
Abstract
Background:
Genetic hemochromatosis is a relatively common disease that may present as an arthropathy. In particular, arthropathy of the ankle is invariably bilateral and occurs in young men. However, the orthopaedic management of this condition has been poorly documented.
Methods:
Four patients with hemochromatic ankle arthropathy were treated with unilateral mobile bearing total ankle arthroplasty.
Results:
All four patients had good relief of symptoms after arthroplasty.
Conclusions:
Hemochromatosis should be considered when symmetrical ankle arthropathy occurs in a young man. Early diagnosis is necessary to prevent extra-articular progression of the disease and inappropriate management.
INTRODUCTION
The prevalence of hemochromatosis is 0.2% to 0.3% of Caucasian populations. 1 A characteristic arthritis is associated with hemochromatosis in approximately 50% of the patients with this disease and frequently is the first presenting feature of the disease. 1 However, although the arthritis associated with hemochromatosis is well documented in the rheumatology literature, little has been documented regarding the orthopaedic management of the disease, 4,7,8,11,16 particularly in the foot and ankle. 3,4,14 We present a case series highlighting the presentation and management of ankle arthropathy associated with hemochromatosis.
CASE REPORTS
Between 1998 and 2004, the senior author (TSS) performed five total ankle arthroplasties in four patients with bilateral ankle arthropathy secondary to genetic hemochromatosis. Informed consent was obtained from all patients.
Case 1
A 52-year-old Caucasian man presented with a 5-year history of bilateral ankle pain and swelling. The symptoms from the right ankle were intrusive enough to disturb sleep. The patient also complained of pain affecting the index and middle metacarpophalangeal joints of his dominant right hand and pain and stiffness in both hips. The diagnosis of hemochromatosis had been established at the age of 46 from genetic studies after the patient's brother had been diagnosed with the condition. Examination of the right ankle revealed neutral hindfoot alignment with 15 degrees of plantarflexion but complete loss of dorsiflexion. There was a valgus deformity of the left hindfoot, with a range of motion from 10 degrees of dorsiflexion to 20 degrees of plantarflexion. Generalized skeletal examination revealed multiple joint abnormalities (Table 1).
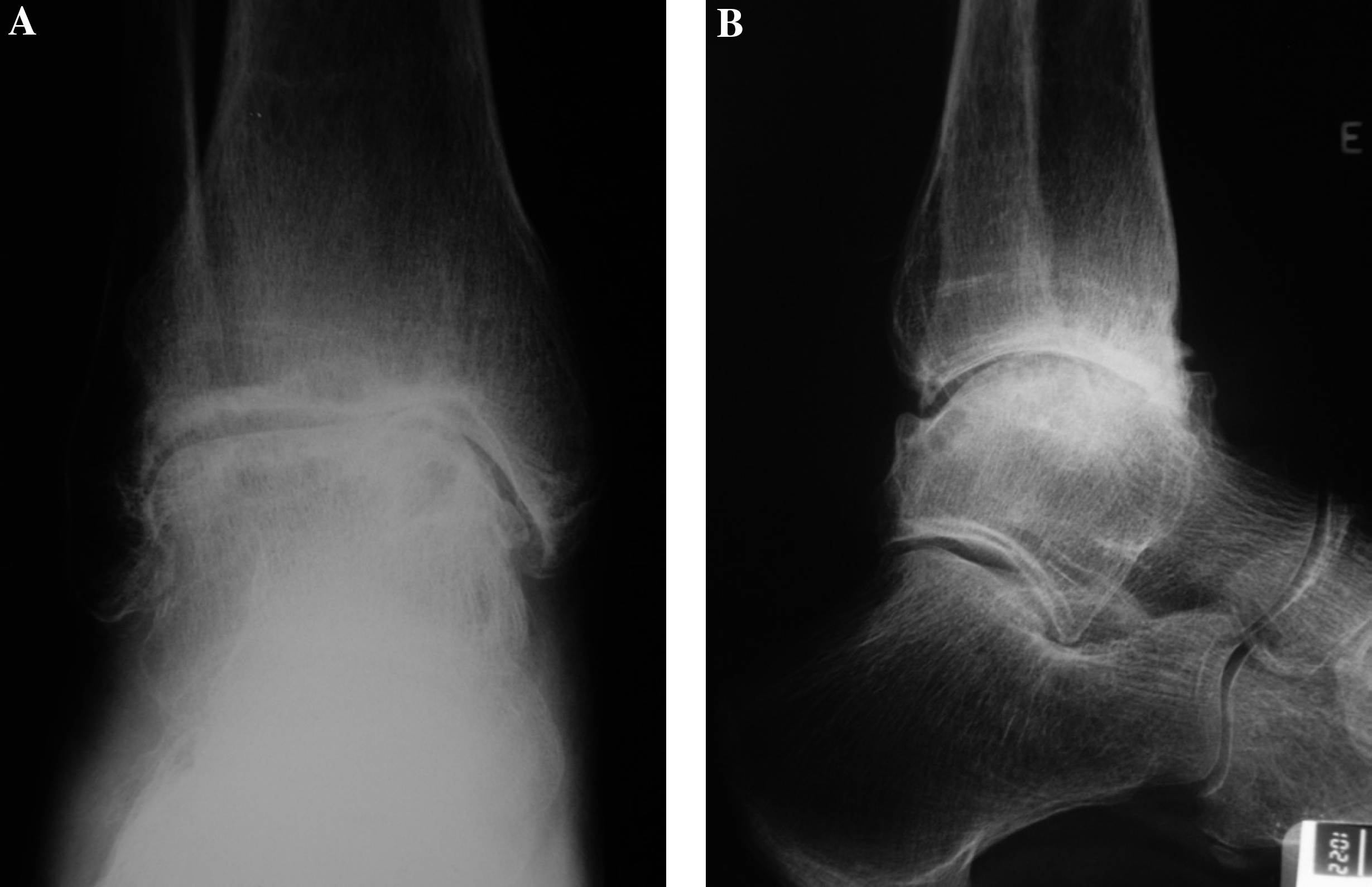
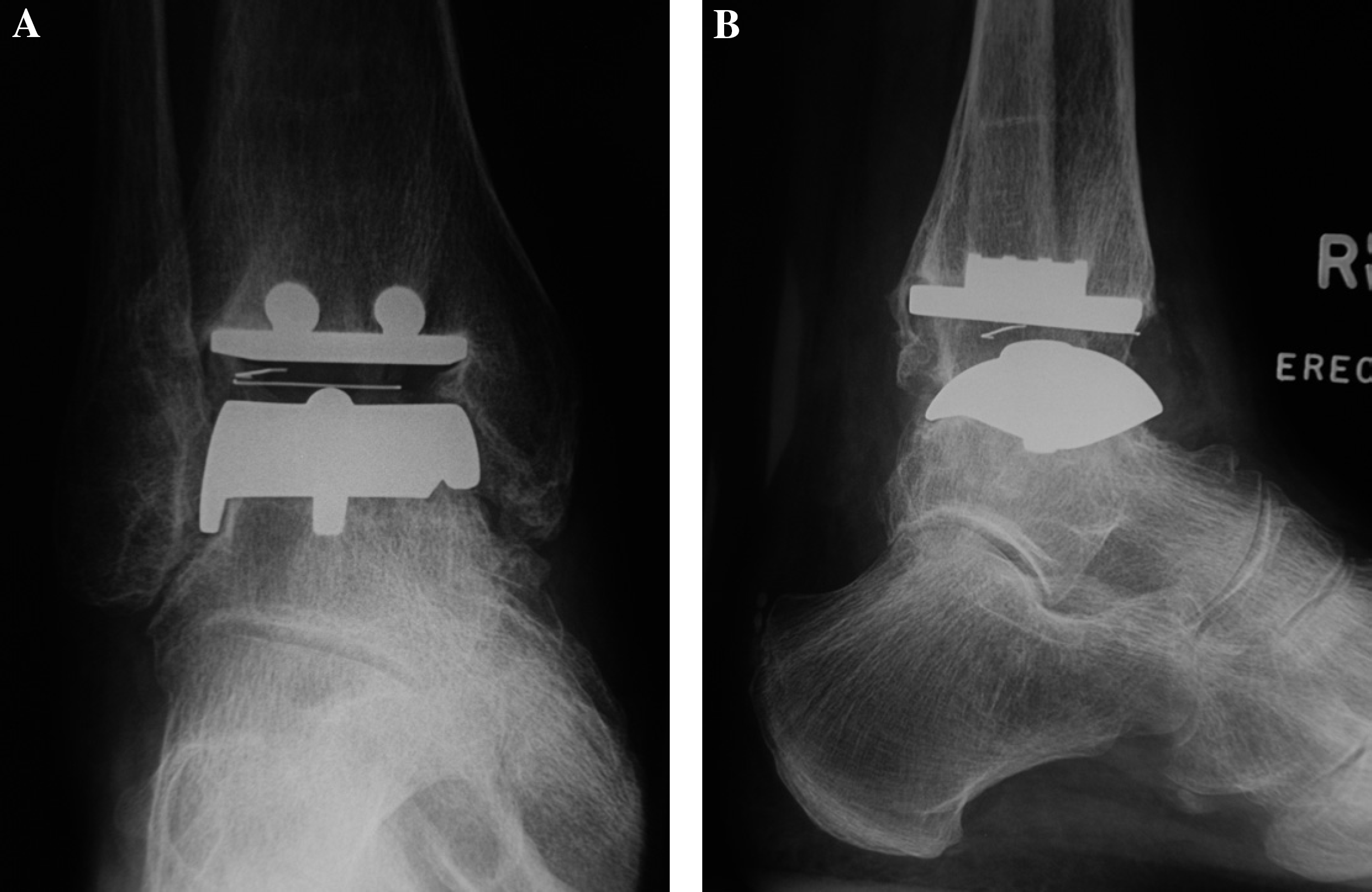
Radiographs revealed bilateral degenerative changes with-in the ankle mortise. The patient did not wish to try nonoperative measures and, in view of the symmetrical arthropathy, was offered the choice of a right-sided ankle arthrodesis or total ankle arthroplasty (Figure 1). After due consideration, the patient had total ankle arthroplasty (STAR, Waldemar Link, Hamburg, Germany). Three years postoperatively, the patient remained free of ankle pain (Figure 2) and was considering contralateral ankle surgery. A left total hip arthroplasty has since alleviated his hip pain.
Case 2
A 71-year-old retired, Caucasian man presented with bilateral ankle pain. Symptoms were worse in the right ankle and had been increasing for 10 years. He also experienced arthralgia in the ipsilateral knee. At the age of 65, he was diagnosed with hemochromatosis, and a liver biopsy revealed early cirrhosis. Four years later, he was diagnosed with hepatocellular carcinoma that was treated with a partial liver resection and was in remission at the time of consulting the senior author (TSS).
Clinical characteristics of four patients with hemochromatosis
Radiographs demonstrated degenerative changes in both ankles similar to osteoarthrosis. Because of the poor range of motion of both ankle joints, the patient elected to have a total ankle replacement (STAR, Waldemar Link, Hamburg, Germany) to try to restore motion. Symptoms were relieved by this procedure and a year later the patient had the same procedure on the contralateral ankle. At the last followup appointment, the patient remained free of pain and was independently mobile, but he died 3 years after the first ankle arthroplasty from recurrence of the hepatic malignancy.
Case 3
A 59-year-old Caucasian businessman presented with a 10-year history of worsening right ankle pain. Over the preceding months, pain had made weightbearing progressively more difficult and prevented the patient from managing his own business. At the age of 53, he had been diagnosed with symptomatic osteoarthrosis of his contralateral ankle and had undergone ankle arthrodesis with good results. The patient also complained of pain and stiffness affecting his right elbow and both hip joints. Pain and stiffness in his dominant right hand hindered his ability to unfasten lids on jars. Orthogonal radiographic views of his right ankle revealed gross degenerative changes as well as notable involvement of the tarsometatarsal complex.
After the diagnosis of hemochromatosis in his sister and as a consequence of abnormal serum iron studies, the patient had undergone genetic studies. At the age of 58, these studies confirmed the diagnosis of hemochromatosis.
Having exhausted nonoperative measures to control the symptoms from his right ankle, the patient elected for operative treatment. With the contralateral ankle arthrodesed, ipsilateral degeneration of the tarsometatarsal complex, and the requirement to manage his own company, the patient elected to have a total ankle arthroplasty (STAR, Waldemar Link, Hamburg, Germany). Although he sustained an intraoperative medial malleolar fracture, he remains pleased with the result 4 years later. Increasing symptoms from other large joints have required orthopaedic intervention and he has since had an unconstrained right total elbow arthroplasty and an uncemented right total hip arthroplasty.
Case 4
A 59-year-old Caucasian man, a civil servant, presented with a 3-year history of worsening bilateral ankle pain exacerbated by activity and unrelieved by orthoses or shoe modifications. The right ankle pain was associated with severe stiffness. At the age of 43, he had a liver biopsy that confirmed the diagnosis of hemochromatosis. Subsequent genetic studies confirmed the genetic nature of his disease. He had moderately severe pain affecting his left knee and his right first metatarsophalangeal joint. Examination revealed a severely limited range of right ankle motion with marked crepitus. Movement of the left ankle was less restricted. Radiographs showed severe degenerative changes in both ankles and early arthrosis of bilateral first tarsometatarsal joints.
Given the bilateral disease and his relatively sedentary occupation, the patient elected for a right total ankle arthroplasty (STAR, Waldemar Link, Hamburg, Germany). One year postoperatively, the patient remained free of pain. In the year since ankle arthroplasty, the patient's left knee symptoms increased sufficiently to require total knee arthroplasty.
DISCUSSION
Hemochromatosis is a generic term for a group of conditions characterized by pathologic deposition of iron in the parenchyma of many organs as a result of inappropriately elevated intestinal absorption of iron. Genetic, primary, or idiopathic hemochromatosis is an autosomal recessive genetic disorder associated with human leucocyte antigens A3, B7, and B14, 19 affecting men 10 times as often as women. 13 The common target organs are the liver, pancreas, heart, skin, and pituitary gland. As a result, patients are prone to cirrhosis and subsequent hepatocellular carcinoma, diabetes, and cardiomyopathy with a resulting diminished lifespan. Establishing a diagnosis before the development of cirrhosis or diabetes and beginning phlebotomy restores a normal life expectancy. 18
The characteristic arthropathy caused by abnormal deposition of iron within joints was first described in 1964 22 and typically presents in the sixth decade of life. Within synovial joints, the synovium and the tidemark region of articular cartilage are particularly susceptible to iron deposition. This makes the cartilage matrix stiffer and more predisposed to fragmentation. 16 In addition, iron salts promote the formation and precipitation of calcium pyrophosphate dihydrate crystals within the joint, leading to secondary chondrocalcinosis. 15 The combination of chondrocalcinosis with fragmentation of articular cartilage at the tidemark leads to subsequent joint degeneration. 2
Approximately 10% of patients experience arthralgia as the presenting feature of hemochromatosis. 1 On average, the arthritis presents 3 to 5 years before the diagnosis of hemochromatosis is established. 1,9 However, almost 50% of patients with the disease will have symptomatic arthropathy. 15 Frequently, this is a symmetrical polyarthropathy in men of working age. With the symmetrical pattern of arthropathy and occasional presence of subcutaneous nodules, hemochromatosis may mimic rheumatoid disease. 5 Radiographic evidence of narrowed joint space and cyst formation may prompt the diagnosis of osteoarthrosis, but osteophyte formation and sclerosis are much less common features. 13,23 Chondrocalcinosis associated with hemochromatosis is common in large joints. 10,13 The distribution of the arthropathy is the key to establishing the diagnosis. The joints most commonly involved are the index and middle metacarpophalangeal joints as well as the proximal carpal row, glenohumeral joint, hips, and knees. 8,13,15
Literature documenting the arthropathy of hemochromatosis in the foot and ankle is limited. Within the forefoot, involvement of the first metatarsophalangeal joint has been documented, 3,4,14 with one case treated operatively with an excision arthroplasty. 14 The medial column of the foot seems to be more prone to arthropathy, with disease documented in the first tarsometatarsal joint and articulations with the navicular. 3,4 Hemochromatosis arthropathy of the hindfoot most frequently involves the ankle mortise. The literature describes nine patients (eight men and one woman) with ankle arthropathy, 3,8,12,19,21 of whom three had bilateral disease. 12,21 The mean age at presentation of the patients in these studies was 52 (range 34 to 75) years. All three patients with bilateral disease were men of working age. When documented in the literature, the ankle arthropathy has been managed with anti-inflammatory medications, physical therapy or ankle-foot orthoses. 3,19 In one case, open debridement of the mortise was done. 8
The patients described in this series all had symptomatic bilateral ankle arthropathy. All were men with an average age of 60 (range 52 to 71) years at presentation. Although the diagnosis of hemochromatosis had been established before presentation, only two of the patients had been diagnosed with hemochromatosis before developing arthralgia. The remaining two patients had bilateral ankle arthralgia predating the diagnosis of hemochromatosis. In one patient, the diagnosis of hemochromatosis was established 5 years after ankle arthrodesis for the mistaken diagnosis of osteoarthrosis. The other patient had long-standing arthralgia before being diagnosed with hemochromatosis and died from extra-articular progression of the disease.
Bilateral ankle arthropathy poses a therapeutic challenge. Unilateral ankle arthrodesis remains a dependable procedure for relief of pain and has tolerable effects on gait. 17,20 However, unilateral ankle arthrodesis in the presence of midfoot arthritis seems to have a deleterious effect on gait 6 and midfoot arthritis may be a relative indication for arthroplasty. In addition, most orthopaedic foot and ankle surgeons prefer not to perform bilateral ankle arthrodeses because of the perceived detrimental effects on gait and functional outcome. Therefore, bilateral ankle arthropathy remains a sound indication for total ankle arthroplasty. These factors influenced the surgical management of all of the patients in this series. In each patient, a unilateral mobile-bearing total ankle arthroplasty was performed. In one case, a previous contralateral ankle arthrodesis together with ipsilateral degeneration of the tarsometatarsal complex influenced the patient's choice for arthroplasty. Because of good pain relief and preservation of ankle motion, one patient had a contralateral ankle arthroplasty. The two patients with untreated contralateral ankle arthropathy postponed further ankle surgery until they had recovered from other large joint arthroplasties.
Symmetrical ankle arthropathy in a young male patient should alert the orthopaedic surgeon to the diagnosis of hemochromatosis. Early diagnosis is crucial to prevent both extra-articular progression of the disease and inappropriate management for other causes of arthropathy. There is a role for unilateral ankle arthrodesis, but advanced cases of bilateral ankle arthropathy may be a relative indication for ankle arthroplasty.