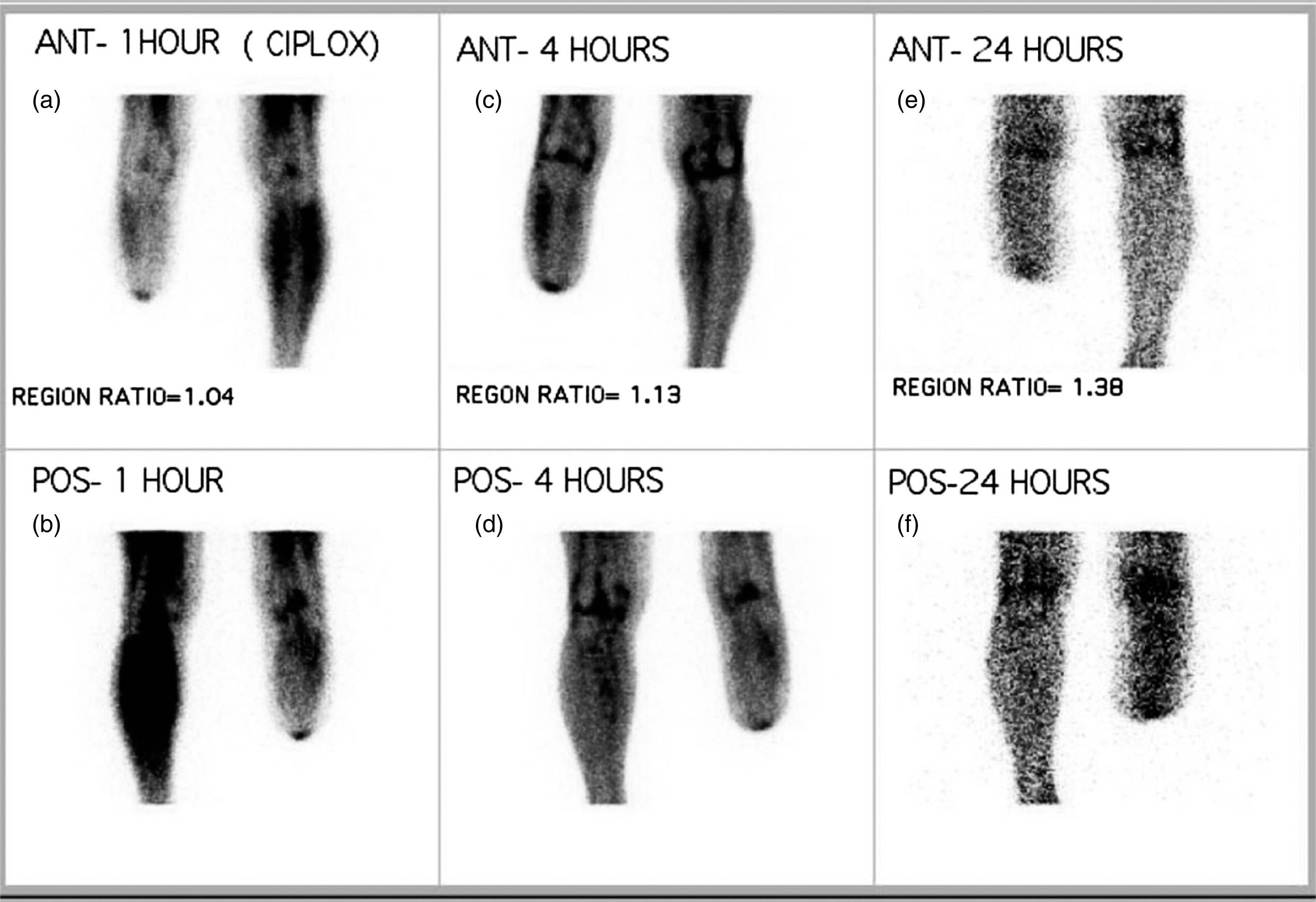
99mTc-Ciproflaxacin bone scan showing focal concentration of radiotracer at 1 hour (a, b), 6 hours (c, d) and 24 hours (e, f) in a patient with amputation stump osteomyelitis.
STATISTICAL ANALYSIS
The SPSS (Statistical Program for the Social Sciences, Release 10.0.1, PC Windows; SPSS Inc, Chicago, IL) was used for data analysis. Data were expressed as mean ± standard deviation (SD) unless specified otherwise. In addition to descriptive statistics, the Chi-square test was used for comparing proportions, and the Mann-Whitney-U test was used in comparing continuous variables. A p-value of less than 0.05 was considered statistically significant.
RESULTS
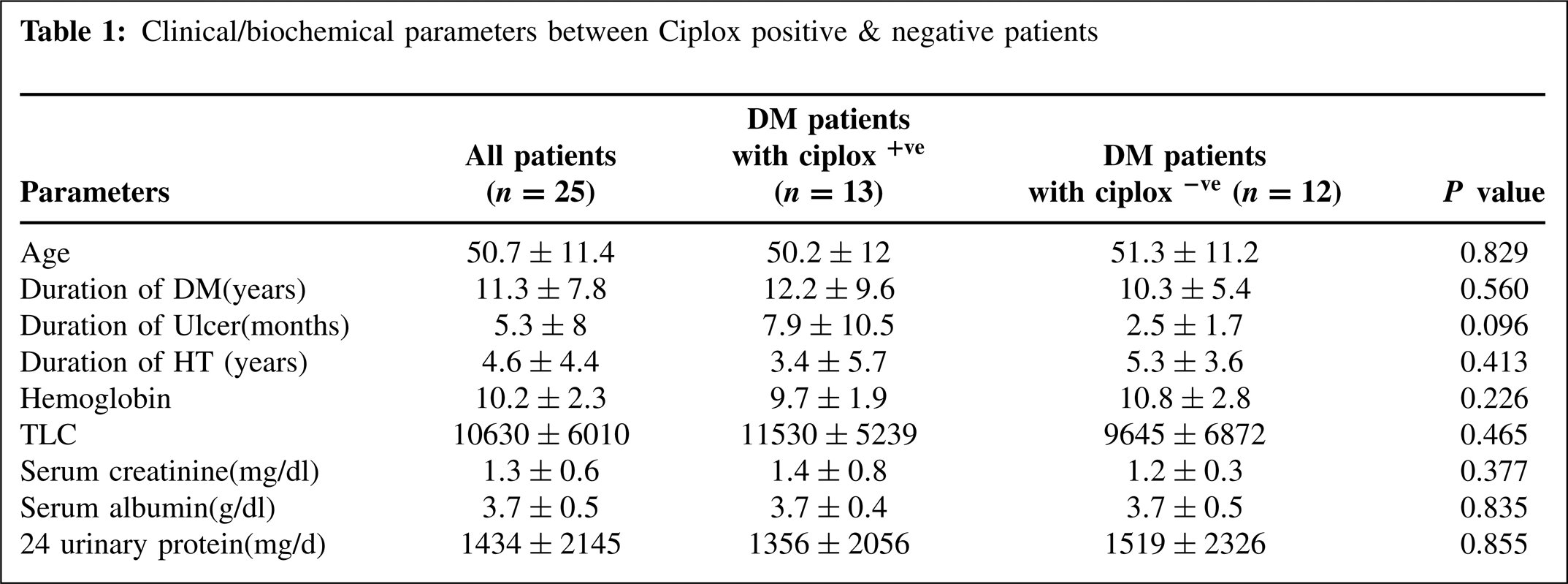
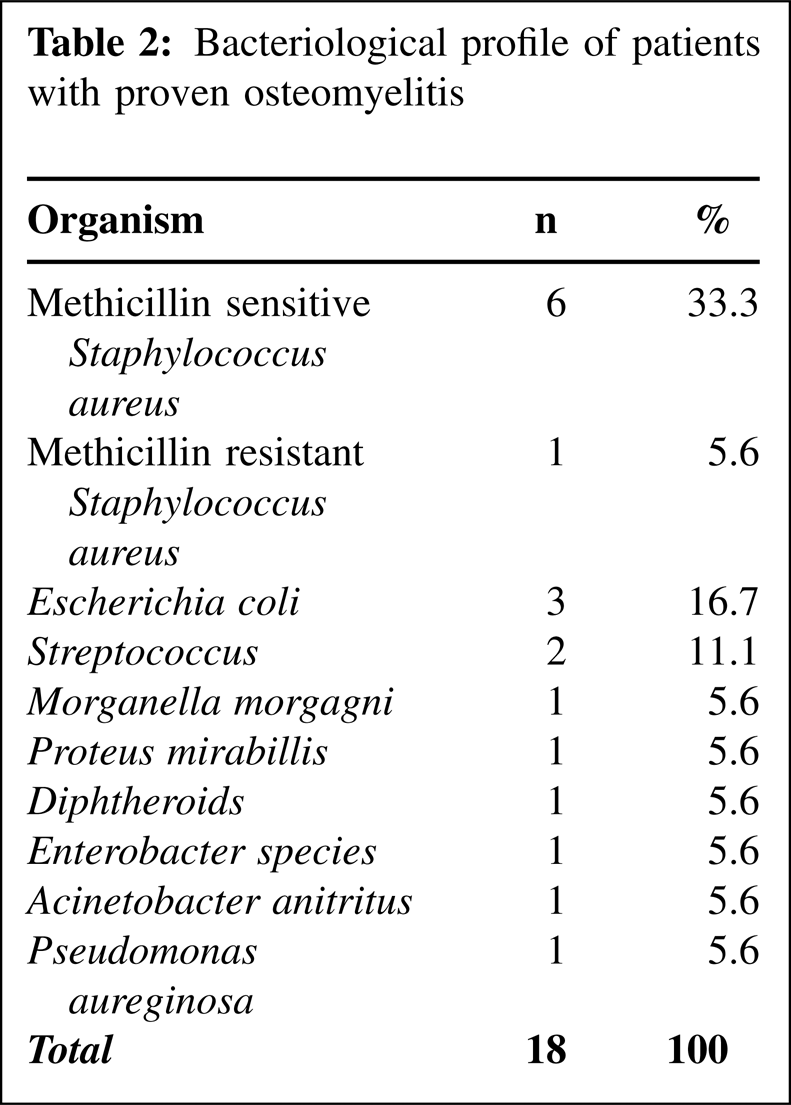
The mean age (±SD) of the patients was 50.7 ± 11.4 (range 20 to 70) years; duration of diabetes mellitus was 11.3 ± 7.8 (range 1 to 25) years. Sixteen of the 25 patients were hypertensive and 13 had clinical protein-uria (≥500 mg/day). The hemoglobin, serum albumin, and creatinine were 10.2 ± 2.3 gm/dl, 3.71 ± 1.47 gm/dl and 112.6 ± 56.3 μmol/L, respectively. In 14 patients (68%), the total leukocyte count was >12000/cumm. The mean duration of ulceration was 7.85 months, and other significant medical history in the population included smoking (eight), alcohol (17), neuropathy (24), nonproliferative retinopathy (18), proliferative retinopathy (three), peripheral vascular disease, clinical or Doppler (10), coronary artery disease (six), stroke (one), deformities or abnormalities in the arches of foot (seven), and neuroarthropathy (four). Twenty-one patients were on insulin and four were on oral hypoglycemic agents. Six patients received laser panretinal photocoagulation (three with proliferative and three with severe nonproliferative diabetic retinopathy). In these six patients, absence of bone infection was confirmed by radiographic followup for at least 3 months and healing of the ulcers without systemic antibiotic therapy was documented. Osteomyelitis was confirmed by bone biopsy culture in 18 and on the basis of histopathological changes only in one patient (Table 1). Staphylococcus aureus and Escherichia coli were the most frequently isolated organisms (Table 2). 99mTc ciprofloxacin scan was positive in 13 and negative in 12 patients including six with superficial ulcers. Only one patient had a negative culture but positive 99mTc ciprofloxacin scan (Table 3). Six patients had false negative ciprofloxacin scans, and one had a “false positive” ciprofloxacin scan.99mTc-MDP bone scan was concordant with ciprofloxacin scan in 13 patients (52%). 99mTc-ciprofloxacin scan was concordant with ciprofloxacin sensitive bacterial growth in 11 of 13 patients (78%), discordant in 2 of 13 patients (22%) so the accuracy of the test was 72%. The sensitivity and specificity of 99mTc ciprofloxacin scan were 66.7% and 85.7%, respectively. However, the positive and the negative predictive values were 92.8% and 50%, respectively (Figure 5). The 99mTc-MDP bone scan was highly sensitive (100%) but not specific (0%). When both these scans were combined, the sensitivity was 100% and specificity 85.7%. The factors predicting 99mTc-ciprofloxacin scan positivity included a history of previous amputation (r = 0.502, p < 0.05), longer duration of ulcer (r = 0.400, p < 0.05), underlying osteomyelitis (r = 0.585, p < 0.01), and positive bacterial growth (r = 0.471, p < 0.05).
Clinical/biochemical parameters between Ciplox positive & negative patients
Bacteriological profile of patients with proven osteomyelitis
Relation between 99mTc-ciprofloxacin scan and culture
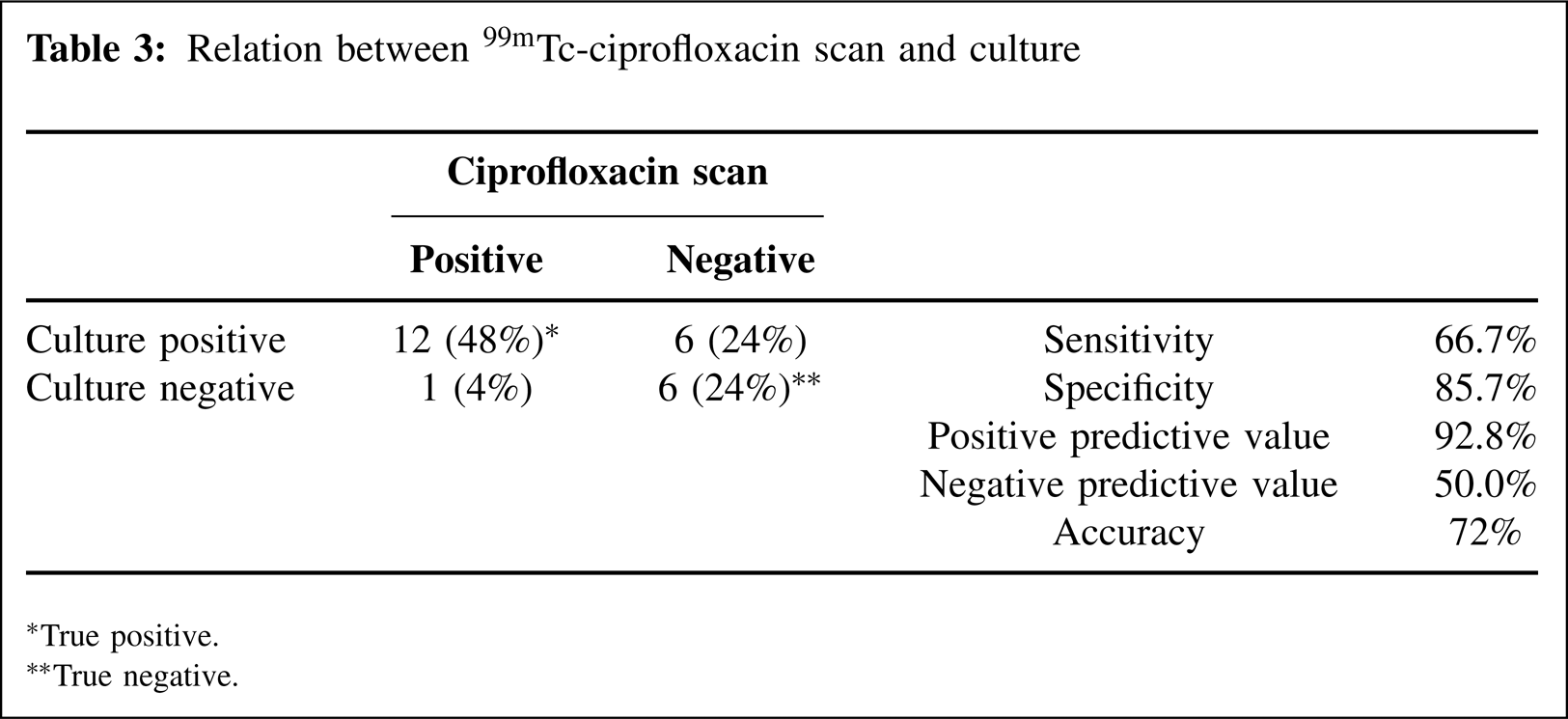
True positive.
True negative.
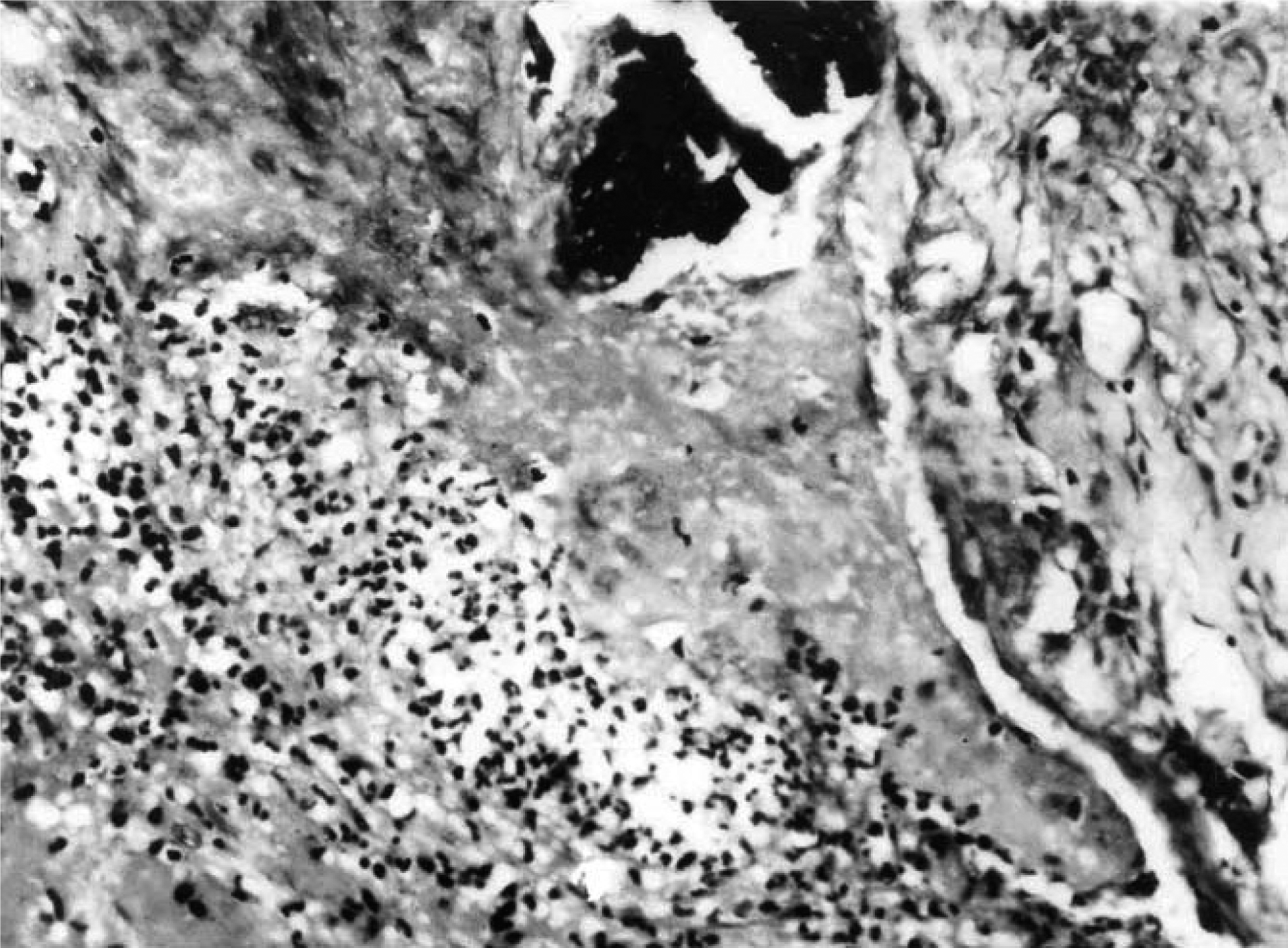
Photomicrograph showing dead bone fragments (black area) dense inflammatory infiltrates comprising of polymorphs and lymphocytes along with fibroblasts and proliferating capillary channels (H and E X 340).
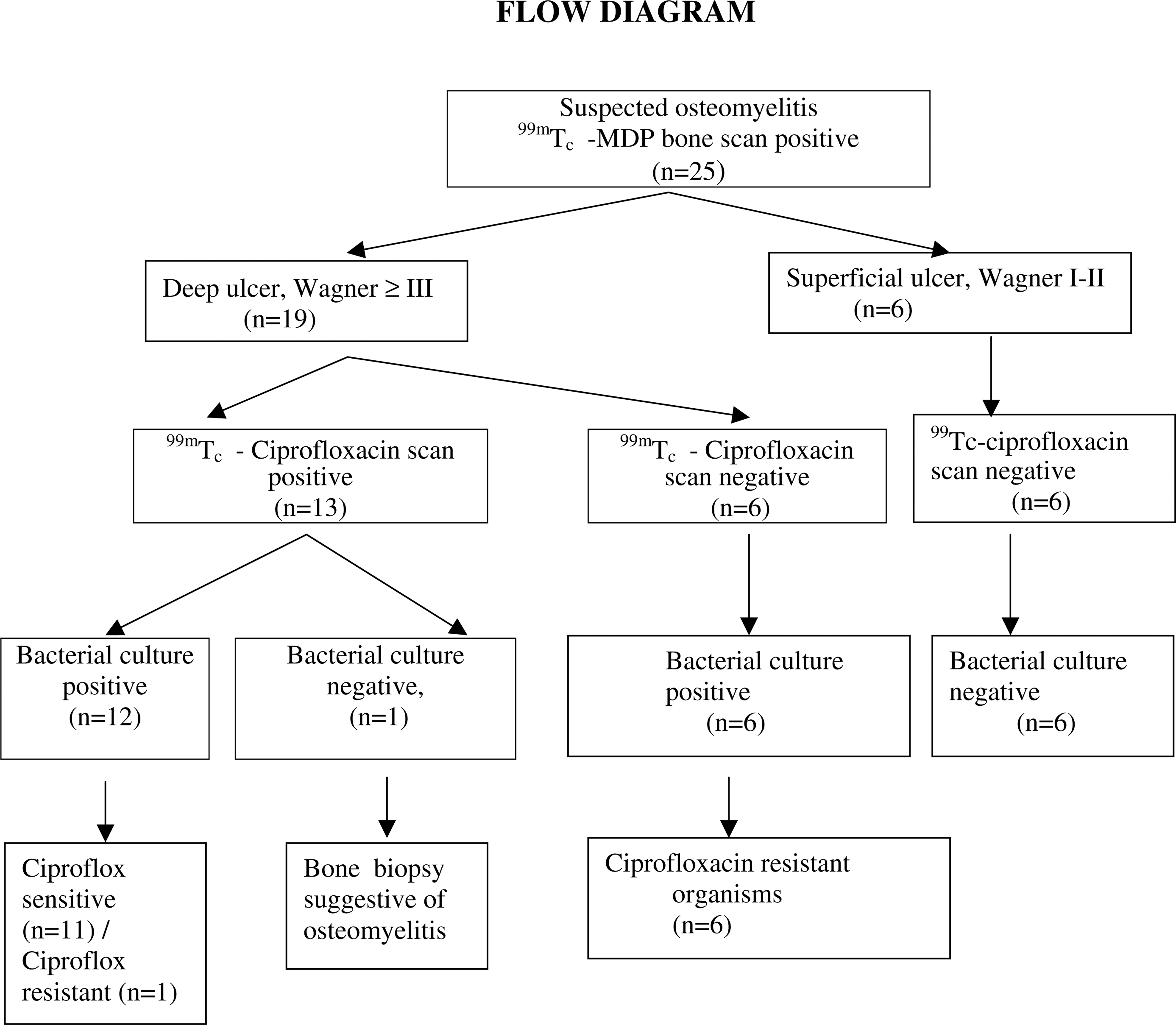
Flow diagram.
In all our patients antibiotics were advised only after appropriate specimens were obtained for bacterial culture and completion of ciprofloxacin scan. The specific antibiotics were administered based on the in-vitro susceptibility results. The duration of therapy was 4 to 6 weeks with 2 weeks of parenteral antibiotics in critically ill patients. At discharge, these patients were given appropriate oral antibiotics and were motivated to take regular therapy along with proper foot care. Debridement and a total contact cast were given to patients in whom they were indicated. Patients with Staphylococcus aureus and Pseudomonas infections that were positive on 99m Tc-ciprofloxacin scan with in vitro sensitivity to ciprofloxacin were given another appropriate drug to avoid resistance during therapy. Seven patients required amputation at various levels, and the others were managed conservatively.
DISCUSSION
This study confirms that 99mTc-ciprofloxacin scintigraphy combined with a 99mTc-MDP scintigraphy is effective in the diagnosis of osteomyelitis of the foot in patients with diabetes mellitus, with a sensitivity of 100% and specificity of 85.7% compared with bacteriological analysis.
Studies are available for 99mTc-ciprofloxacin scan in detecting septic foci and bone infection in nondiabetics. 3 , 14 , 18 , 28 , 30 However, to our knowledge, none of the previous studies specified the role of this scan in diabetics with underlying osteomyelitis. The major limitation of 99mTc-ciprofloxacin scan is poor spatial resolution unless combined with bone scan and multiprojection images, which were obtained in our patients. As 99Tc-ciprofloxacin alone cannot differentiate osteomyelitis from soft-tissue infection, this problem was partially was overcome by bone biopsy and histopathology in all patients (Figure 4).
Conventional diagnosis of osteomyelitis in patients with diabetes is based on clinical features, positive test on probing with a blunt forceps in the ulcer bed, and radiography. 11 The radiographic changes take 2 to 3 weeks to develop, and radiographic changes showing osteolysis, irregular bone destruction, and periosteal new bone formation also can be seen in neuroarthropathic feet and hence are nonspecific. 6 , 10 Considerable bone remodeling in neuroarthropathy limits the specificity of 99mTc-MDP scintigraphy. 10 Diabetic foot ulcers with osteomyelitis need more aggressive treatment, and the duration of antibiotic therapy is more prolonged as compared to soft-tissue infection. 7 , 20 The pattern of antibiotic treatment also requires bacteriological culture, which often is more time consuming, and if a proper sample is not taken, the bacterial flora may not be a true representative one. Appropriate microbiological studies in the form of samples from needle aspiration of pus in bone or soft tissues or a bone biopsy should be obtained for culture to guide therapy. 17
The radiopharmaceutical agent 99mTc-ciprofloxacin has been developed for improving specificity for diagnosis of infection in general and osteomyelitis in particular. 18 It consists of a synthetic broad-spectrum antimicrobial agent, ciprofloxacin attached to 99mTc. This agent combines the advantages of a 99mTc label and the broad spectrum bacterial localizing capacity of ciprofloxacin. After this combination it behaves as a small peptide, extravasates at the site of inflammation but stays for a prolonged period only when ciprofloxacin sensitive bacteria are present. 9 , 29 Gram-negative bacteria contain DNA-gyrase, and gram-positive bacteria contain topoisomerase IV responsible for negative super-coiling of DNA that helps in bacterial DNA replication. During the period of strand cutting, ciprofloxacin incorporated into the DNA prevents action of the above-mentioned enzymes and, thus, replication. Human DNA contains DNA topoisomerase II, which is not susceptible to this drug. 5 , 15 Initial in vitro studies and animal experiments have shown that ciprofloxacin localizes at high concentration at sites of infections caused by both Gram-positive and Gram-negative bacteria. 15 It has a special predilection for bones and joints 13 and does not localize to areas of sterile inflammation, abscess with dead bacteria. 30 Ciprofloxacin scintigraphy compared to white blood cells-labeled scans has shown greater specificity and precision, and it is negative in Charcot arthopathy. 23 It is not localized by normal marrow tissue, which is the greatest advantage over conventional white blood cells scans. 23 99mTc-MDP-bone scan alone can not differentiate infection from neuroarthropathy, traumatic fractures, hyperemia due to autonomic neuropathy. Hence a negative bone scan virtually rules out osteomyelitis in a diabetic foot but a positive one is inconclusive. 8 , 26 . 99mTc-ciprofloxacin scan combined with bone scintigraphy in our study had a specificity of 85.7% and sensitivity of 100%. These results are comparable to those reported in the literature. 4 , 18 These discrepancies in sensitivity and specificity are partly due to the inclusion criteria and different diagnostic criteria for osteomyelitis. One of our patients had a false positive scan (culture negative but scan positive), which could have been due to fastidious organisms, inflammation site edema with compartmentalization of extravasated radiopharmaceutical, or additional localizing mechanisms for 99mTc-ciprofloxacin. This was previously reported in patients with fibrous dysplasia, various inflammatory, and neoplastic bone diseases and at sites of excessive bone remodeling. 1 Transchelation appears to be the reason for 99Tc-ciprofloxacin's nonspecific uptake at metabolically active bone sites. Its 15% plasma protein bonding also may contribute to nonspecific localization in noninfected or minimally infected lesions. 1 In six of our patients there was bacterial growth, but 99mTc-ciprofloxacin scan was negative. In these patients the organisms were not susceptible to ciprofloxacin (Streptococci and methicillin resistant Staphylococcus aureus). The postulated mechanism of resistance in these organisms is mutation in chromosomal gene coding DNA gyrase or topoisomerase or active transport of the drug out of bacteria. 19 , 31 In one patient, there was growth of ciprofloxacin-resistant organism but the scan also was positive. This was previously reported by Britton et al. 4 This implies that 99mTc-ciprofloxacin scan may be positive in bacteria that have in vivo sensitivity but in vitro resistance.