
Abstract
Background:
Open foot fractures are rare, and few surgeons see the whole spectrum of these injuries. There has been no previous study of the epidemiology and severity of open foot fractures.
Methods:
A 23-year study of the epidemiology of open fractures was undertaken in a hospital with a catchment area of about 530 000 adults. The results were used to calculate the incidences of open foot fractures and to study their epidemiology and severity.
Results:
In 23 years, 348 open foot fractures were treated. Analysis showed 3 levels of severity with the least severe fractures being isolated open forefoot fractures, which occurred in 69% of the patients. Patients with multiple forefoot fractures had a higher Injury Severity Score (ISS), prevalence of Gustilo type III fractures, and amputation rate. The most severely injured patients presented with open hindfoot and midfoot fractures. They had an average ISS of 12, and 65.9% had Gustilo type III fractures. In patients with open hindfoot fractures, the amputation rate was 17.1%. This rose to 30% in patients with open midfoot fractures. Open foot fractures tended to occur in younger patients, and only 13% were in patients aged at least 65 years.
Conclusions:
Open foot fractures are uncommon. There were 3 levels of injury. Level 1 injuries were isolated fractures of the forefoot. Level 2 injuries were multiple forefoot fractures, and level 3 injuries were open fractures of the midfoot and hindfoot. These were severe injuries with a high amputation rate. They should be treated in level 1 trauma centers.
Level of Evidence:
Level III, retrospective comparative series.
Fractures of the foot are relatively common, with a recent study showing that 12.3% of all fractures occurred in the foot. 3 They represent a wide spectrum of injury from simple phalangeal fractures to very complex midfoot and hindfoot fractures that can be difficult to treat and may result in considerable morbidity for the patient, particularly in the multiply injured patient. 14 Open foot fractures are frequently associated with a worse prognosis, but there is very little information about them in the literature. This is for two reasons: first, open fractures are rare, and second, many severe open fractures are treated in level 1 trauma centers, with less severe fractures being treated in other hospitals. As a consequence, few surgeons see the whole range of open foot fractures, and because of this, there have been no previous studies of the epidemiology and severity of all open foot fractures.
To obtain sufficient information to allow an accurate analysis of the epidemiology and severity of open foot fractures, we believe they need to be reviewed and documented over a considerable period. We have analyzed all open foot fractures over a 23-year period to investigate their epidemiology and to see which foot fractures were most severe and which were associated with other injuries. Their modes of injury were also examined.
Methods
Clinical information on all patients aged 15 years or older who presented with open fractures on an inpatient or outpatient basis to the Royal Infirmary of Edinburgh over the 23-year period between 1988 and 2010 was collected and analyzed. Clinical data up to 2005 were collected prospectively, with later data being retrieved retrospectively from the hospital’s computerized database. The Royal Infirmary of Edinburgh is the only hospital treating orthopaedic trauma in the City of Edinburgh, Midlothian, and East Lothian. It also treats patients from adjacent areas and acts as a secondary referral center for complex fractures in the southeast of Scotland. However, for the purpose of this study, all patients resident outside the City of Edinburgh, Midlothian, and East Lothian were excluded from analysis, although patients injured outside these areas but resident in our catchment area were included. To analyze the incidence of fractures over such a prolonged period, the populations aged 15 years or older in our catchment area in 1988 and 2010 15 were averaged and the average population of 532 465 used to calculate incidence.
Basic epidemiological information was collected on all patients with open fractures. This included age, sex, date of injury, type of fracture, mode of injury, extent and type of associated injuries, the Gustilo classification7,8 of the fracture, and the requirement for an amputation. The overall severity of injury was assessed using the Injury Severity Score (ISS), 1 which was derived from the Abbreviated Injury Scale (AIS) 6 of each fracture. There is some debate about the relevant AIS for open fractures as opposed to closed fractures, but in this analysis, we have used an AIS of 3 for all long-bone fractures; 2 for all hindfoot, midfoot, and metatarsal fractures; and 1 for all finger and toe phalangeal fractures. An AIS score of 1 was given for all Gustilo type I and II fractures, and a score of 2 was given for all Gustilo type III fractures. Thus, an isolated Gustilo type I open toe phalangeal fracture was given a total AIS of 2, whereas a Gustilo type IIIb open tibial fracture was given an AIS of 13. The ISS was computed by adding the squares of the 3 highest AIS scores in each patient.
Each severe musculoskeletal injury was analyzed to provide a musculoskeletal index (MSI). All fractures and severe soft tissue injuries, such as ligamentous disruptions, dislocations, nerve damage, vascular damage, and tendon injuries, were given a score of 1 and the total used to provide an assessment of the degree of musculoskeletal injury. Minor joint sprains and soft tissue injuries were excluded from analysis.
Mode of injury was divided into falls from a standing height; falls from a height (greater than 6 feet); motor vehicle accidents (MVAs); crush injuries; cutting injuries, such as those associated with lawnmowers, saws, and grinders; direct blows or assaults; and sports injuries. Two open foot fractures from a train crash were included with the MVA-related fractures. The prevalence of amputations throughout the patients’ treatment was determined. The amputations were usually undertaken because of the severity of the initial injury, the presence of other severe injuries in the leg or foot, or late complications. The type of amputation is stated in the text as clearly toe amputations were much less disabling than other foot or leg amputations. Sex ratios are presented as a male/female percentage.
Results
During the 23 years of the study, 348 open foot fractures were treated, giving an incidence of 2.84/105/y. The fractures occurred in 283 individuals with 241 patients presenting with a single open fracture, 29 with 2 open fractures, 6 with 3 fractures, 5 with 4 fractures, 1 with 5 fractures, and 1 with 6 fractures. The epidemiological details of all 348 fractures together with those of each fracture type are shown in Table 1. The average age of the patients who presented with multiple foot fractures was 41.7 (range, 15-92) years, the sex ratio was 72/28, and 10.3% were at least 65 years of age.
Epidemiological Data of Open Foot Fractures
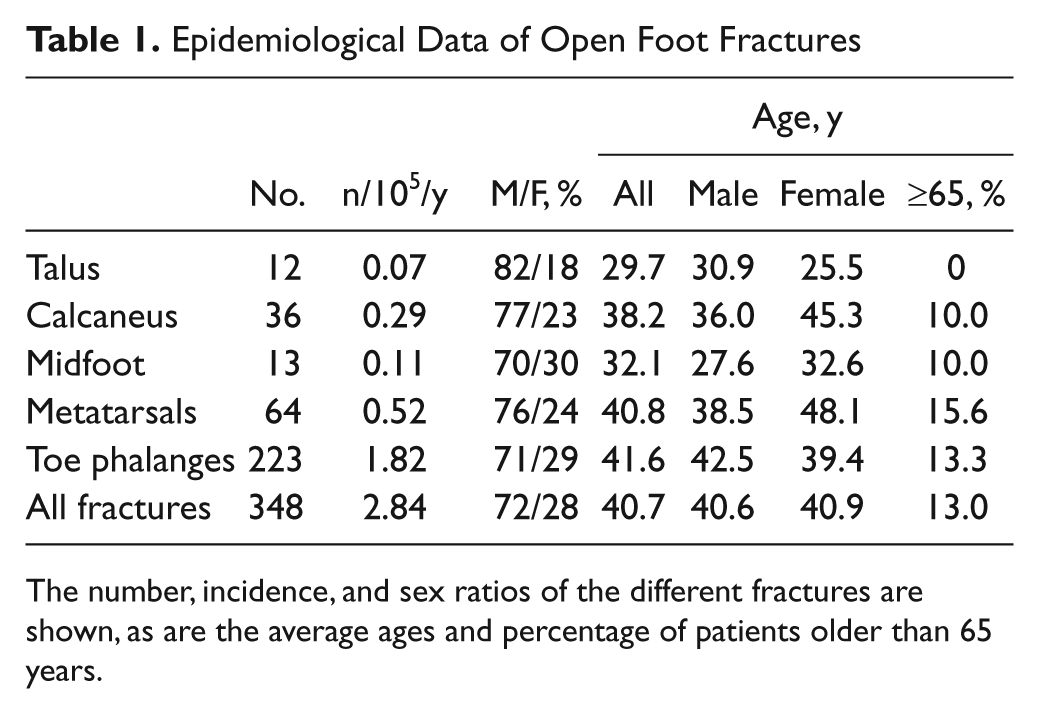
The number, incidence, and sex ratios of the different fractures are shown, as are the average ages and percentage of patients older than 65 years.
The severity of the different foot fractures is detailed in Table 2, which shows the average ISS, the percentage of patients who presented with an ISS 16 or more, and the average MSI. The percentage of Gustilo type III fractures and the amputation rate are also shown. Table 3 shows the demographic characteristics and the severity of injury associated with each mode of injury.
Severity of the Different Open Foot Fractures
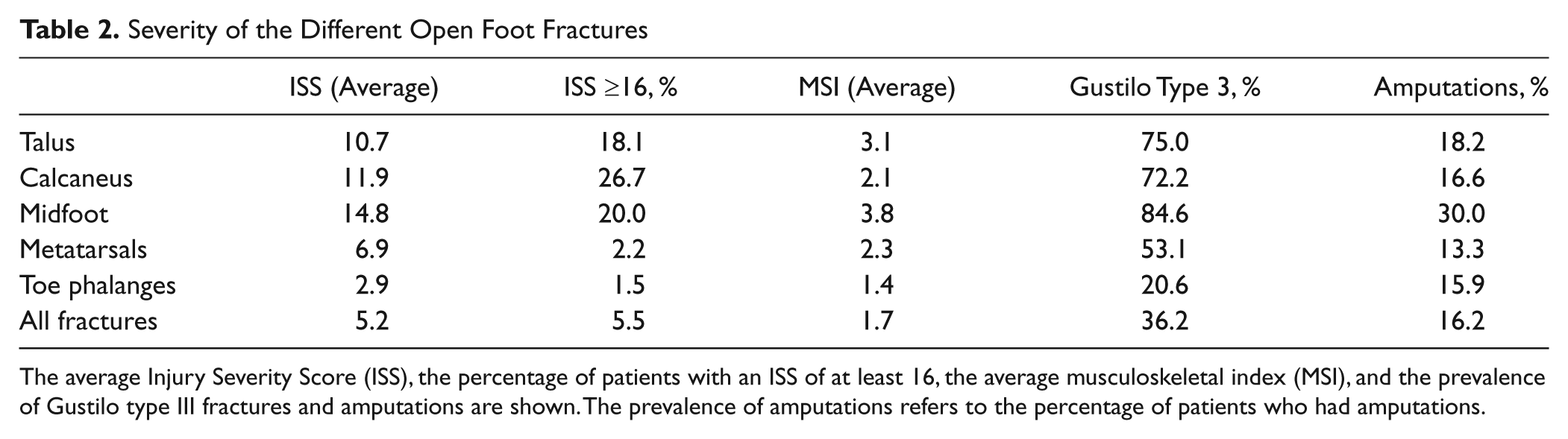
The average Injury Severity Score (ISS), the percentage of patients with an ISS of at least 16, the average musculoskeletal index (MSI), and the prevalence of Gustilo type III fractures and amputations are shown. The prevalence of amputations refers to the percentage of patients who had amputations.
Severity of Injury Associated With the Different Modes of Injury
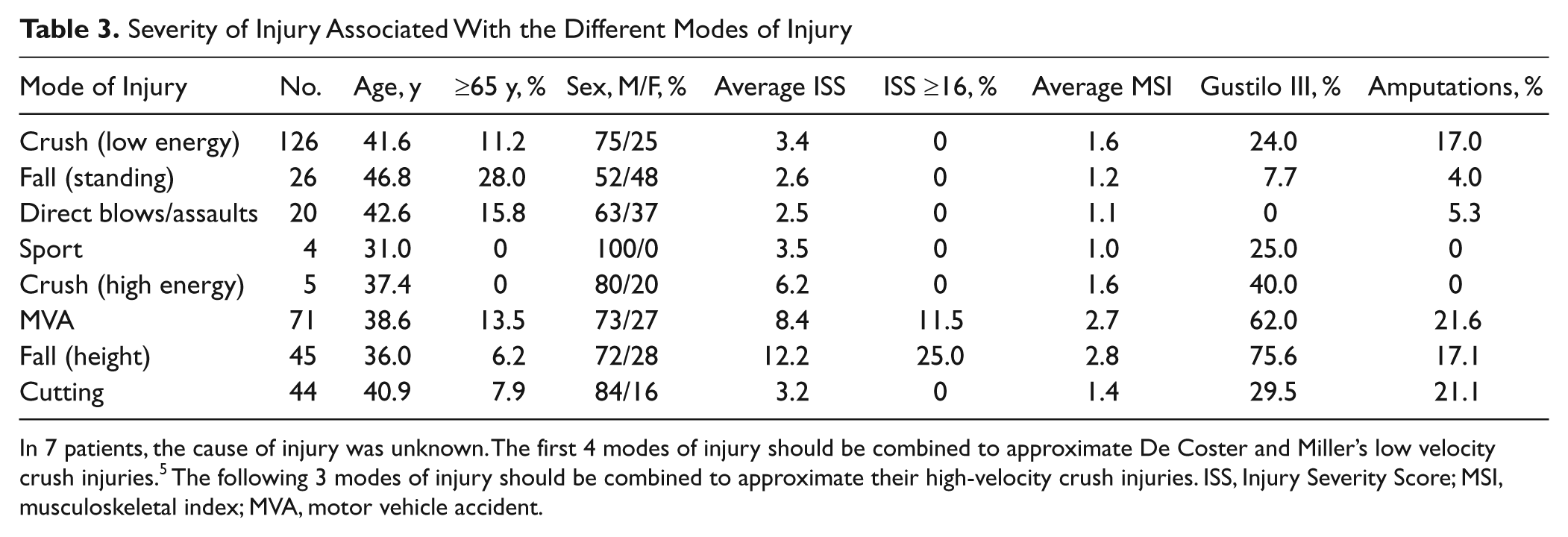
In 7 patients, the cause of injury was unknown. The first 4 modes of injury should be combined to approximate De Coster and Miller’s low velocity crush injuries. 5 The following 3 modes of injury should be combined to approximate their high-velocity crush injuries. ISS, Injury Severity Score; MSI, musculoskeletal index; MVA, motor vehicle accident.
Talar Fractures
Eleven of the 12 open talar fractures were unilateral, with 1 patient presenting with bilateral open calcaneal and talar fractures. Five (45.5%) of the patients were injured in MVAs and 5 (45.5%) in falls from a height. The remaining patient fell from a horse. The average ISS, the percentage of patients who had an ISS of 16 or more, and the sex ratio are listed in Table 2. Five (45.5%) patients presented with other musculoskeletal injuries, of whom 4 (80%) had other open or closed fractures of the foot and ankle. There were 2 amputations; one was a below-knee amputation and the second a forefoot amputation, which was undertaken because of a severe associated forefoot injury.
Calcaneal Fractures
All of the open calcaneal fractures were caused by a fall from a height, an MVA, or a high-energy crush injury. The most common cause was a fall from a height, which resulted in 66.6% of the open fractures. This group presented with an average ISS of 12.3, and 33.3% had an ISS of 16 or more. A further 19.4% of the fractures were caused by an MVA. The average ISS of these patients was 13.6, and 40.0% had an ISS of at least 16. The remaining 13.9% of the fractures were caused by crush injuries. These patients were less severely injured, with an average ISS of 6.2, the highest ISS being 8.
Six (20.0%) patients presented with bilateral open fractures. All these fractures were Gustilo type IIIb in severity. The average ISS of patients with open calcaneal fractures was 14.2, and 50.0% had an ISS of 16 or more. Further analysis showed that 58.3% of patients with open calcaneal fractures had other musculoskeletal injuries, 13.9% of patients had a spinal fracture, and 50.0% had other open or closed foot or ankle fractures. Five patients had a below-knee amputation.
Midfoot Fractures
The 13 midfoot fractures occurred in 10 patients, with 1 patient presenting with multiple midfoot fractures and 1 presenting with bilateral Gustilo type IIIc fractures. Two patients were injured in a fall from a height and 7 in an MVA. The remaining patient had a crush injury. The average ISS was 14.8, and 20.0% of the patients had an ISS of at least 16. Nine patients presented with other musculoskeletal injuries, with 6 patients having other fractures of the distal tibia, ankle, and foot. Two patients presented with Gustilo type IIIc open tibial diaphyseal fractures. Three patients (30.0%) were treated by amputation. One patient had midfoot amputation and a contralateral below-knee amputation, 1 had an above-knee amputation because of severe associated injures, and 1 had a forefoot amputation.
Metatarsal Fractures
Of the 64 open metatarsal fractures, 28 (43.8%) were single fractures. The average age of this group was 41.2 years, and the sex ratio was 72/28. The average ISS was 5.6, and the highest ISS was 8. Only 17.9% had other musculoskeletal fractures, of which 80% were foot injuries. The most common cause of a single open metatarsal fracture was a crush injury (46.4%), with 21.4% resulting from MVAs. Only 21.4% of the fractures were Gustilo type III fractures, and 10.7% had an amputation.
The remaining 36 fractures were multiple open metatarsal fractures with patients presenting with 2 to 5 fractures. The average age of this group was 40.2 years, and the sex ratio was 82/18. The average ISS was 8.9, 5.9% had an ISS of 16 or more, and 52.9% had other musculoskeletal injuries apart from multiple open metatarsal fractures. As with single metatarsal fractures, the most common causes of fracture were crush injuries and MVAs, but with multiple open metatarsal fractures, 52.9% were caused by MVAs and 29.4% by crush injuries. Analysis of fracture severity showed that 77.8% were Gustilo type III fractures, and 27.8% of the fractures were treated by amputation. All amputations were forefoot amputations.
Toe Phalangeal Fractures
Of the 223 open toe phalangeal fractures, 171 were single fractures. The average age of this group was 41.7 years, and the sex ratio was 72/28. The average ISS was 2.4, the highest ISS was 9, and 8.8% had other musculoskeletal injuries, with 80% of these being foot injuries. The majority (46.8%) of single phalangeal fractures were caused by crush injuries, with 16.4% being caused by cutting injuries and 12.3% by standing falls. Only 7.6% were caused by MVAs and 2.9% by falls from a height. Analysis of fracture severity showed that 10.5% were Gustilo type III fractures, and 12.9% had an amputation.
The remaining 52 open phalangeal fractures were multiple fractures with patients presenting with 2 to 5 fractures. The average age of this group was 40.1 years, and the sex ratio was 63/37. The average ISS was 6.4, 12.5% of patients had an ISS of 16 or more, and 20.8% had other musculoskeletal injuries. Analysis of the mode of injury showed that 83.3% were caused by crush injuries, MVAs, or cutting injuries (33.3%, 29.2%, and 20.8%, respectively). Analysis of the fracture severity showed that 53.8% were Gustilo type III fractures and 23.1% were Gustilo type IIIc fractures. Overall, 37.5% of the patients with multiple open phalangeal fractures had an amputation. All amputations for single or multiple toe fractures were toe amputations. No amputations were undertaken because of associated injuries.
Open Fractures in the Elderly
Analysis of the patients who were 65 years or older showed that there were 41 fractures comprising 11.8% of the open fractures. The sex ratio was 76/24, and the average ISS was 4.4, with 5.4% having an ISS of at least 16. A review of the fracture types shows that 9.8% were calcaneal fractures, 2.4% were midfoot fractures, 19.5% were metatarsal fractures, and 68.3% were toe phalangeal fractures. There were no talar fractures. Four (10.8%) of the patients had multiple fractures, with 1 patient presenting with bilateral calcaneal fractures, 1 with 2 metacarpal fractures, and 2 with 2 phalangeal fractures. The 2 most common modes of injury were MVAs (24.4%) and crush injuries (19.5%). A review of the MVA-related fractures shows that 71.4% occurred in pedestrians and were probably crush injuries. Only 26.8% of the fractures were Gustilo type III, and 17.1% of the open fractures were treated by amputation, with 71.4% of the amputations being for open phalangeal fractures.
Discussion
It might be considered surprising that there has been no previous analysis of the epidemiology and severity of open foot fractures. However, open foot fractures are not common, and few hospitals will treat the complete spectrum of these injuries. Analysis of our data showed that 69% of open foot fractures were isolated fractures of the forefoot involving the metatarsus or phalanges. These fractures will often be treated in community hospitals. The remaining 31% of the fractures were either multiple forefoot fractures or open fractures of the midfoot or hindfoot. These are more serious injuries and are often treated in specialist trauma units. It is therefore difficult for many surgeons to analyze all open foot fractures. All foot fractures in our catchment area are reviewed in one emergency department and admitted to one hospital. Our data are accurate, but we accept that it is sometimes difficult to decide if an isolated fracture of a distal phalanx of a toe is open. We review all fractures in which there is clinical suspicion of the fracture being open, but we accept that no system is perfect, and some minor open injuries may not have been reviewed.
De Coster and Miller 5 listed 5 categories of traumatic foot trauma: low-velocity blunt trauma such as a crush injury, high-velocity blunt trauma such as MVAs, low-velocity penetrating trauma such as nail penetration wounds, high-velocity penetration wounds such as lawnmower wounds, and thermal injury wounds. The last category does not cause fractures, but analysis of our data according to De Coster and Miller’s criteria 5 (Table 3) shows that 181 (50.6%) of the open fractures in our series resulted from low-velocity crush injuries, 121 (34.8%) followed high-velocity crush injuries, 24 (6.9%) were caused by low-velocity penetrating trauma, and 20 (5.7%) followed lawnmower injuries. In 7 (2.0%), the cause of injury was unknown. De Coster and Miller’s study was undertaken in the United States, but we believe that the social infrastructure of the 2 countries is similar, and our results will be relevant in many countries. The one proviso is that there are no gunshot wounds in our series. These occur more commonly in other countries, but it is difficult to accurately estimate their incidence. In a recent study from a major level 1 trauma center in the United States, only 3.3% of the open gunshot fractures occurred in the foot. 4
We have categorized our fractures differently from De Coster and Miller. 5 Our results show that there are 3 levels of severity of open foot fractures. Level 1 injuries are isolated open forefoot fractures. Analysis of patients who presented with this level of injury showed that they had an average ISS of 3.7 and that 1.7% of the patients had an ISS of at least 16. The average MSI was 1.6, the prevalence of Gustilo type III fractures was 19.2%, and 15.4% of the patients had an amputation at some point during their treatment.
Level 2 injuries occurred in those patients who sustained multiple open fractures of the forefoot. These patients were more severely injured. The average ISS of this group was 7.1, 7.5% had an ISS of 16 or more, and the average MSI was 3.2. The associated soft tissue injuries were also more severe, with 52.5% having Gustilo type III fractures and 30% having an amputation.
The most severely injured group of patients, those with level 3 injuries, were the patients who presented with open fractures of the midfoot or hindfoot. Table 2 indicates the severity of open fractures of the talus, calcaneus, and midfoot, but overall the ISS was 12.0, 22.4% of the patients had an ISS of at least 16, and the average MSI was 2.5. The prevalence of Gustilo type III fractures was 69.5%, but only 16.3% of the patients had an amputation, although Table 2 shows that the amputation rate in patients with midfoot fractures was 30%. The high amputation rate for open midfoot fractures emphasizes the severity of these fractures in addition to the problems of coexisting forefoot soft tissue damage and other severe leg fractures. It also reflects the difficulty of covering midfoot and forefoot injuries with flaps.
A review of the literature shows that our amputation rate is consistent. There is very little information about open midfoot injuries, but Marsh et al 11 documented 18 open talar fractures and fracture dislocations over a 23-year period. They stated that 77.7% of their injuries were Gustilo type III in severity. They did not undertake any amputations but reported poor results with a high infection rate, and they suggested that primary talar body excision should be considered in cases where the talar body had been extruded.
There is more information available about open calcaneal fractures. The rates of amputation vary; a Canadian study 2 reported a 6.7% rate over a 10-year period, but 2 studies9,13 from trauma units in the United States reported a 14% amputation rate. Hoxie et al, 10 who treated 10 open metatarsal fractures in an 11-year period, documented the amputation rate for open metatarsal fractures. They reported a 20% amputation rate for single open metatarsal fractures and a 60% rate for multiple open metatarsal fractures. These studies confirm the rarity of these fractures and the considerable morbidity associated with them.
Table 2 suggests that open midfoot fractures are the most severe open fractures that surgeons will have to treat. They are associated with the highest ISS and MSI, although their proximity to the metatarsals means that one might expect a higher MSI than with calcaneal or talar fractures. However, 84.6% of the fractures were Gustilo type III in severity. Calcaneal fractures were associated with a higher ISS than talar fractures, but patients with talar fractures had a higher prevalence of other open fractures and a higher MSI. Our results suggest that open talar and calcaneal fractures are similar in severity. The severity of these fractures is highlighted by comparing them with other open lower limb fractures, from the same catchment area, in the 23-year study period. The comparative results for these fractures are shown in Table 4. This shows that patients who are admitted with open femoral diaphyseal fractures and distal femoral fractures will usually be the most severely injured, but patients who present with open midfoot and forefoot fractures are, if anything, more seriously injured than those who present with open tibial diaphyseal fractures and proximal tibial fractures. Patients with open distal tibial and ankle fractures are, on average, less severely injured. However, a comparison of Tables 2 and 4 shows that open hindfoot and midfoot fractures have a higher prevalence of Gustilo type III soft tissue injuries than other open lower limb fractures.
Severity of Different Open Fractures in the Lower Limb
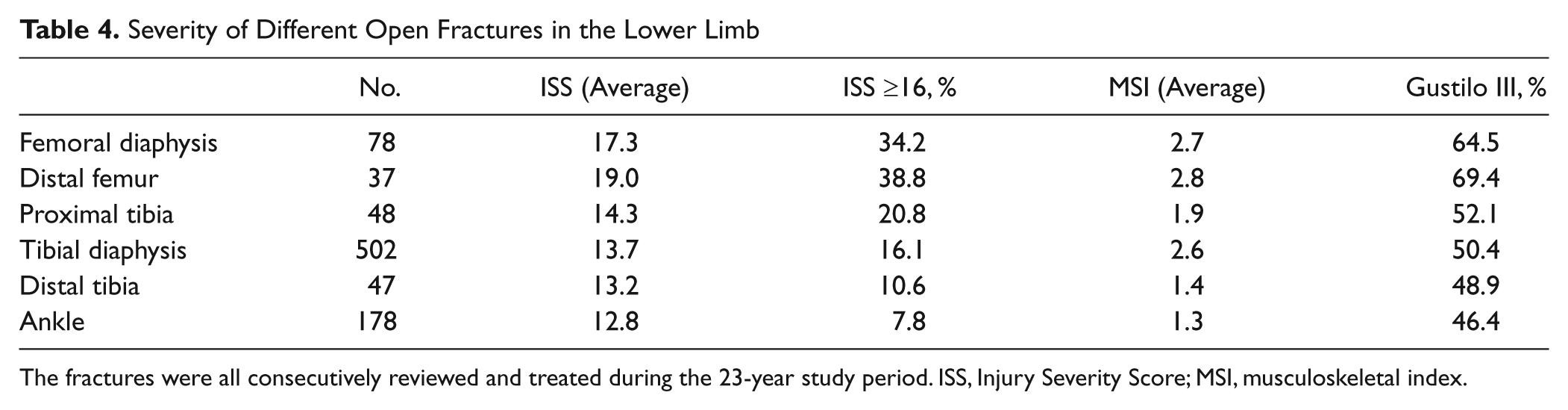
The fractures were all consecutively reviewed and treated during the 23-year study period. ISS, Injury Severity Score; MSI, musculoskeletal index.
A review of the modes of injury (Table 3) shows that low-energy crush injuries caused 36.2% of all open foot fractures. All were metatarsal and phalangeal fractures. Cutting injuries were responsible for 12.6% of the fractures. This included 1 midfoot fracture, but the rest of the cutting injuries affected the forefoot. There were 20 lawnmower injuries during the study period. These injuries have received considerable attention in the past 15 years, and a study from the United States 4 has shown that 32.4% of hospitalizations following lawnmower injures resulted in toe amputations. In our series, the 20 fractures occurred in 15 patients with an average age of 42.3 years and a sex ratio of 80/20. All patients had open toe fractures, 35% were Gustilo type IIIb in severity, and 20% of the patients had amputations.
Injuries to the midfoot and hindfoot are usually high-energy injuries, and 83.4% of these fractures followed an MVA or a fall from a height. A further 5 (8.2%) resulted from a high-energy crush injury with a heavy object falling on the foot from a height. Table 3 shows that the patients who presented with open foot fractures following a fall from a height were more seriously injured than those involved in an MVA. Richter et al 12 analyzed foot fractures in restrained front seat car occupants and noted that foot fractures were mainly caused by foot compartment deformation in head-on collisions. However, in our study, 42.1% of the open foot fractures due to MVAs occurred in pedestrians.
In recent years, there has been increasing interest in fractures in the elderly. However, none of the foot fractures are osteoporotic fractures, and this probably accounts for the fact that only 13% of the open foot fractures occurred in patients aged 65 years or older. A study of all fractures in our catchment area in 2007-2008 showed that overall, 35.9% of fractures occurred in this age group, but Tables 1 and 3 show that the average ages of patients who present with the different open foot fractures are relatively low. Only 7 (18.9%) of the 65-year or older group were injured as a result of a standing fall, and 6 presented with single open forefoot fractures, with 1 patient presenting with 2 open toe fractures. There were 5 open midfoot and calcaneal fractures in 4 patients. All were caused by an MVA or a fall from a height. The average ISS was 12.0, 25% had an ISS of at least 16, 75% were Gustilo type III fractures, and 50% of the patients had an amputation. As one would expect, high-energy open fractures in older patients are associated with a considerable morbidity.
In conclusion, our results show that open fractures of the foot are significant injuries. There are 3 levels of injury. However, even level 1 single open forefoot fractures have a high amputation rate, which increases in level 2 injuries when there are multiple open forefoot fractures. Level 3 injuries, these being open fractures of the midfoot and hindfoot, are rare but, when they occur, are associated with a high prevalence of other injuries and severe soft tissue injuries, which may lead to amputation. We believe that level 3 injuries should be treated in specialist trauma units.
Footnotes
Ethical Approval
The ethical committee of the parent institution regards this study as audit, and ethical approval is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.