
Abstract
Background:
Osteochondral autologous transplantation (OAT) has been performed for years for osteochondritis dissecans of the knee with good clinical results. In osteochondritis dissecans of the talus, however, OAT represents a challenge to the orthopaedic surgeon as frequently malleolar osteotomy has to be performed for exposure of the talus and the harvesting of the osteochondral graft usually requires an arthrotomy of the knee.
Methods:
In this study, we evaluated the clinical outcome of OAT in 32 patients (mean follow-up 29 months) by means of the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Scale, ankle pain on the visual analogue scale (VAS), HSS Patella Score, and magnetic resonance imaging (MRI) of the osteochondral graft.
Results:
Median AOFAS score was 86, median ankle pain on VAS was 2.0, and median HSS Patella score was 95. Complications included 1 case of delayed wound healing and 1 case of nonunion of the malleolar osteotomy requiring revision surgery. MRI findings were abnormal in 14 out of 28 cases; however, with the numbers available in our study no correlation to clinical outcome could be detected.
Conclusion:
OAT in osteochondritis dissecans of the talus was a safe procedure with good clinical results. As abnormal MRI finding was not necessarily diagnostically conclusive, MRI might be of limited value in postoperative follow-up.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Osteochondritis dissecans is characterized by avascular necrosis, which is at first confined to the subchondral bone (stage I-II according to the International Cartilage Repair Society 5 ) but may result in discontinuity of the adjacent articular cartilage (stage III) or dislocation of the entire osteochondral fragment (stage IV). As previous operative techniques—for example, fixation of the osteochondral fragment,2,21 excision of the osteochondral fragment with or without drilling, or cancellous bone grafting6,8—are only successful in 73% to 86% of patients with osteochondritis dissecans stage III or IV, 26 autologous osteochondral transplantation has been increasingly used to reconstruct the articular surface. In osteochondritis dissecans of the knee, autologous osteochondral transplantation has yielded good clinical results7,14,18 even though no one technique among the various treatment options has as yet reached the status of “gold standard.” Autologous osteochondral transplantation of the talus represents a challenge to the orthopaedic surgeon, as (1) tibial wedge or malleolar osteotomy has to be considered in most cases to gain perpendicular access to the talus and (2) the osteochondral graft has to be harvested usually from the lateral femoral condyle of the knee, thus requiring an additional arthrotomy.1,4,11-13,16,17,23-25 Most studies investigating clinical results after osteochondral autologous transplantation describe small groups with osteochondral lesions of varying origin.
In this study, however, we included exclusively patients with osteochondral lesions due to osteochondritis dissecans of the talus. We evaluated clinical results of both donor and recipient site after osteochondral autologous transplantation (OAT) with the lateral femoral condyle as the donor site. We performed magnetic resonance imaging (MRI) of the osteochondral graft and looked for any correlation between abnormal MRI findings and clinical results.
Methods
Patients
For this study we reviewed 36 patients who had undergone osteochondral autologous transplantation for osteochondritis dissecans of the talus between March 2005 and March 2009. This particular interval was chosen because all operative procedures were performed by or under the direct supervision of one surgeon, thus allowing for more homogenous conditions. Four patients were lost to follow-up. Characteristics of the remaining 32 patients are shown in Table 1. In all cases we performed magnetic resonance imaging for preoperative planning and to rule out osteochondral lesions of traumatic origin. Ankle pain had been present for more than 6 months in all patients.
Characteristics of Patients Included (n = 32)
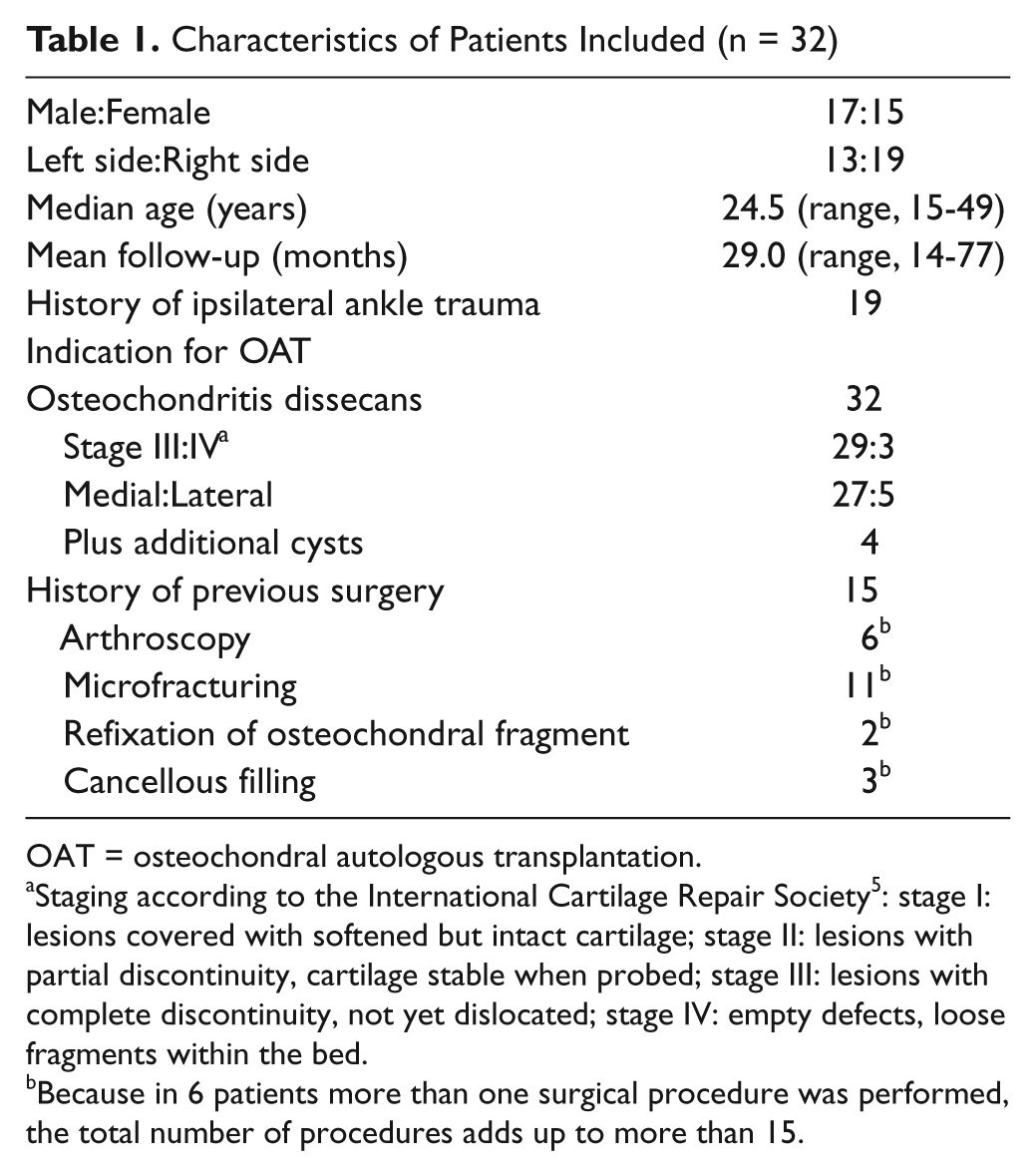
OAT = osteochondral autologous transplantation.
Staging according to the International Cartilage Repair Society 5 : stage I: lesions covered with softened but intact cartilage; stage II: lesions with partial discontinuity, cartilage stable when probed; stage III: lesions with complete discontinuity, not yet dislocated; stage IV: empty defects, loose fragments within the bed.
Because in 6 patients more than one surgical procedure was performed, the total number of procedures adds up to more than 15.
Operative technique
Operative exposure was achieved as follows according to the location of the osteochondral lesion (see Figure 1): For a centro- or posteromedial location, a medial malleolar osteotomy was performed (n = 25) and in the case of centro- or posterolateral location a lateral malleolar osteotomy (n = 1) was performed. Image intensifiers were used in all of these procedures. If the osteochondral lesion was located anteromedially (n = 2) or anterolaterally (n = 4), an anteromedial or anterolateral arthrotomy was sufficient for adequate exposure. For autologous osteochondral transplantation the press fit Osteochondral Autologous Transfer System (OATS, Arthrex, Naples, FL) was used. According to the size of the osteochondral lesion, 1 (n = 20), 2 (n = 9), or 3 (n = 3) cylindrical grafts sized 6 mm (n = 10), 8 mm (n = 36), or 10 mm (n = 1) were harvested at the ipsilateral lateral femoral condyle adjacent to the trochlear groove just proximal to the sulcus terminalis (Figure 2) and inserted into the recipient site. Afterwards, internal fixation of the medial malleolus was achieved by means of 1 cancellous screw and 1 Kirschner wire for rotational stability. Internal fixation of the lateral malleolus was obtained by q lag screw and plate osteosynthesis. No additional surgical procedures were performed in any of the patients.
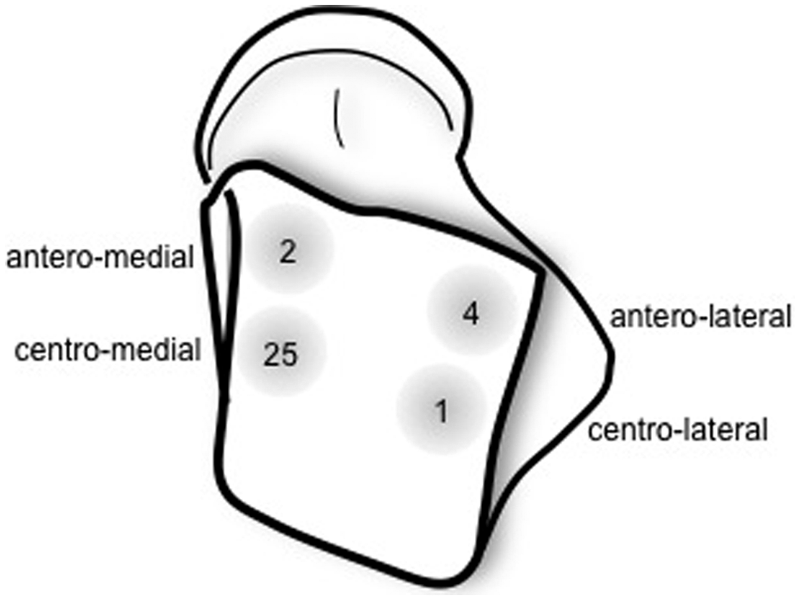
Location of osteochondral lesions of the talus.

Intraoperative photograph of the optimal harvest site located on the lateral femoral condyle adjacent to the trochlear groove just proximal to the sulcus terminalis.
Postoperatively, partial weightbearing (20 kg) was allowed for 6 weeks. After 6 weeks postoperatively, progression of weightbearing was allowed. If applicable, hardware was removed 6 to 12 months later depending on osseous healing seen on radiographs. Due to slight persistent ankle pain, diagnostic arthroscopy of the ankle joint was conducted in 4 cases simultaneously with and in 1 case independent of hardware removal.
Data gathering
The patients were seen 14 to 77 months (mean 29 months) after surgery for follow-up. After informed consent was obtained, they were asked to rate their ankle pain on a visual analogue scale (VAS). Any complications arising during the postoperative course were noted. Ankle pain and donor site morbidity were evaluated by questionnaires (American Orthopaedic Foot and Ankle Society [AOFAS] Ankle-Hindfoot Scale score for ankle pain, maximum 100 points; Hospital for Special Surgery [HSS] Patella Score for anterior knee pain, maximum 100 points; see Table 2). These scores were chosen because they combined both subjective and objective features to describe the patients’ functional level. On physical examination, range of motion, crepitation, joint effusion, scar tissue, and tenderness on palpation of both ankle and knee joint were noted.
Hospital for Special Surgery Patella Score (0-100 points) From Baldini et al 3
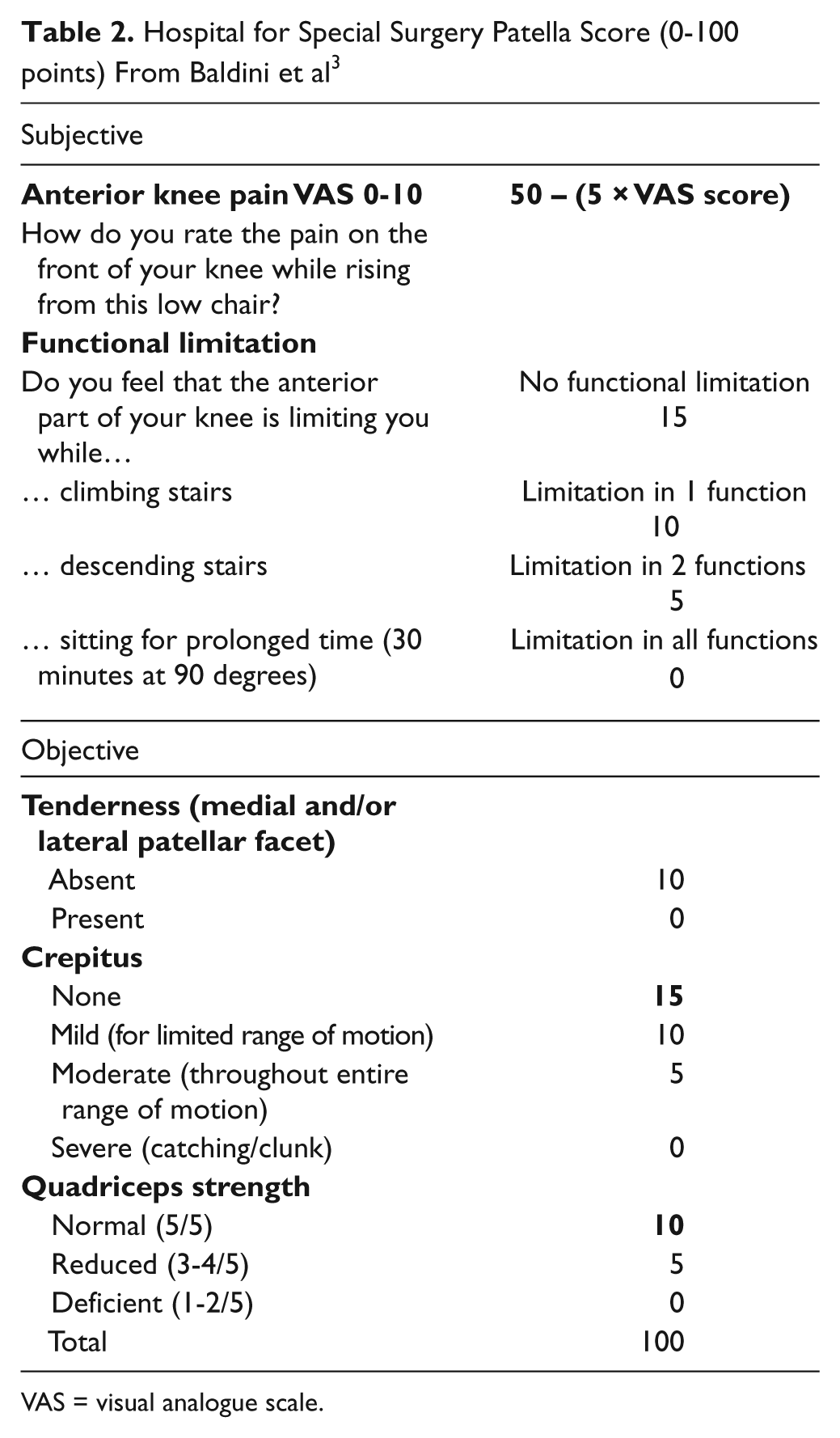
VAS = visual analogue scale.
MRI of the ankle was performed in all but 4 patients, who refused further radiologic imaging. MRI studies were performed using a Siemens symphony 1.5 Tesla scanner. The sequences that were used for rating were as follows: Sagittal and coronal PD_tse-fat saturated; FOV 220*220 thickness 4 mm; coronal T2w-3D DESS; FOV 220*220 thickness 1.5 mm. Radiologic assessment was performed by a radiologist blinded to the clinical results of the patients. The study design was approved by the university ethical committee.
For statistical analysis the Statistical Package for Social Sciences (SPSS® Inc., IBM, version 19) was used. Continuous normally distributed variables were summarized as mean including minimal and maximal range, continuous non-normally distributed variables as median including minimal and maximal range. Percentages were rounded off to the first decimal. When comparing results of clinical scores between 2 groups, 2-tailed unpaired Student t-test was used for normally distributed score values, and Mann-Whitney U test was used for non-normally distributed score values. Shapiro-Wilk test was used to test for normality. A probability value of less than 0.05 was considered to indicate statistical significance.
Results
Median ankle pain on the VAS was 2.0 (range, 0-5.5), median postoperative score results were 95 for the HSS Patella Score (range, 35-100) and 86 for the AOFAS score (range, 68-100). In all 5 cases of diagnostic arthroscopy of the ankle joint, good integration of the osteochondral graft with good alignment of the articular surface was seen (Figure 3A).
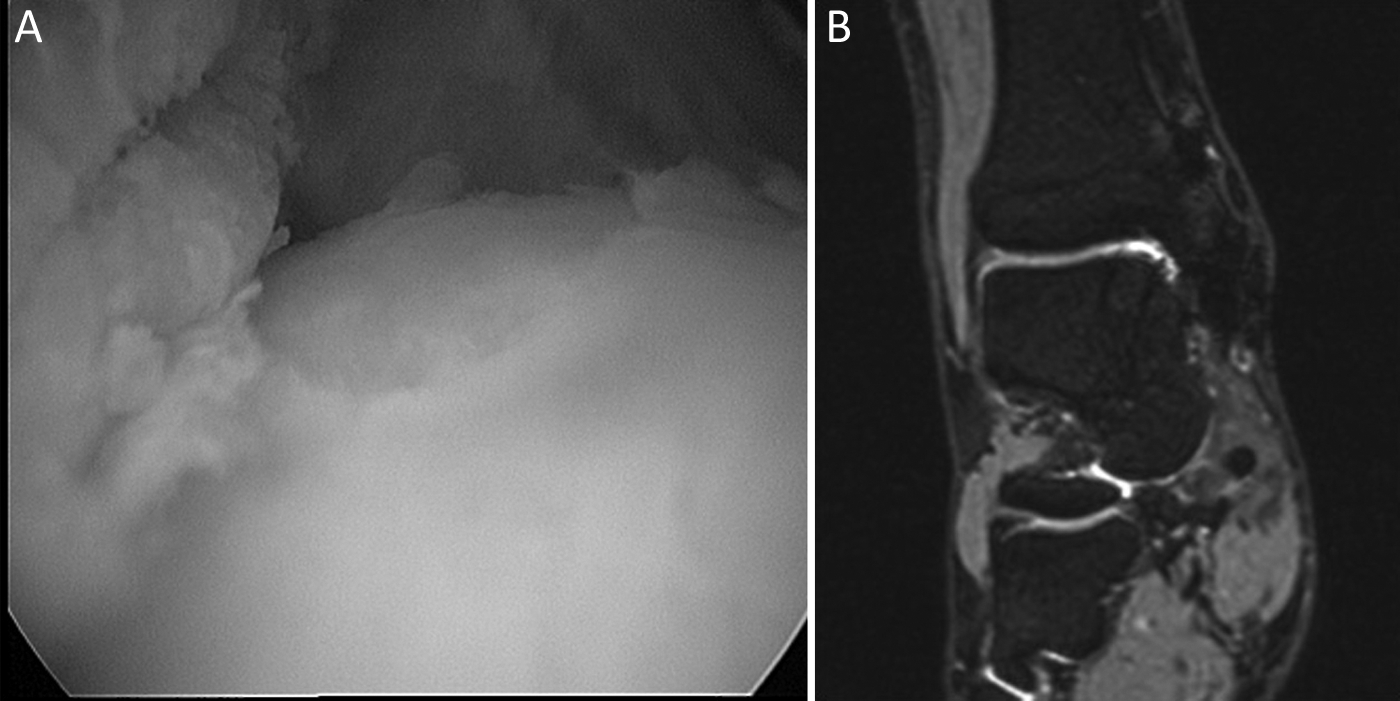
Arthroscopic view of the talus of a 20-year-old male patient 9 months after osteochondral autologous transplantation (Figure 3A). Magnetic resonance imaging of the osteochondral graft was conducted 18 months after surgery (Figure 3B), the patient scored 97 points on the American Orthopaedic Foot and Ankle Society (AOFAS) scale at that time.
There were 2 complications: In 1 patient, there was protracted wound healing, which required no further operative intervention. In another patient, a heavy smoker, revision surgery with reosteosynthesis and apposition of autologous cancellous bone had to be performed 16 months after OAT for nonunion of the medial malleolus. Even though complete consolidation of the medial malleolus occurred after revision surgery, the patient continued to complain of persistent ankle pain. Twenty-seven months after OAT the patient scored 68 points on the AOFAS score.
Diagnostic arthroscopy of the ipsilateral knee was performed due to persisting postoperative knee pain in 2 cases (6% of patients). The first case was a 20-year-old patient who underwent arthroscopy 9 months after OAT. Intraoperatively, a sufficient layer of surrogate cartilage was seen to have formed at the donor site; no further damage of articular cartilage was noted. The patient’s knee pain resolved with time; 43 months after surgery the patient scored 95 points on the HSS Patella Score. The second patient was 41 years of age and had suffered from retropatellar osteoarthritis stage III-IV before OAT had been performed. Arthroscopy showed no deterioration of retropatellar osteoarthritis but brought little relief. Twenty-two months after surgery, the patient scored 35 points on the HSS Patella Score.
On magnetic resonance imaging of the osteochondral graft, no necrosis of the graft was seen. Some hyperintense signal of both graft and surrounding bone was present in all patients. We saw no significant difference of the time elapsed since OAT between patients with less than 50% and those with more than 50% hyperintense bone signal of the osteochondral graft (P = 0.749, Mann-Whitney U test) with the numbers available in our study. MRI findings are depicted in Table 3; an example is shown in Figure 3B.
Results of Magnetic Resonance Imaging (n = 28)
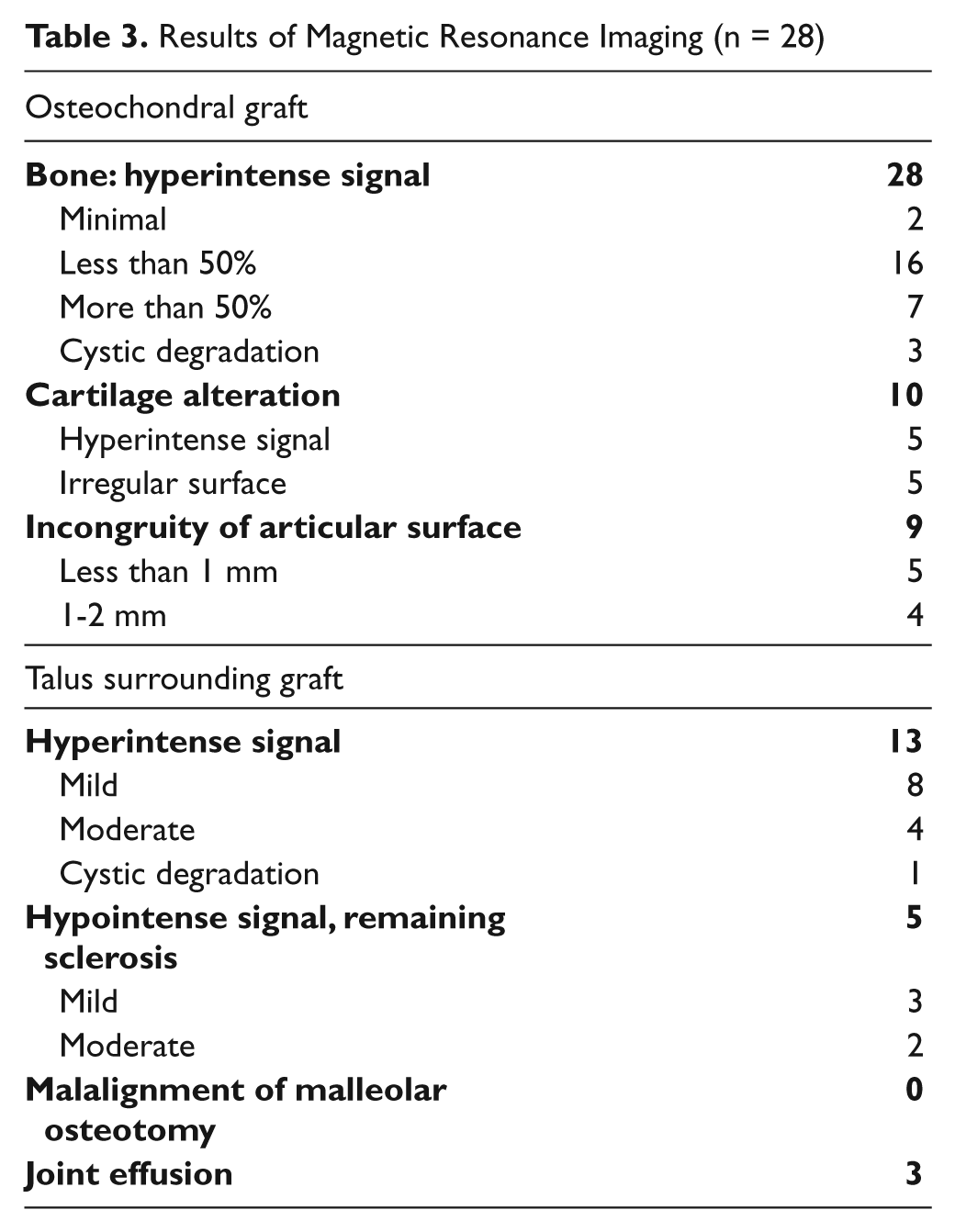
With the numbers available in our study we found no significant difference of ankle pain rated on VAS and AOFAS score results between patients with articular incongruity more than 1 mm and those with minor or none incongruity (P = 0.0666 and P = 0.868, respectively, Mann-Whitney U test). Furthermore, we saw no significant difference of AOFAS scores (P = 0.183, Mann-Whitney U test) or VAS ankle pain (P = 0.501, Mann-Whitney U test) in patients with or without abnormal MRI findings in general (irregular and/or hyperintense cartilage of graft, incongruity of articular surface more than 1 mm, persisting sclerosis of surrounding bone, cystic degradation of graft or surrounding bone, joint effusion; n = 14).
Discussion
This study represents one of the largest groups of patients with osteochondritis dissecans of the talus who received osteochondral autologous transplantation. We saw good clinical results of OAT harvested from the ipsilateral lateral femoral condyle with or without malleolar osteotomy after an average follow-up of 29 months. Postoperative functional level of the ankle joint was high (median AOFAS score 86 points), pain level was low (2.0 on VAS), and complications were uncommon.
Our clinical results concur with those in the literature even though in most study groups the etiology of osteochondral lesions was much more varied than in ours (Table 4): Whereas in our study the only indication for osteochondral autologous transplantation was osteochondritis dissecans stage III or IV, most study groups included osteochondral lesions of any etiology (ie, degenerative, traumatic, osteochondritis dissecans). As our findings concur with those in literature, it may be assumed that clinical results of osteochondral autologous transplantation are mostly independent of the etiology of the osteochondral lesion. We saw no relevant difference between our clinical results and those of study groups performing alternative operative techniques such as tibial wedge osteotomy for operative exposure or harvesting of the osteochondral graft from the medial calcaneus or ipsilateral talar articular facet.16,23,27 However, as these studies only include a small number of patients, the superiority or inferiority of these alternative operative techniques remains unclear.
Comparison of Clinical Results After Autologous Osteochondral Transplantation of the Talus
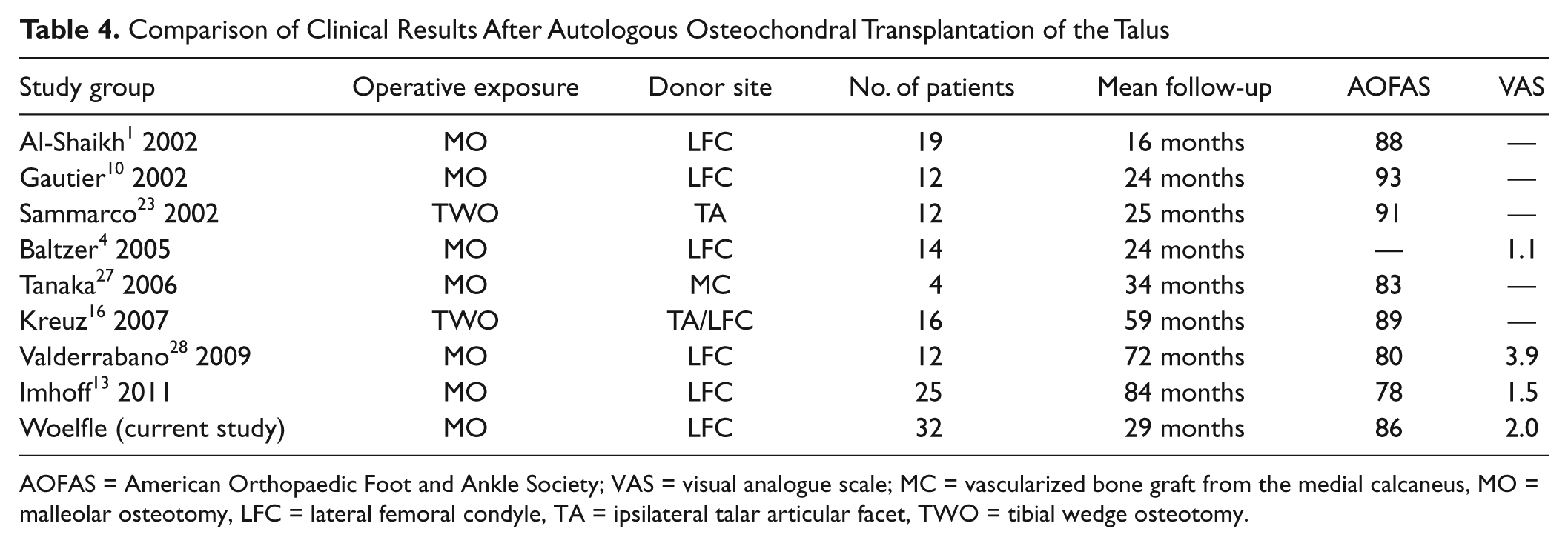
AOFAS = American Orthopaedic Foot and Ankle Society; VAS = visual analogue scale; MC = vascularized bone graft from the medial calcaneus, MO = malleolar osteotomy, LFC = lateral femoral condyle, TA = ipsilateral talar articular facet, TWO = tibial wedge osteotomy.
In our study donor site morbidity of the ipsilateral knee joint was low (median HSS Patella Score 95 points). To evaluate donor site morbidity, the HSS Patella Score was chosen in this study, even though this score was originally developed to quantify anterior knee pain in total knee arthroplasty. 3 In our view, this score allows for a very precise quantification of both subjective (anterior knee pain on rising, descending stairs, etc) and objective (crepitus, tenderness, etc) findings to be expected after harvesting the osteochondral graft from the lateral femoral condyle.
The low donor site morbidity found in our study concurs with data published by Gautier et al, Paul et al, and Al-Shaikh et al (Table 5). They investigated donor site morbidity after osteochondral autologous transplantation of the talus1,10 and various other locations 20 with the lateral femoral condyle as harvest site and found good clinical results. By contrast, other recent studies demonstrate that donor site morbidity can be considerable: Reddy et al found a Lysholm score of only 81 points at 47 months after harvesting an osteochondral graft from the asymptomatic knee, 22 and Valderrabano et al noted complaints of knee pain in 50% of the patients. 28 The difference in donor site morbidity might be associated with the location of the harvest site; biomechanical studies on 7 cadaveric knees showed that patellofemoral contact pressure decreases as one moves distally along the lateral trochlea. Thus, the graft should be harvested as distally as possible—just proximal to the sulcus terminalis of the lateral femoral condyle. 9
Comparison of Clinical Results at Donor Site After Autologous Osteochondral Transplantation
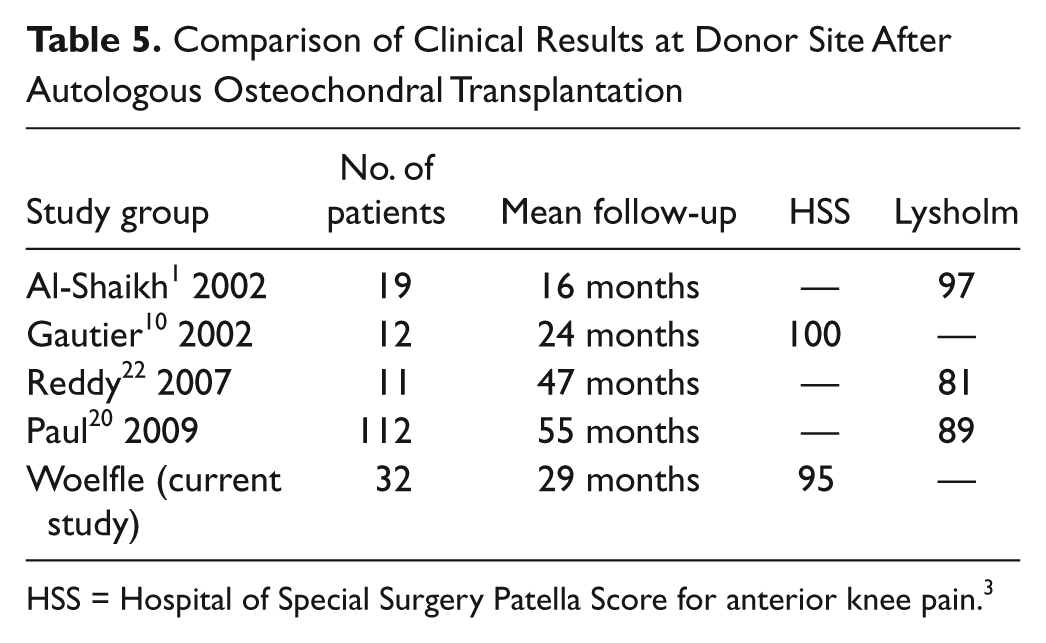
HSS = Hospital of Special Surgery Patella Score for anterior knee pain. 3
Magnetic resonance imaging of the talus showed no case of osteonecrosis of the osteochondral graft. However, in half of our patients some abnormal MRI findings were seen, for example, incongruity of the articular surface more than 1 mm, cystic degradation of the graft or surrounding bone, irregular and/or hyperintense cartilage of the graft, persistent sclerosis of surrounding bone, or joint effusion. The diagnostic value of MRI in osteochondral autologous transplantation, however, remains unclear. With the numbers available, we found no significant difference of AOFAS score or ankle pain rated on the VAS when MRI findings were abnormal. This is consistent with findings by Kokkinakis et al and Links et al; Kokkinakis et al saw no correlation between clinical outcome and MRI findings such as articular step-off, subchondral laminar irregularity, or subchondral edema in patients with osteochondral transplantation of both ankle (n = 13) and knee (n = 20) joint. 15 Link et al did not observe that incongruity of the articular surface, bone marrow edema or even osteonecrosis of the graft were related with pain at rest. 19 Only Imhoff et al found a correlation between major incongruity (> 1 mm) of the articular surface and lower AOFAS score results. 13 This statistical correlation, however, could not be confirmed in our study. In almost all patients, some hyperintense signal of the graft and/or the surrounding bone was observed. This concurs with MRI findings by Baltzer et al where they found that enhanced signal intensity is still visible up to 3 years after osteochondral transplantation. 4 However, their hypothesis that this enhanced signal intensity disappears slowly with time could not be confirmed by MR findings in our study: There was no significant difference of the time elapsed since surgery between patients with less than 50% hyperintense bone signal and those with more than 50%. As the clinical relevance of the MRI findings mentioned previously still remains unclear, abnormal MRI findings in the postoperative course should be regarded with caution.
This study’s weakness was the comparatively short follow-up and the retrospective design, which did not allow for a comparison of preoperative and postoperative scores. Major strengths of the study were the homogeneity of the study group, as it consisted exclusively of patients with osteochondritis dissecans, and the number of patients included in the study, which is one of the largest in the current literature.
Conclusion
Osteochondral autologous transplantation from the ipsilateral lateral femoral condyle in osteochondritis dissecans of the talus was a safe procedure with low donor site morbidity and good clinical results. With the numbers available in our study, we did not find a significant difference in the clinical outcome between patients with abnormal MRI findings and those without; thus, the value of MRI in postoperative follow-up might be limited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.