
Abstract
Background:
To evaluate the prevalence of osteomyelitis in different areas of the foot and the possible correlation between localization and outcome of major amputation.
Methods:
From January 2008 to December 2010, a total of 350 diabetic patients were admitted to our diabetic foot unit for the surgical treatment of osteomyelitis. Osteomyelitis was diagnosed when both the probe-to-bone maneuver and plain radiography were positive. In all of these patients, osteomyelitis was confirmed by histological examination.
Results:
Osteomyelitis was localized to the forefoot in 300 (85.7%) patients, to the midfoot in 27 (7.7%) patients, and to the hindfoot in the remaining 23 (6.75) patients. On average, foot lesions had developed 6.6 ± 5.6 months before admission to our unit. Transtibial amputation was performed in 1 (0.33%) patient with forefoot osteomyelitis, in 5 (18.5%) patients with midfoot osteomyelitis, and in 12 (52.2%) patients with osteomyelitis of the heel (χ2 = 128.4, P < .001). Multivariate analysis showed the independent role that osteomyelitis in the heel region had in major amputation outcome (odds ratio 15.3; P < .001; confidence interval, 17.4-5336.0), dialysis treatment (odds ratio 6.3; P = .012; confidence interval, 2.5-1667.2), and leukocyte count greater than 103 mm3 (odds ratio 2.25; P = .036; confidence interval, 1.1-76.6).
Conclusions:
We found a higher rate of transtibial amputation when osteomyelitis involved the heel instead of the midfoot or forefoot in diabetic patients.
Level of Evidence:
Level III, retrospective comparative series.
Osteomyelitis is a common and serious complication of diabetic foot wounds. Almost 20% of diabetic patients with an infected foot ulcer will develop osteomyelitis; according to some case studies, osteomyelitis may occur in up to 66% of diabetic patients with foot ulcers.8,11 Usually, osteomyelitis is a complication of a preexisting, longstanding nonhealing ulcer, thus allowing the infection to spread into the bone. 5 Major amputation is required more often in patients with osteomyelitis, especially if it is accompanied by a deep soft tissue infection. 10
Many studies have evaluated the localization of foot lesions and the outcome of forefoot, midfoot, or heel wounds30,25,28; however, few studies have compared the outcome of diabetic ulcers localized to different areas of the foot.13,22,27 To our knowledge, no studies have evaluated the localization of osteomyelitis in different areas of the foot; in 2009-2010, only 2 studies mentioned the site of osteomyelitis.9,17 However, both of these studies focused on 1 site rather than evaluating different areas of the foot. Thus, there seems to be a paucity of studies focusing on the prevalence of osteomyelitis in the forefoot, midfoot, and heel and the possible outcomes. The aim of this retrospective study was to evaluate the prevalence of osteomyelitis in different areas of the foot and its possible correlation with the outcome of major lower limb amputation.
Methods
Protocol
In all diabetic patients referred to our outpatient clinic because of foot ulcer, osteomyelitis was suspected when the bone was exposed or the probe-to-bone maneuver was positive and plain radiography of the involved foot had findings consistent with osteomyelitis (lytic lesions, periosteal reaction). 14 Osteomyelitis in the forefoot was diagnosed when both these tests were positive. 1 If the foot lesion involved the midfoot or the heel, a magnetic resonance imaging study was required to confirm the diagnosis. 18 In our protocol, all diabetic patients with osteomyelitis were eligible for surgical “curative” class of treatment according to the classification of diabetic foot surgery described by Armstrong and Frykberg. 2
At the initial visit, debridement of the ulcer was performed if necessary. A biopsy sample for microbial culture was obtained after wound debridement to avoid contamination and optimize identification of pathogens; parenteral antibiotic therapy, which was modified during the following visits according to the culture results, was begun. Patients then returned once a week. After 4 weeks of antibiotic therapy and local dressing changes, if osteomyelitis had been confirmed by plain radiography patients were admitted for surgical elective therapy using the technique described by Sanders. 24 The portion of infected bone removed underwent a histological examination. According to the culture results, all patients were treated with intravenous antibiotics during hospital stay. All patients were evaluated to identify the presence of neuropathy, chronic critical limb ischemia, metabolic control, and comorbidities. Peripheral neuropathy was detected by means of vibration perception threshold greater than 25 V with a biothesiometer (Neurothesiometer SLS, Nottingham, UK), absence of sensitivity in more than 5 of 9 foot points with a Semmes-Weinstein 10-g filament, and absence of Achilles tendon reflex.
According to the TransAtlantic Inter-Society Consensus (TASC II) parameters, critical limb ischemia was diagnosed if transcutaneous oxygen tension at the dorsum of the foot was less than 30 mm Hg and ankle pressure was less than 70 mm Hg, when assessable (ankle pulses not detectable or noncompressible foot arteries because of medial calcifications). 21
All patients with these parameters underwent an angiographic study, and if an obstruction of greater than 50% of the vessel diameter was present, percutaneous transluminal angioplasty was performed in the same session as a first-choice revascularization procedure. In patients in whom percutaneous transluminal angioplasty was unsuccessful, a bypass graft was considered.
In patients with fasting glycemic value greater than 140 mg/dL and postprandial glycemic value greater than 180 mg/dL, a new insulin regimen was initiated. Blood glucose level was measured 7 times per day.
For each patient, all of the following variables were recorded: gender; age; type, duration, and treatment of diabetes; and history of cardiac disease, stroke, diabetic retinopathy, and hypertension. The laboratory variables assessed were blood glucose level on admission, glycosylated hemoglobin level, serum creatinine, C-reactive protein, and leukocyte count.
After surgical intervention, every patient with a dorsal ulcer was given a therapeutic shoe. All patients with plantar ulcers received pressure relief of the affected limb using a nonremovable fiberglass off-loading cast.
Complications
Any event that required specific medical or surgical treatment or prolonged hospital stay following surgical procedure was recorded and was considered a complication.
Follow-Up
After hospital discharge, all patients were maintained with oral antibiotics until the ulcer healed. Patients were seen in clinic weekly until complete wound healing and during the first month and bimonthly thereafter. The aim of the visits was to verify compliance with the treatment. The orthoses consisted of insoles prepared on plaster cast and rigid sole footwear. The shoes were made with rigid rocker soles, with extra depth to fit customized insoles and soft thermoformable leather that adapted to toe deformities (MAC 2 Optima Molliter, Civitanova Marche, Italy). The customized insoles were shaped by cast using Alcapy, a material derived from PPT (Professional Protective Technology, Deer Park, NY) and designed to relieve local pressure, and by Alcaform, a material derived from Plastazote and designed to absorb high pressure points. The insoles were modified or changed every 6 months, and the shoes were modified according to wear.
Furthermore, we supplied patients with household slippers made of a rigid sole so that the insoles could be used at home.
Outcome Measures
The primary end point of the study was major amputation as it related to forefoot, midfoot, or heel localization of the osteomyelitis. Limb salvage was deemed successful if the patient was able to bear weight on the plantar aspect of the foot, even if this was achieved by a tarsometatarsal amputation, and if the patient was able to walk without the aid of crutches or prosthetic leg. A major amputation was performed in patients in whom the lesion extended above the Chopart joint. Any amputation proximal to the ankle was considered a major amputation. The secondary end point was the evaluation for possible association of the considered variables with the major amputation.
Statistical Analysis
Descriptive statistics of the whole population were reported; differences between the patients with forefoot, midfoot, or heel ulcers were tested using the Student t test for mean values, standard deviation for the continuous variables, and the Pearson’s chi-square test for discrete variables. The 95% level was adopted for the confidence intervals, and the 5% level was considered to test the null hypothesis. The presence of any statistically significant difference in major amputation was assessed using Pearson’s chi-square test.
Correlation between major amputation and characteristics of the studied population was tested with a univariate logistic regression. A P value of .05 was considered sufficient to reject the null hypothesis. The same analysis was carried out with multivariate logistic regression and stepwise selection of independent variables to determine independent factors associated with major amputation. All results were evaluated using the statistical package SPSS 18 (Statistical Package for Social Science, IBM Corporation, Somers, NY).
Results
From January 2008 to December 2010, a total of 350 diabetic patients were admitted to our diabetic foot unit for surgical treatment of osteomyelitis. In all these patients, osteomyelitis was confirmed by the histological examination of the portion of bone removed during the surgical treatment. Patients with abscess or gangrene and patients with history of Charcot arthropathy or with Charcot diagnosis at magnetic resonance were excluded from the study population.
In 300 (85.7%) patients, the osteomyelitis was localized to the forefoot; in particular, it was localized to the toes in 136 (38.9%) patients and to the metatarsals in 164 (46.9%) patients. In 27 (7.7%) of the 350 patients, osteomyelitis was localized to the midfoot and was localized to the heel in the remaining 23 (6.7%) patients. The demographic and clinical characteristics of the 3 groups of patients are reported in Table 1.
Demographic and Clinical Characteristics of the Three Groups of Patients a
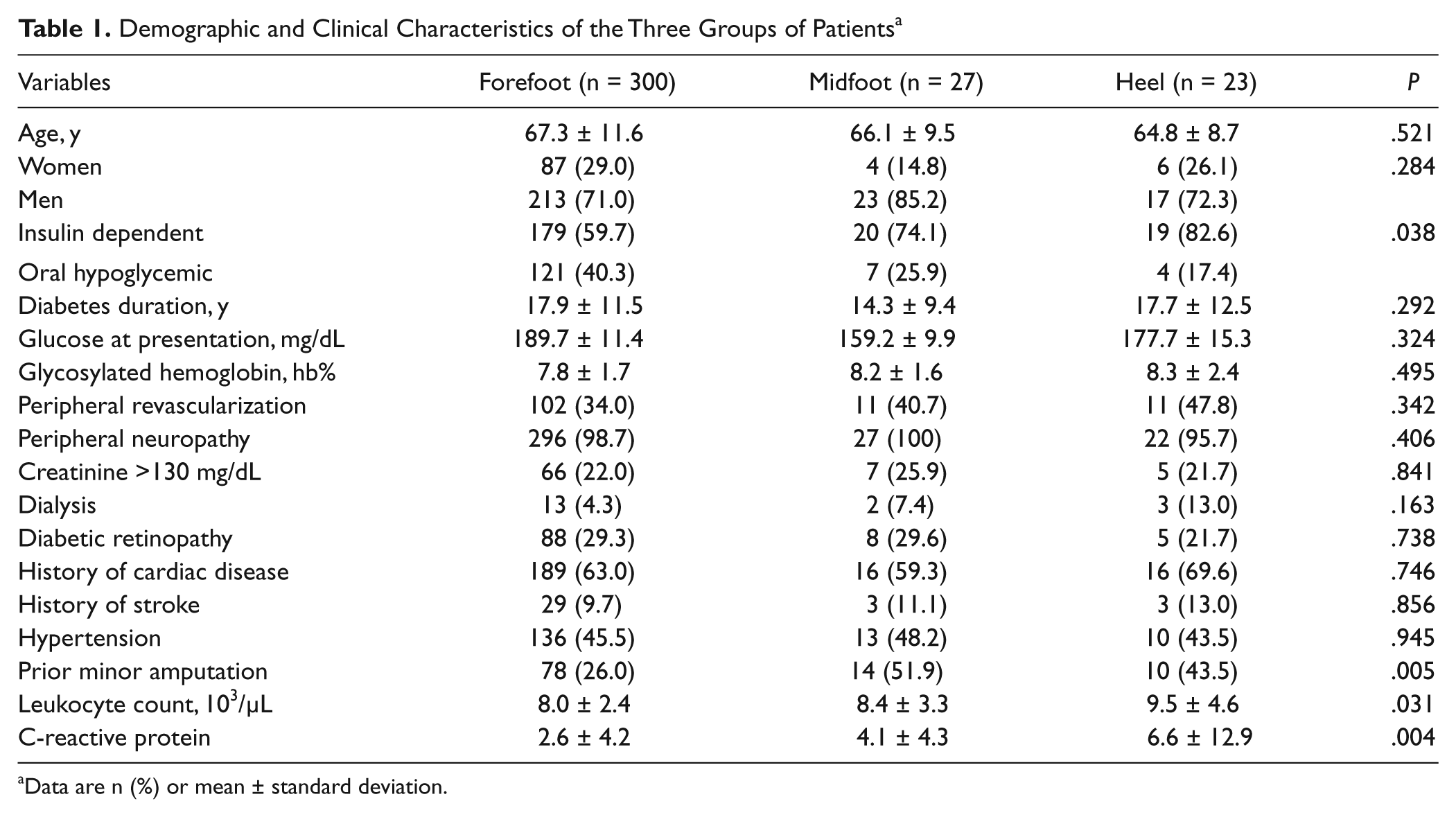
Data are n (%) or mean ± standard deviation.
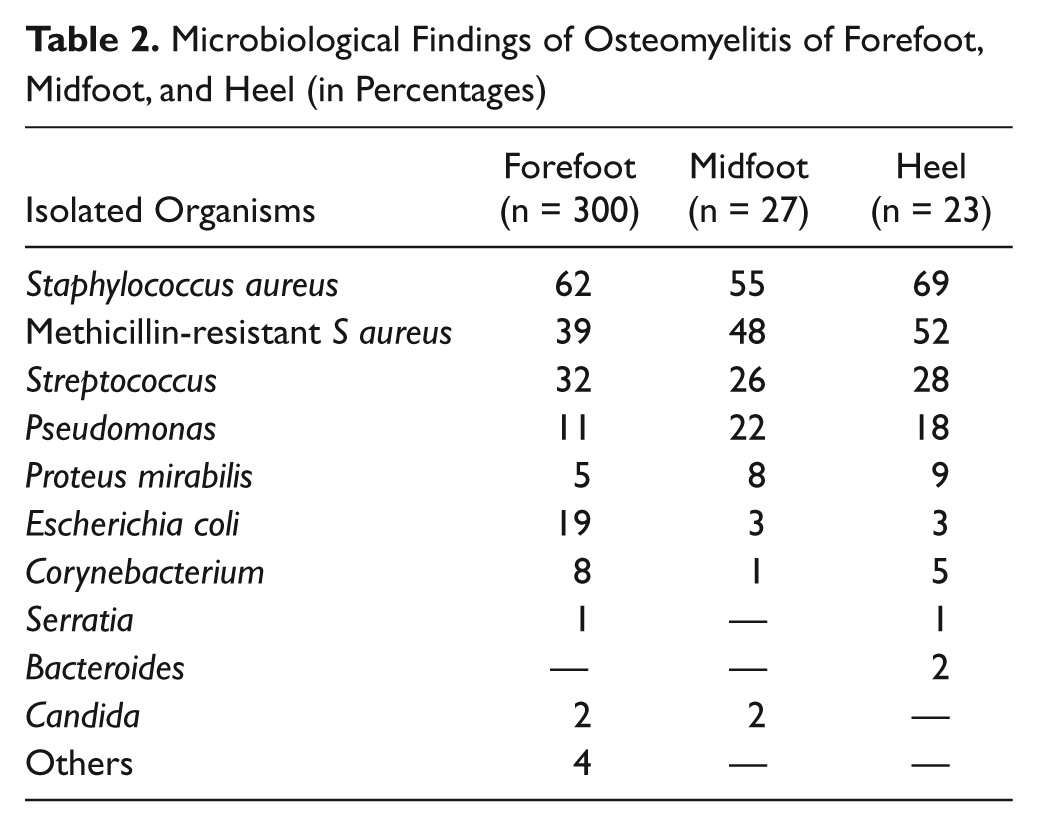
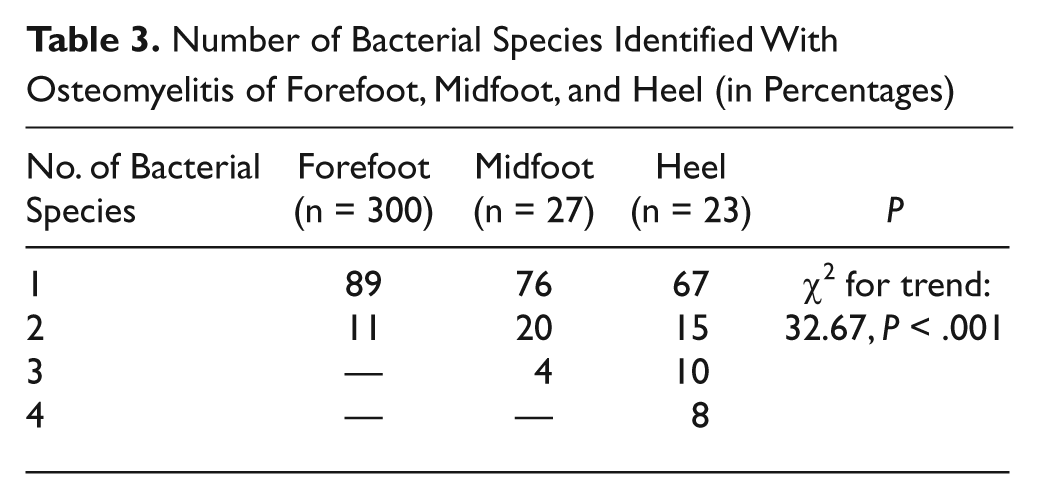
Table 2 reports the microbiological findings and Table 3 reports the number of bacterial species identified by culture examination. The average time to onset for the foot lesions was 6.6 ± 5.6 months (P = .353).
Microbiological Findings of Osteomyelitis of Forefoot, Midfoot, and Heel (in Percentages)
Number of Bacterial Species Identified With Osteomyelitis of Forefoot, Midfoot, and Heel (in Percentages)
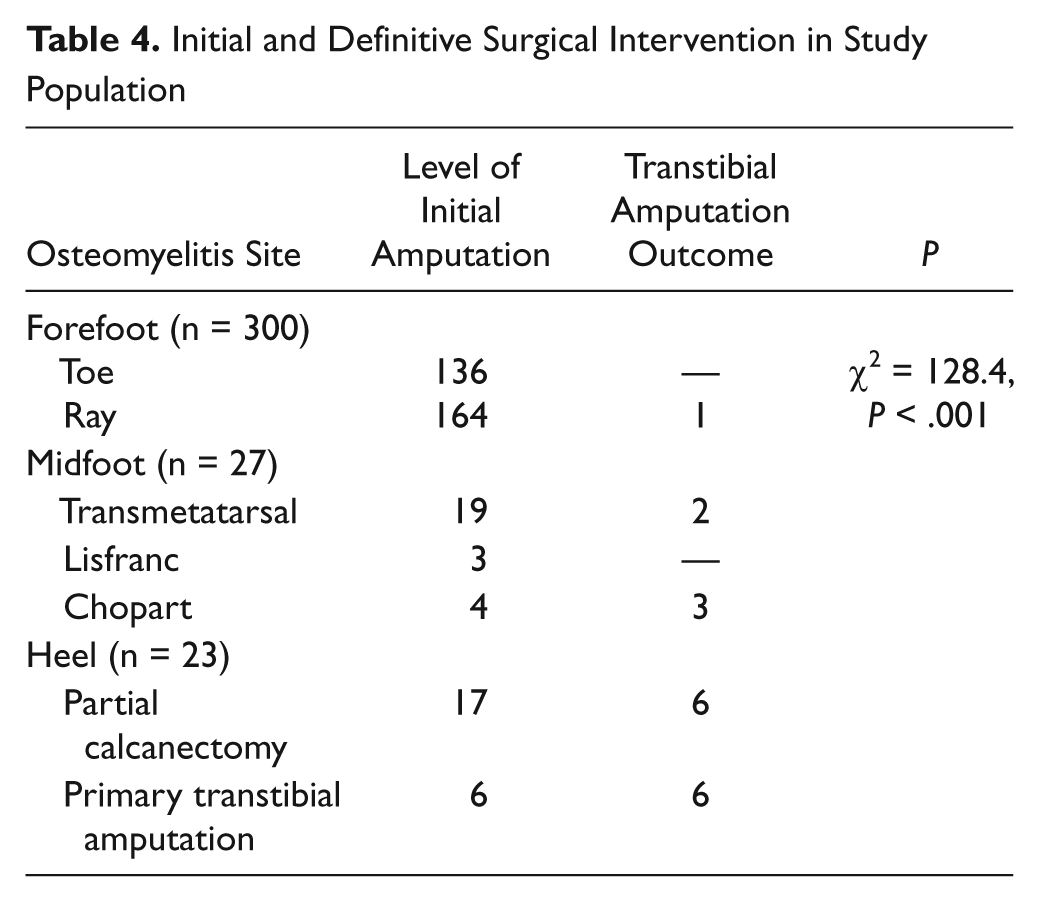
Transtibial amputation was performed in 1 (0.33%) patient with forefoot osteomyelitis, in 5 (18.5%) patients with midfoot osteomyelitis, and in 12 (52.2%) patients with osteomyelitis of the heel (χ2 = 128.4, P < .001). Table 4 reports the initial level of amputation and the outcome of transtibial amputation. The average hospital stay for patients with osteomyelitis of the forefoot was 3.8 ± 1.8 days, for patients with midfoot osteomyelitis 4.9 ± 2.1 days, and for patients with osteomyelitis of the heel 7.1 ± 3.5 days (P < .001). The univariate logistic analysis results of the association of the variables considered with major amputation are summarized in Table 5.
Initial and Definitive Surgical Intervention in Study Population
Univariate Logistic Analysis of Transtibial Amputation (n = 18) vs Study Population as a Whole (N = 350)
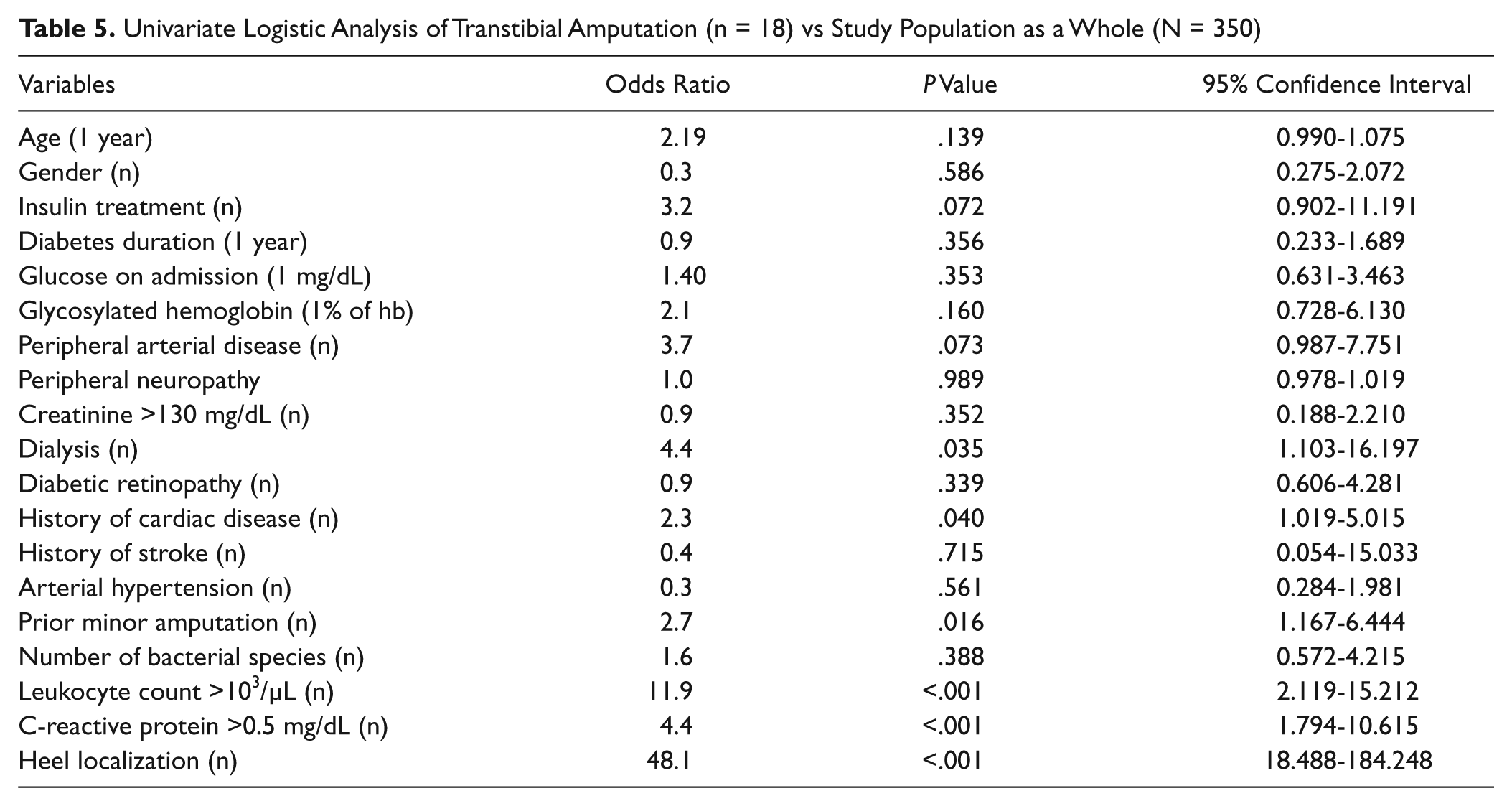
Multivariate analysis showed the independent role that osteomyelitis in the heel region had on major amputation (odds ratio 15.3; P < .001; confidence interval, 17.4-5336.0), dialysis treatment (odds ratio 6.3; P = .012; confidence interval, 2.5-1667.2), and leukocyte count greater than 103/µL (odds ratio 2.25; P = .036; confidence interval, 1.2-76.6).
Discussion
Osteomyelitis can be difficult to diagnose, and its treatment has been the subject of controversy.12,16 A bone biopsy is the gold standard for diagnosing osteomyelitis. However, because of the invasive nature of this method and the frailty of subjects such as diabetic patients, it has been a long time since we have used this diagnostic technique to differentiate between Charcot neuropathy and osteomyelitis. 4 According to our protocol, osteomyelitis was diagnosed when both the probe-to-bone test and standard radiography of the forefoot lesion were positive. Moreover, if the foot lesion involved the midfoot or the heel, a magnetic resonance imaging study was always required to confirm the diagnosis. 20 The high specificity of this diagnostic approach was indicated by the fact that osteomyelitis was confirmed at histological examination in all patients in our study. 29
The selection of the best therapeutic approach has also been matter of debate. 23 Despite the fact that 2 guidelines have been published on osteomyelitis treatment, current approaches may differ greatly.6,19 Some studies highlighted the efficacy of antibiotic therapy alone, whereas other studies revealed that bone infection was more effectively treated by proper antibiotic treatment combined with surgery.15,26
Many studies have examined the effectiveness of medical or surgical approaches in the treatment of osteomyelitis of the foot, but there is a paucity of data on the relevance of the site of osteomyelitis on prognosis for amputation.
The results of our study clearly show that localization of the osteomyelitis to the heel posed very high risks for amputation of the whole foot. Primary amputations were only performed when osteomyelitis was localized to the heel; the spread of osteomyelitis prevented a partial calcanectomy. The high rates of amputations after partial calcanectomy in our series demonstrate our efforts to preserve the extremity, even using approaches at high risk of failure.3,7
The localization of osteomyelitis to the midfoot posed less risk for an amputation above the ankle, yet the risk was much higher than that observed in patients with osteomyelitis of the forefoot.
In this study, all patients with osteomyelitis underwent surgical treatment, and therefore we cannot comment on conservative therapy with antibiotics without surgery.
Some points should be emphasized. Because of prolonged, ineffective treatment, much time elapsed between occurrence of wounds and the osteomyelitis diagnosis in our center. In addition, osteomyelitis of the toes may only affect the toes. Osteomyelitis of the midfoot bones may extend to the hindfoot, thus compromising the heel and/or the ankle, leading to a high risk for an amputation above the ankle. In fact, a transtibial amputation was performed in only 1 patient, due to concomitant cardiovascular–renal complications that required a prolonged stay in bed with consequent onset of new foot lesions. In contrast, an unsuccessful therapeutic approach had devastating consequences in patients with osteomyelitis of the midfoot and even more so in patients with osteomyelitis of the heel. Thus, the question arises whether more prompt, proper surgical treatment, allowing the wound to heal faster, could have changed the outcome. Such a retrospective study does not allow conclusions regarding the best approach to treat osteomyelitis of the midfoot or heel.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.