
Abstract
Background:
Women wearing high-heeled shoes often complain of foot instability and low-back pain. Previous studies have demonstrated that using total-contact inserts (TCIs) in running shoes reduces impact on leg muscles and alters rearfoot motion. This study investigated how shoe heel height and use of TCIs in high-heeled shoes affect the wearer’s rearfoot complex, muscle loading, and subjective comfort.
Methods:
Fifteen inexperienced high heel wearers walked under 6 test conditions formed by the cross-matching of shoe insert (with and without TCI) and heel height (1.0, 5.1, and 7.6 cm) at a speed of 1.3 m/s. The measures of interest were rearfoot kinematics; muscle activities by electromyography (EMG) of the tibialis anterior (TA), medial gastrocnemius (MG), quadriceps (QUA), hamstrings (HAM), and erector spinae (ES); and subjective comfort rating by visual analogue scale for each test condition.
Results:
The statistical results showed that elevated heel height significantly increased plantar flexion (P < .001) and inversion (P < .01) at heel strike, prolonged TA-MG co-contraction (P < .001) and QUA activation period (P < .001), and increased root mean square (RMS) EMG in all measured muscles (TA, MG, QUA, ES: P < .001; HAM: P < .01). The use of TCIs reduced the rearfoot inversion angle (P < .01) and RMS EMG in both QUA and ES muscles (P < .01) and increased comfort rating (P < .001).
Conclusions:
These findings suggest that wearing high-heeled shoes adversely affects muscle control and reduces loads in QUA and ES muscles.
Clinical Relevance:
The use of a TCI may improve comfort rating and foot stability.
Surveys of shoe choice show that 37% to 69% of women regularly wear high-heeled shoes.13,39 However, epidemiological studies show that high-heeled shoes are implicated in almost 60% of foot problems in women.7,8,13 Such problems include forefoot pain and hallux valgus,7,23,24 metatarsalgia and calluses,10,24 and ankle sprains. 28 Wearing high-heeled shoes results in a smaller and unstable supporting base, which then alters the structure of the lower extremities and diminishes the shock-absorbing and weight-supporting functions of the foot.3,5,6 Studies also show that high-heeled shoes cause postural alterations such as excessive plantar flexion and inversion motion at the ankle.15,35 During walking, such alterations can increase metabolic cost 11 and muscle loading17,38 and can accelerate muscle fatigue. Accelerated muscle fatigue may then impair foot stability and increase the risk of ankle sprains11,15,36 or even lead to a fall.11,16
Comfort is a major concern in the choice of footwear. Increasing interest in footwear comfort motivated several studies of the link between discomfort and biomechanical factors in wearing high heels, such as postural alterations,13,36 increases in leg and low-back muscle activities,1,21,37 and plantar pressure distributions.18,22 Research findings suggest that reduced muscle activity and biomechanical alterations may help decrease discomfort.6,18,25,29 A subjective visual analogue scale (VAS) has proven reliable for assessing footwear comfort 25 and was combined with biomechanical measures to determine the effectiveness of inserts in high-heeled shoes. 18
Shoe inserts are widely used in footwear to increase comfort and to reduce the frequency of movement-related injury.27,34 Total-contact inserts (TCIs) are made according to the individual plantar geometry of a wearer’s foot combined with accommodative arch-support and heel-cup mechanisms. Customized TCIs can reduce leg muscle loading and increase lower extremity joint stability in flat or casual shoes.5,27,34,40 Lee and Hong, 22 who examined the effectiveness of different insert types for high-heeled footwear, found that the TCI is both comfortable and effective in reducing impact force and forefoot pressure. However, TCIs used in high-heeled shoes have not been evaluated in terms of the effect on muscle loading and foot stability.
Muscular loads while walking can be adequately measured by electromyography (EMG). 9 Analyses of loading by major leg muscles may shed light on the cause of discomfort experienced by those wearing high-heeled shoes. High muscular load causes fatigue, whereas co-contraction of lower leg muscles stabilizes the ankle joint at heel strike and contributes to foot stability during the early stance phase. 33 Nevertheless, few studies have reported EMG values for lower limb muscles while subjects are walking in high-heeled shoes.17,21
Analysis of rearfoot motion during walking was used as an index of foot stability by Snow and Williams. 36 Such analysis is important for evaluating potential factors related to inversion injury of the ankle. 4 This study investigated the effect of heel height and TCIs on muscle loading and foot stability while walking. Surface EMG and rearfoot angle measurements were integrated to analyze the effects of muscle loading on the foot and the structural stability of the foot. The objective was to determine the effects of heel elevation and TCI use on muscle activities in the leg and lower back and on foot stability during walking. This study hypothesized that heel elevation can increase EMG activities in leg and low-back muscles, prolong activation periods in quadriceps and co-contraction periods in the tibialis anterior–medial gastrocnemius muscles, increase plantar flexion and inversion motion at the rearfoot, and reduce VAS comfort rating. The TCI was hypothesized to have reverse effects from heel elevation on muscle loading, foot stability, and subjective comfort.
Methods
Subjects and Materials
Fifteen Taiwanese female adults were recruited for this study. Subject average age was 24.5 years (range, 20-30 years), average weight was 49.6 kg (range, 44-57 kg), and average height was 159.3 cm (range, 155-168 cm). No subject suffered from a neuromuscular or musculoskeletal disorder. All subjects claimed they were inexperienced high-heeled shoes wearers (fewer than 2 times per month). This study was approved by the local institutional review board (China Medical University Hospital), and all subjects signed the informed consent.
The shoes in this study were commercially available and selected based on similarity of foot contact points, support, and pump style (closed back, low-cut front, and without laces, buckles, straps, or ties). The main difference among these shoes was heel height (1.0 [flat shoes], 5.1, and 7.6 cm). A pair of TCIs was custom fabricated for each subject. For fabrication steps, refer to the study by Lee and Hong. 22 The TCIs were made of Multiform (AliMed, Inc, Dedham, MA) which is a thermoformable, cross-linked polyethylene foam. The Multiform density provides good support and cushioning. 20 To prevent tightness in the toe box, each TCI was designed to terminate at the distal border of the metatarsal heads (Figure 1). To reduce sliding between the inserts and the shoes, the inserts were fixed firmly in place using thin double-sided tape.
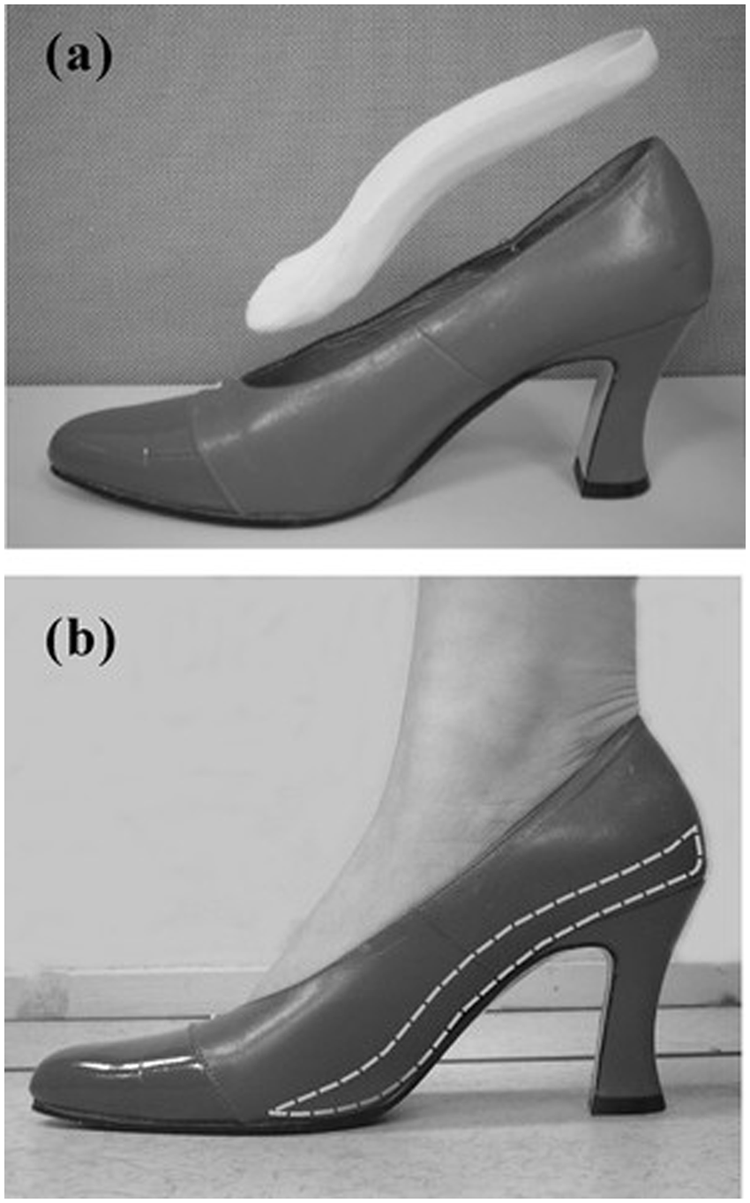
Illustration of (a) a total contact insert (TCI) and a high heel shoe with a 7.6-cm heel height. (b) A scheme demonstrating a TCI placed in a high heel shoe.
Experiments
A motion analysis system (Vicon 370; Oxford Metrics Ltd, Oxford, UK), 2 force plates (AMTI; Advanced Mechanical Technology, Inc, Watertown, MA), and an EMG system (MA-100; Motion Lab Systems, Inc, Baton Rouge, LA) were integrated to collect kinematic and EMG data simultaneously. The Vicon 370 system has 6 infrared cameras that acquire kinematic trajectories of reflective markers attached to a subject’s lower limbs at a rate of 60 Hz. The force plate system was used to measure foot–floor reactions to define the phases of a gait cycle. The MA-100 system was used to measure activities of the tibialis anterior (TA), medial gastrocnemius (MG), quadriceps (QUA), hamstrings (HAM), and erector spinae (ES) muscles via surface electrodes at a rate of 960 Hz. The centers of the surface electrodes were longitudinally located at the point of recommended insertion of needle electrodes according to Perotto et al. 30
The rearfoot and lower leg of each subject were modeled as 2 rigid segments according to the method described by Allinger and Engsberg. 2 Movement of the rearfoot and leg segment was defined by 2 ‘T’ shaped plastic bars with each bearing 3 markers (Figure 2). One T-bar was attached to the posterior counter of the shoe, and another was attached on the posterior shank to avoid artifact introduced by skin movement. Additional markers were placed on toe position for subsequent use in determining gait cycle events (Figure 2).
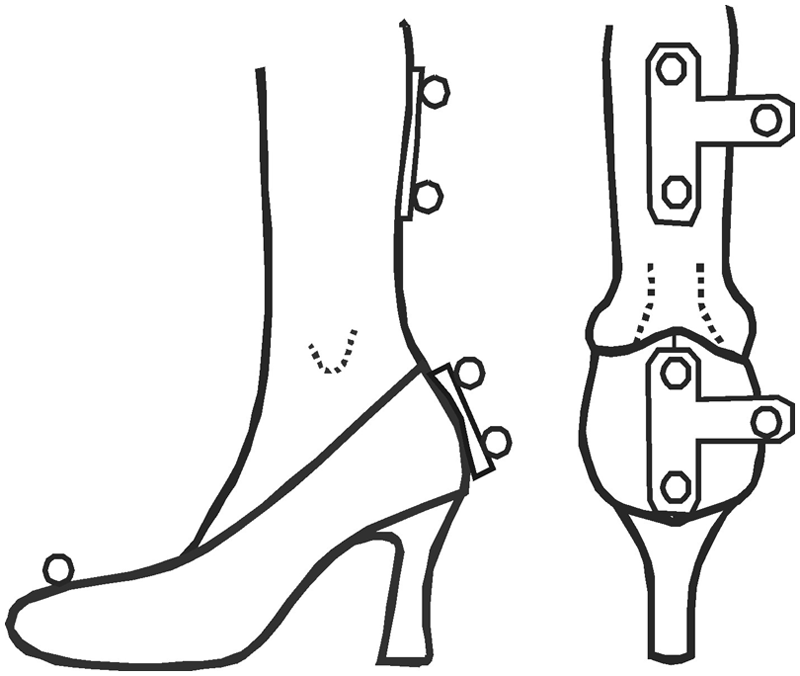
The marker set used to define rearfoot and leg segments.
The VAS developed by Mündermann et al 26 was used to assess footwear comfort. Comfort was rated by a ruler that consisted of a 100-mm VAS with the left end of the scale labeled “not comfortable at all” (0 comfort points) and the right end labeled “the most comfortable condition imaginable” (10 comfort points). Each subject was required to exclude the consideration of shoe cosmetics from her rating.
Procedures
Test conditions cross-matched 2 shoe inserts (noninsert and TCI) and 3 heel heights (1.0, 5.1, and 7.6 cm). The order for use of different heel heights was randomized for both noninsert and TCI conditions. Before the first test, participants walked on a treadmill for 5 minutes at 130 cm/s to become habituated to heel height and walking speed. During this period, an investigator set a metronome to the preferred stepping frequency of each subject to ensure that the subject maintained the same stepping frequency in subsequent tests. This control was intended to ensure that any observed gait changes did not result from different average walking speeds. For each subject, posture was analyzed while the subject wore the flat shoes with no insert condition while standing still for 3 seconds to establish the neutral (zero) position and to calibrate local coordinate systems at the rearfoot and lower leg. Afterward, participants rated the comfort VAS for each insert and heel height combination.
Data Analysis
Analysis software programmed using LabView 7.1 (National Instruments, Austin, TX) was applied to compute rearfoot angles and EMG magnitudes from acquired data.
Rearfoot Complex
A calibration matrix, the rotational matrix between the rearfoot and lower leg coordinate systems, based on flat-shoe standing posture was computed for each participant to calculate joint angles relative to those of neutral posture under each test condition. Euler angles were used to document rotational movement of a rearfoot relative to the lower leg. The plantar flexion–dorsiflexion angle was defined as the anterior–posterior rotational angle of a rearfoot in the sagittal plane relative to the lower leg. The inversion–eversion (supination–pronation) angle was defined as the tilt angle of a rearfoot in the frontal plane relative to the lower leg in the medial–lateral direction. Adduction–abduction angles were defined as the medial–lateral rotational angle of a rearfoot relative to the lower leg in the transverse plane. The instants of heel strike (HS) and toe-off were determined as the lowest point in the vertical trajectory of the posterior counter of shoe and toe markers, respectively. The selected variables of rearfoot motion were based on definitions by Snow and Williams. 36 These variables were as follows: (1) dorsiflexion–plantar flexion at HS; (2) maximal plantar flexion angle during loading response (0%-10% of the gait cycle) 31 ; (3) maximal dorsiflexion angle during preswing (50%-60% of the gait cycle) 31 ; (4) range of dorsiflexion–plantar flexion during stance phase (SP); (5) inversion angle at HS; (6) maximal eversion angle during preswing; and (7) range of inversion–eversion during SP. Figure 3a shows these variables on typical angle waveforms of a rearfoot.
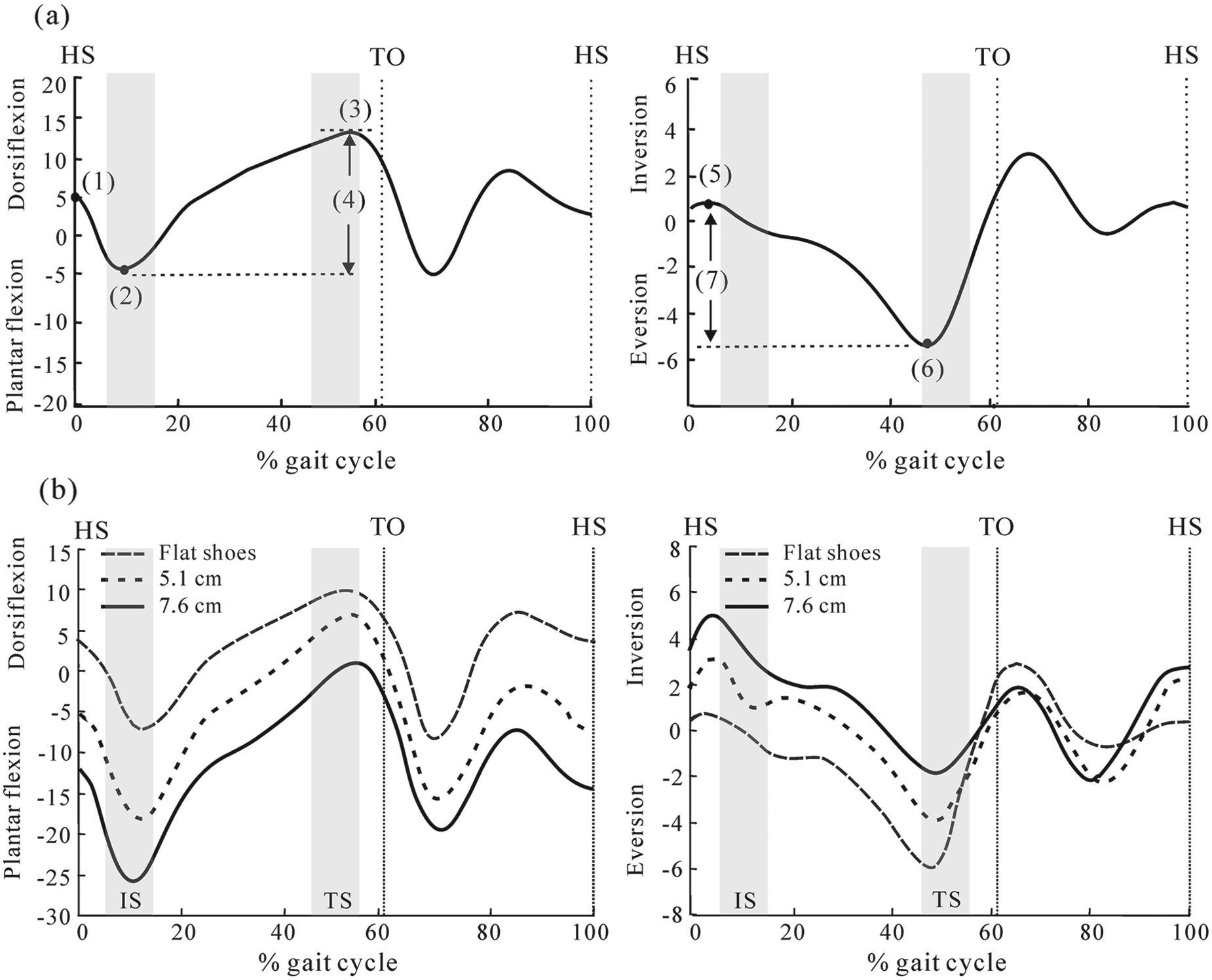
(a) Representation of analytical variables for rearfoot kinematics: (1) dorsiflexion angle at heel strike (HS); (2) maximal plantar flexion angle during loading response (LR); (3) maximal dorsiflexion angle during preswing; (4) range of dorsiflexion–plantar flexion during stance phase (SP); (5) inversion angle at HS; (6) maximal eversion angle during preswing; (7) range of inversion–eversion during the SP. (b) The mean angular motion of the rearfoot for different heel heights without inserts during walking. TO, toe-off.
Electromyography
The linear envelope of each muscle EMG was calculated by full-wave rectification of the raw EMG signal and then filtering of the rectified signal through a second-order Butterworth low-pass filter (5 Hz cutoff) using LabView analytical software. The peak EMG amplitude of each muscle at HS (0%-5% gait cycle), which was determined from the linear envelope and root mean square (RMS) EMG of each muscle during a full gait cycle, was chosen as an index for muscle loading analysis. For the TA, MG, and QUA muscles, the greatest EMG peak amplitude among 3 heel heights was first determined and its 20% value was defined as the activating threshold of the corresponding muscle. 3 If both TA and MG muscles were activated, the time period was considered the co-contraction period at the ankle joint. The overall co-contraction period at the ankle joint and activation period of the QUA muscle in each trial were recorded for statistical analysis. The TA-MG co-contraction period and QUA activation period were represented as a percentage of gait cycle (GC).
Statistical Analysis
Analytical variables included rearfoot angles, TA-MG co-contraction, QUA muscle activation periods, RMS EMG in a gait cycle, peak EMG value at HS for each muscle, and comfort rating. Statistical analyses used SPSS 10.0 (SPSS, Inc, Chicago, IL). Two-way analysis of variance (ANOVA) for repeated measures (3 heel heights × 2 insert conditions) was used to assess the effects of heel height and shoe insert on these variables. The level of significance was P < .05. If an insert condition had a significant effect on peak EMG at HS, multiple paired t tests were conducted to compare the difference between noninsert and TCI use at each heel height; the significance level was corrected using the Bonferroni method. Pearson’s correlation coefficient was used to assess the relationship between comfort rating and EMG and angle parameters.
Results
Electromyography
Co-contraction occurred when both agonist and antagonist muscles were activated simultaneously. For the flat shoes condition, TA and MG muscles co-contracted only in SP. For the 5.1-cm and 7.6-cm heel height conditions, TA and MG muscles co-contracted in SP and swing phase. Both the QUA and HAM muscles contracted from terminal swing and continued to loading response. Two bursts of ES activity existed, one at HS and one at toe-off. The ANOVA results indicate that the TA-MG co-contraction period (F = 74.9, P < .001), QUA activation period (F = 60.2, P < .001), and RMS values of all muscles increased significantly as heel height increased (F = 7.0-46.8, P < .01) (Table 1). The use of a TCI effectively reduced the QUA activation period, RMS QUA, and RMS ES (QUA activation period, F = 12.2, P < .01; RMS QUA, F = 22.5, P < .001; RMS ES, F = 23.5, P < .001). When compared with the noninsert condition, use of a TCI in the 7.6-cm heel height condition reduced the QUA activation period by 9.1% GC, RMS QUA by 10.0%, and RMS ES by 15.8% (Table 1). Similar reductions were also obtained for the flat shoes and 5.1-cm heel height conditions.
TA-MG Co-contraction Period, QUA Activation Period, and RMS Magnitude of Each Muscle for 6 Test Conditions
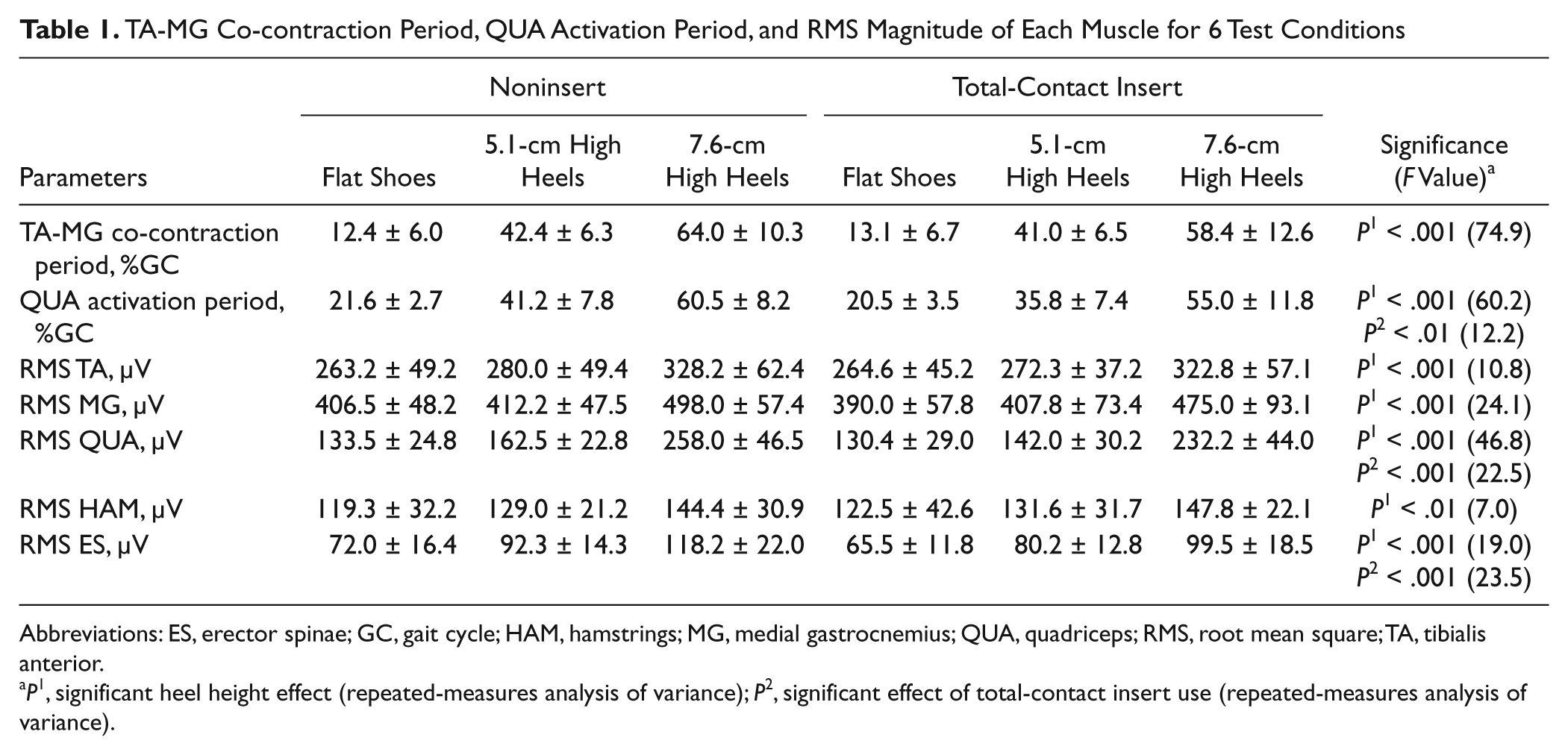
Abbreviations: ES, erector spinae; GC, gait cycle; HAM, hamstrings; MG, medial gastrocnemius; QUA, quadriceps; RMS, root mean square; TA, tibialis anterior.
P1, significant heel height effect (repeated-measures analysis of variance); P2, significant effect of total-contact insert use (repeated-measures analysis of variance).
The ANOVA results indicate that all peak EMGs at HS were increased significantly as heel height increased (F = 6.4-13.8, P < .05) (Figure 4). For instance, under the flat shoes condition, peak MG at HS was 47.5 ± 22.8 µV, and it increased to 513.6 ± 54.5 µV for the 7.6-cm heel height condition. In addition to the heel-height effect, peak MG and peak ES at HS were significantly reduced by insert use (MG, F = 17.6, P < .001; ES, F = 11.5, P < .01) (Figure 4). When compared with the noninsert conditions, use of a TCI reduced peak MG by 30.1% and peak ES by 15.0% for the flat shoes condition and reduced peak MG by 19.0% and peak ES by 21.5% for 7.6-cm heel height condition (Figure 4).
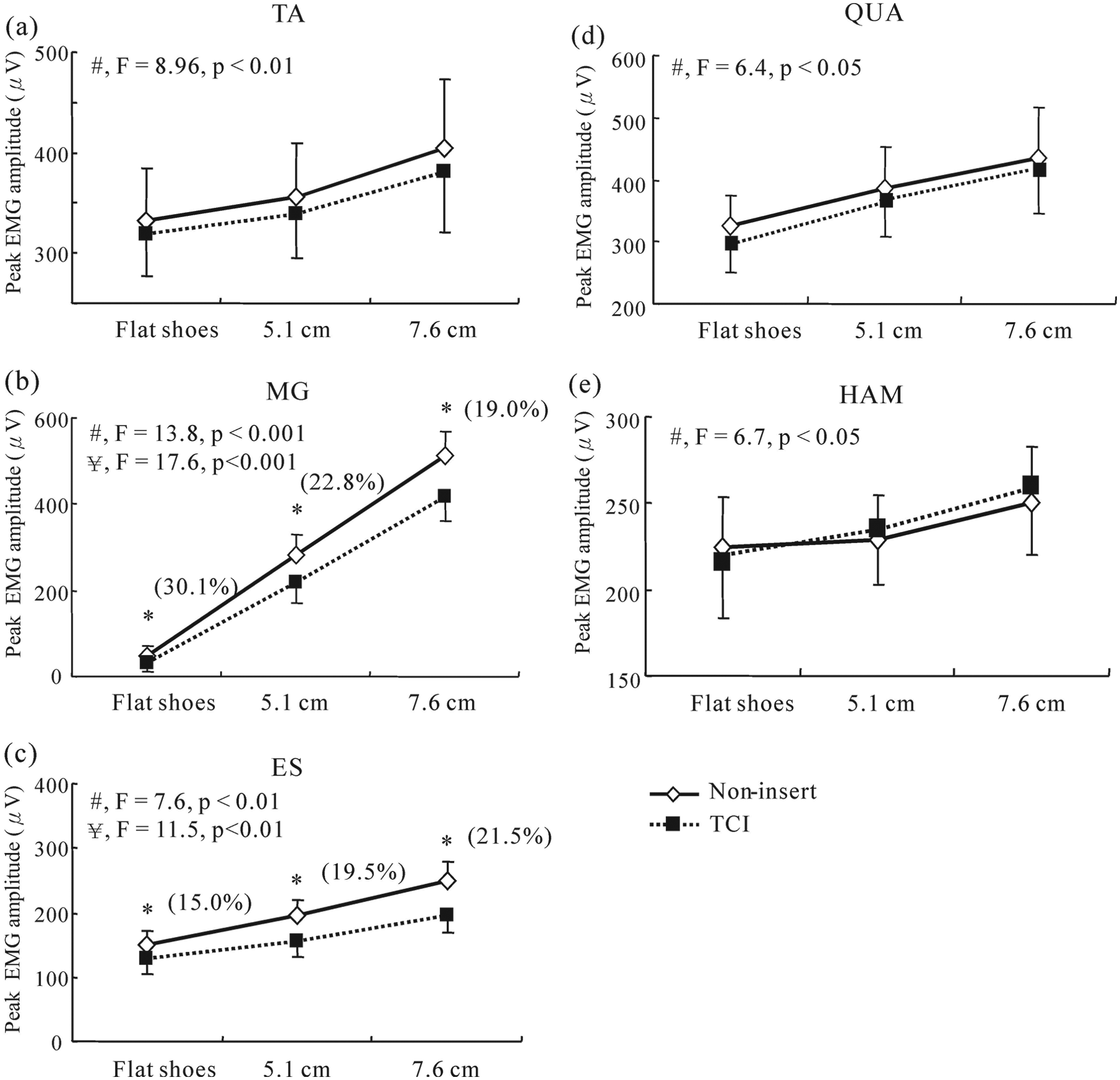
Peak electromyographic (EMG) reading of the (a) tibialis anterior (TA), (b) medial gastrocnemius (MG), (c) erector spinae (ES), (d) quadriceps (QUA), and (e) hamstrings (HAM) muscles at heel strike (HS) for different heel heights and insert conditions. The number in parentheses denotes difference between noninsert and total-contact insert (TCI) conditions: (Noninsert – TCI)/Noninsert × 100%. #Significant heel height effect (repeated-measures ANOVA). ¥Significant TCI effect (repeated-measures ANOVA). *P < .01; significant difference between noninsert and TCI use (paired t test).
Rearfoot Angles
Figure 3b shows the mean angular motions of the rearfoot for the 3 heel heights without inserts. Statistical analysis showed that increasing heel height significantly increased plantar flexion (F = 25.6, P < .001) and inversion angles at HS (F = 12.2, P < .01) and the maximal plantar flexion angle during loading response (F = 28.7, P < .001) (Table 2). Maximal dorsiflexion (F = 16.0, P < .001) and maximal eversion angles during preswing (F = 13.5, P < .01) as well as the range of dorsiflexion–plantar flexion during SP (F = 6.8, P < .05) were also significantly increased by increasing heel height (Table 2). Nevertheless, only the inversion angle at HS was significantly decreased by TCI use (F = 11.8, P < .01), and no other computed angles were significantly affected by TCI use (Table 2).
Mean Rearfoot Angle ± SD for Different Heel Heights and Insert Conditions a
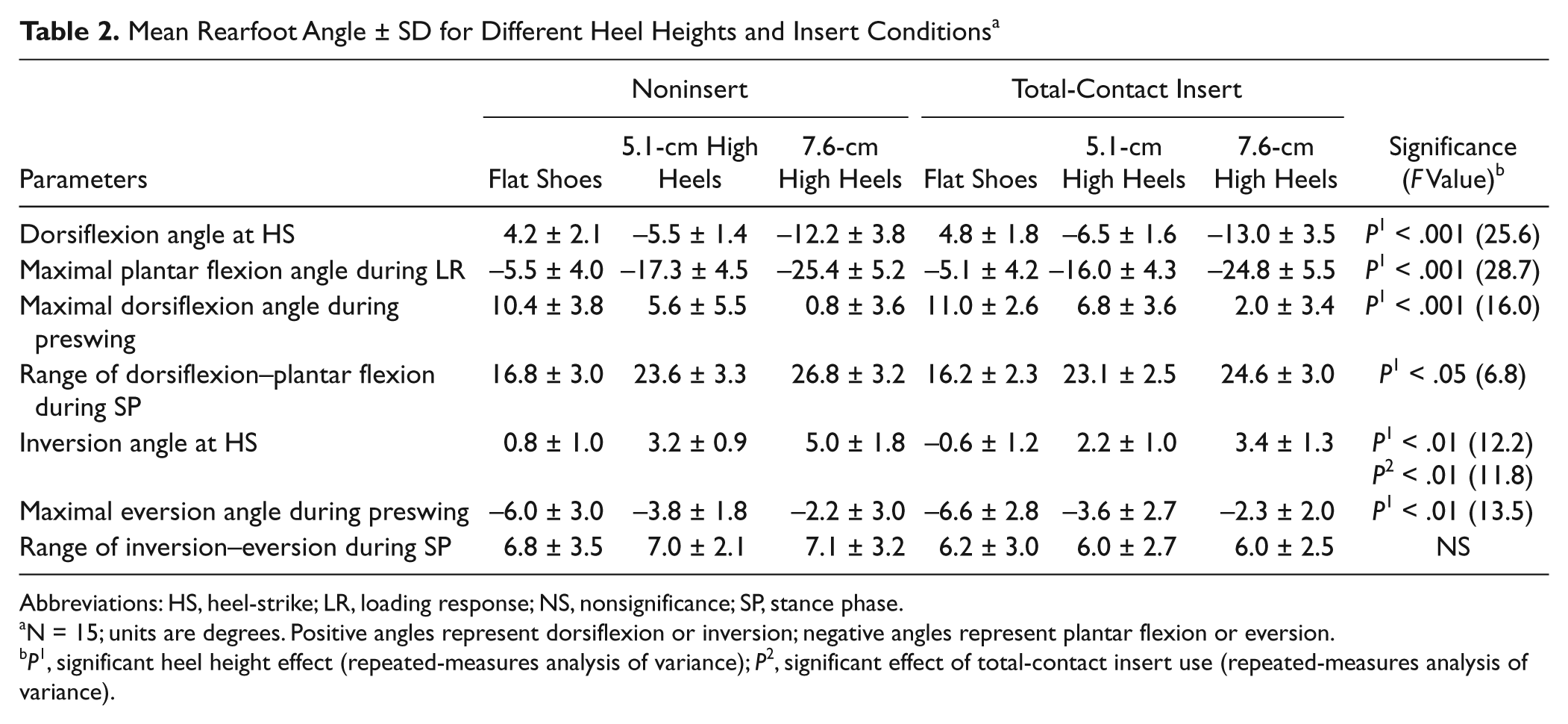
Abbreviations: HS, heel-strike; LR, loading response; NS, nonsignificance; SP, stance phase.
N = 15; units are degrees. Positive angles represent dorsiflexion or inversion; negative angles represent plantar flexion or eversion.
P1, significant heel height effect (repeated-measures analysis of variance); P2, significant effect of total-contact insert use (repeated-measures analysis of variance).
Comfort Rating
The comfort ratings statistically significantly reduced as heel height increased (F = 4.2, P = .032) (Figure 5). After installation of the TCI, the comfort ratings were significantly increased (F = 53.0, P < .001). A repeated-measures ANOVA for comfort rating indicated significant interaction effects between heel height and shoe insert (F = 182.0, P < .001). Comfort ratings were negatively correlated with RMS QUA (r = −0.591, P < .01), QUA activation period (r = −0.567, P < .01), RMS ES (r = −0.612, P < .01), and HS inversion angles (r = −0.604, P < .01).
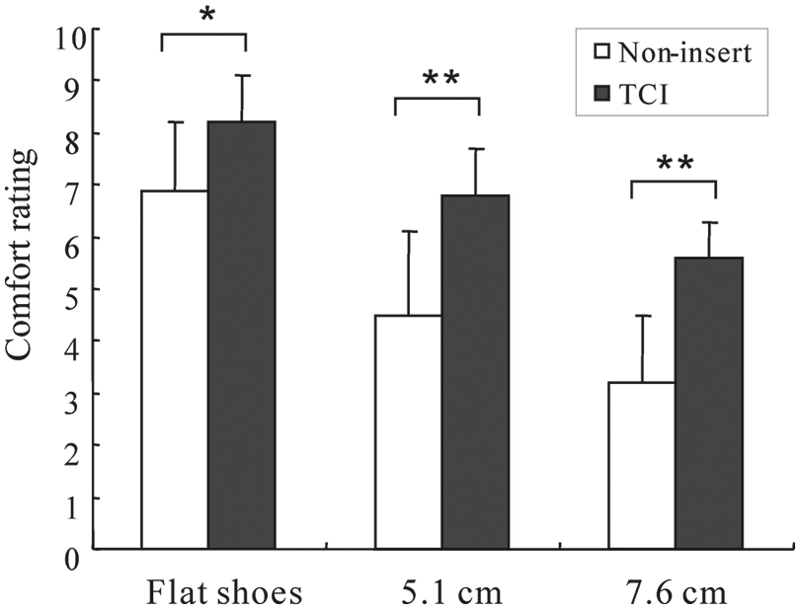
Comparison of comfort rating between shoe only and total-contact insert (TCI) in different heel heights. *P < .05; **P < .01, significant difference between noninsert and TCI conditions.
Discussion
This study indicates that increasing heel height not only increases plantar flexion and rearfoot inversion but also increases leg and low-back muscle loadings. The results are consistent with previous studies.15,19,21,36,38 Previous studies demonstrated that increased plantar flexion and inversion at heel strike likely increase risk for an inversion ankle sprain.15,36 Experimental results showed that tibialis anterior, medial gastrocnemius, and quadriceps muscles contracted more powerfully with high heels than with flat shoes while walking. Moreover, wearing high heels increases plantar flexion and inversion at heel strike and causes medial gastrocnemius activation at the end of the swing phase and the early stance phase, coinciding with antagonistic activity of the tibialis anterior muscle. Such co-contraction mechanisms of tibialis anterior and medial gastrocnemius muscles may reveal the need to stabilize the ankle joint during early stance phase. 33 Experimental results also show that quadriceps muscle activity was increased and prolonged during stance phase as heel height increased.12,19 Such increased and prolonged contraction may help maintain hip and knee stability. The observed prolonged co-contraction/contraction and increased muscle loading while wearing high heels may suggest early fatigue and, hence, limited endurance.
Use of a TCI significantly reduced peak medial gastrocnemius and the inversion angle to improve foot stability at heel strike. When compared with the 7.6-cm heel height without insert condition, the use of a TCI effectively reduced the inversion angle by 32% and peak medial gastrocnemius activity by 19.5% at heel strike. The eversion (pronation) of the rearfoot complex at heel strike is frequently regarded as a component of the shock absorption mechanism operating in the lower limbs. 32 The fabricated TCI was based on the plantar geometry of a subject’s foot, providing high conformity between the insert contact surface and foot contour. The use of a TCI may help control the position and medial–lateral extensions of a foot via its calcaneal heel-cup, thereby improving shock absorption at heel strike. 18 Lee and Hong 22 identified a relatively smaller impact force at heel strike while subjects were wearing high-heeled shoes with TCI, which resulted in a smaller impact wave traveling upward through the skeletal structures of the body, compared with that of the noninsert conditions. That use of a TCI reduced impact force at heel strike may explain the 19.5% decrease in peak medial gastrocnemius activity observed in high-heel tasks in this study.
This study also showed that the use of a TCI can significantly reduce lower limb and low-back muscle loads while walking. When compared with the 7.6-cm heel height without insert condition, use of a TCI effectively reduced peak erector spinae activity by 21.5% at heel strike, the magnitude of mean erector spinae by 15.8%, and mean quadriceps by 10% under the 7.6-cm heel height with inserts condition. Voloshin and Wosk 42 concluded that reduced shock-absorbing capacity of the human musculoskeletal system is correlated with low-back pain. Previous clinical trials demonstrated that shoe insoles or shock-absorbing heel inserts reduced low-back pain.14,18,41 When subjects wear high-heeled shoes for prolonged periods while standing or walking, reduced muscle loads by a TCI can lower the possibility of muscle fatigue and, thus, improve foot stability and reduce low-back strain. However, such a decrease in erector spinae and quadriceps muscle loads by TCI use cannot compensate for the load increase as heel height increases. Therefore, wearing flat shoes or lowering heel height may be more effective than TCIs in reducing loads on the low-back muscles.
Subjects feel less comfortable in higher heels, and the installation of a TCI can improve comfort. Interestingly, the interaction between heel heights and shoe inserts indicated that the effects of the TCI are enhanced to a greater extent in the 7.6-cm high heels than in 5.1-cm high heels or flat shoes. Such interaction might be partly due to stronger perception of discomfort for higher heels, which leads to elevated muscular loads in quadriceps and erector spinae and foot instability.
This study has several limitations. Age and experience wearing high heels may be a confounding factor in experimental conditions. Study participants were limited to young female adults inexperienced in wearing high heels. Hence, study results may not be generalizable to females of different age and experience levels. Additionally, this study was a laboratory-based experiment and tasks were performed over a 2-hour period. The positive effects of TCIs on muscle loading and foot stability while wearing high-heeled shoes may not be applicable to all wearing conditions of high-heeled shoes. In a realistic work environment, an individual may stand all day. An experiment of longer duration may further reveal individual behavioral and physical adaptations and provide a better indication of effects in actual work environments. 22 Therefore, the relationship between foot stability and muscle loading while walking in high-heeled shoes over a long period warrants further investigation.
Conclusion
Our findings indicate that wearing high-heeled shoes prolonged tibialis anterior–medial gastrocnemius co-contraction and the quadriceps muscle activation periods. Such mechanisms are adaptive strategies for maintaining foot stability. High-heeled shoes increased muscle loads on the lower extremities and low back, likely expediting muscle fatigue and thus increasing injury risk. Use of a TCI improved subjective comfort, heel-striking angle, and foot stability and reduced the loading on the quadriceps and low-back muscles. These findings suggest that wearing flat shoes or lowering heel height as much as possible is the best way to reduce injury risk. We conclude that TCIs may benefit women wearing high-heeled shoes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.