
Abstract
Background:
The safety of posterior ankle arthroscopy is still the subject of debate. The purpose of this study was to evaluate the anatomical relationship between the posterior portals and the neurovascular structures using magnetic resonance imaging (MRI) to determine the safety of posterior portals in posterior ankle arthroscopy.
Methods:
Forty ankles from 38 patients who had undergone MRI scanning for ankle disorders were assessed (18 males, 20 females). For each ankle, the angles of the presumed position of the portals to the posterior neurovascular structures and the malleoli were measured on 4-mm proximal slices from the anterior tip of the fibula. The shortest distance from the sural nerve and the tibialis posterior neurovascular bundle to the position of the posterior portals was measured.
Results:
The average distance between the posteromedial portal and the tibialis posterior neurovascular bundle was 18 ± 3 mm, whereas the average distance between the posterolateral portal and the sural nerve was 15 ± 3 mm. In 100% of ankles, there were no neurovascular structures lying within the region between the anterior tip of fibula and the posteromedial portal or between the posterior tip of fibula and the posteromedial portal. In 32 ankles (80%), the medial neurovascular structures were present on the medial side of the line running between the anterior tip of medial malleolus and the posteromedial portal.
Conclusion:
The posterior neurovascular structures were not in immediate proximity to where we estimated the posteromedial and posterolateral portals to be located.
Clinical Relevance:
The findings of the present MRI-based study suggest that arthroscopic instruments oriented toward the fibula may be safely introduced into the posterior ankle without injuring the neurovascular structures.
Posterior ankle disorders pose a diagnostic and therapeutic challenge to surgeons, owing to the deep location of the anatomical structures and lesions within and around the joint. Arthroscopy has therefore become a valuable tool for the diagnosis and treatment of posterior ankle disorders.2,5-7,9,11,13,17,20 Although the use of a 2-portal endoscopic approach to the posterior aspect of the ankle has been reported, 17 the safety of posterior ankle arthroscopy remains controversial.1,3,6,9,14,19 Many studies discourage the use of posteromedial portals because of the increased risk of neurovascular injury.1,3,6,9,14,19 Clinical studies using posterior ankle arthroscopy have described the complication rate of injury to the sural nerve or tibial nerve rate in the range of 0% to 8.3%.2,5,6,7,9-11,13 As such, surgeons are still searching for reproducibility in operative techniques in order to minimize the risk of iatrogenic injury during ankle arthroscopy. Various anatomical studies have assessed the safety, efficacy, and anatomical relationships associated with placement of the posterior portals, describing the distance between posterior portals, neurovascular structures, and the instruments required for surgery.4,8,12,15,16,18 However, during posterior ankle arthroscopy, it is difficult to confirm the distance between the instruments and the neurovascular structures, because it is necessary to first remove the fatty tissue and the joint capsule to reach the target. This is technically demanding, and until the posterior structures are properly identified, there is potential risk to the posterior neurovascular structures. The purpose of this study was to evaluate the anatomical relationship between the position of presumed posterior portals and the underlying neurovascular structures using magnetic resonance imaging (MRI). We hypothesized that there would be a safe direction for instrument placement during posterior ankle arthroscopy.
Methods
Study Participants
The medical records of 40 ankles from 38 patients (18 males, 20 females; mean age 38.1 years; age range, 13-68 years), and their respective axial MRI scans of the ankle taken between January 2007 and December 2010, were retrospectively analyzed. The ankles included in this study had undergone an MRI for ankle disorders (osteochondral lesion of the talus, 16 ankles; soft tissue anterior ankle impingement syndrome, 6 ankles; residual ankle disability after sprain, 18 ankles). All ankles showed no deformation to the ankle structures, as confirmed on anteroposterior and lateral radiographs and on MRI axial, sagittal, and coronal sequences.
Magnetic Resonance Imaging
Imaging was obtained with a 1.0-T clinical unit (NT Intera, Philips Medical Systems, Best, The Netherlands) using a transmit/receive quadrature coil. For all ankles, T2-weighted sequences were obtained in the axial plane with a time to echo of 80 milliseconds, a time to repeat of 3500 milliseconds, and a 4-mm slice thickness, with no slice gap. This slice thickness was routinely used in our clinic as a standard for ankle MRIs. For each axial sequence, stacks were parallel to the articular surface of the distal tibia. For each ankle, the angles of the presumed portals (posteromedial portal and posterolateral portal) to the posterior neurovascular structures and the malleoli were measured on the 4-mm proximal slice, beginning from the tip of the fibula. The portals described for posterior ankle arthroscopy were from the tip of fibula; therefore, measurements were taken in this plane. The positions of the portals were presumed to be 3 mm medial or lateral from the Achilles tendon, because our institute uses the 2.7-mm oblique arthroscope for posterior ankle arthroscopy. The angle measured was created by dropping a perpendicular line toward a line running between the centers of the medial and lateral malleoli and a line running between the portals and neurovascular structures (Figure 1). The center of a malleolus was defined on the slice of ankle joint identified anterior tip and posterior tip of the malleolus (Figure 2). The shortest distances between the posterior portals (posteromedial portal and posterolateral portal) and the sural nerve and the tibialis posterior neurovascular bundle were measured electronically. In addition, the distances between the posterior portals and the lateral and medial malleoli were assessed. All structures were confirmed by 2 orthopedic surgeons.
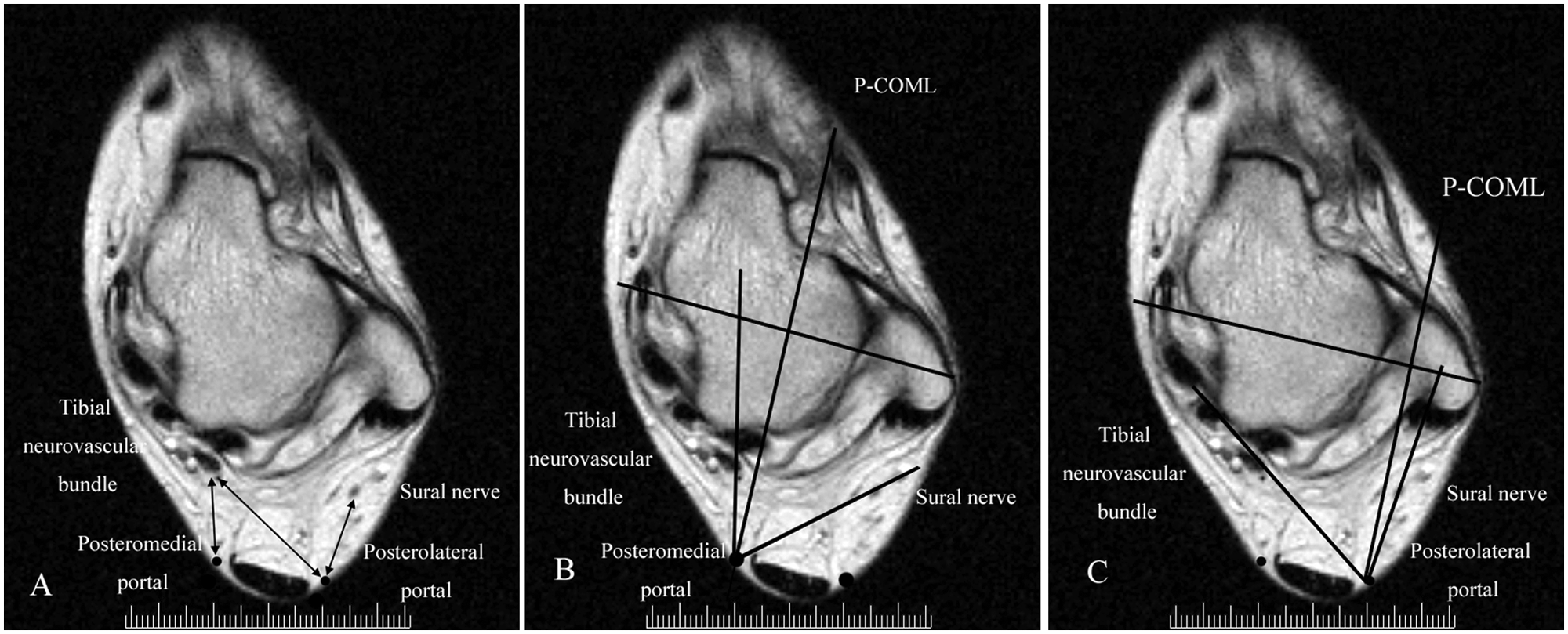
Distances and angles between the portals and the posteromedial neurovascular structures/sural nerve. (A) The distances between the posteromedial portal and the tibialis posterior neurovascular bundle; the posterolateral portal and tibialis posterior neurovascular bundle; and the posterolateral portal and sural nerve are marked with arrows. (B) The angles made by 3 straight lines running between the posteromedial portal and the tibialis posterior neurovascular bundle; and the perpendicular line toward a line running between the centers of the medial and lateral malleoli and the posteromedial portal and the sural nerve. (C) The angles made by lines running between the posterolateral portal and the tibialis posterior neurovascular bundle; the centers of the medial and lateral malleoli; and the posterolateral portal and the sural nerve. P-COML, the line running perpendicular to the line between the center of medial and lateral malleoli.
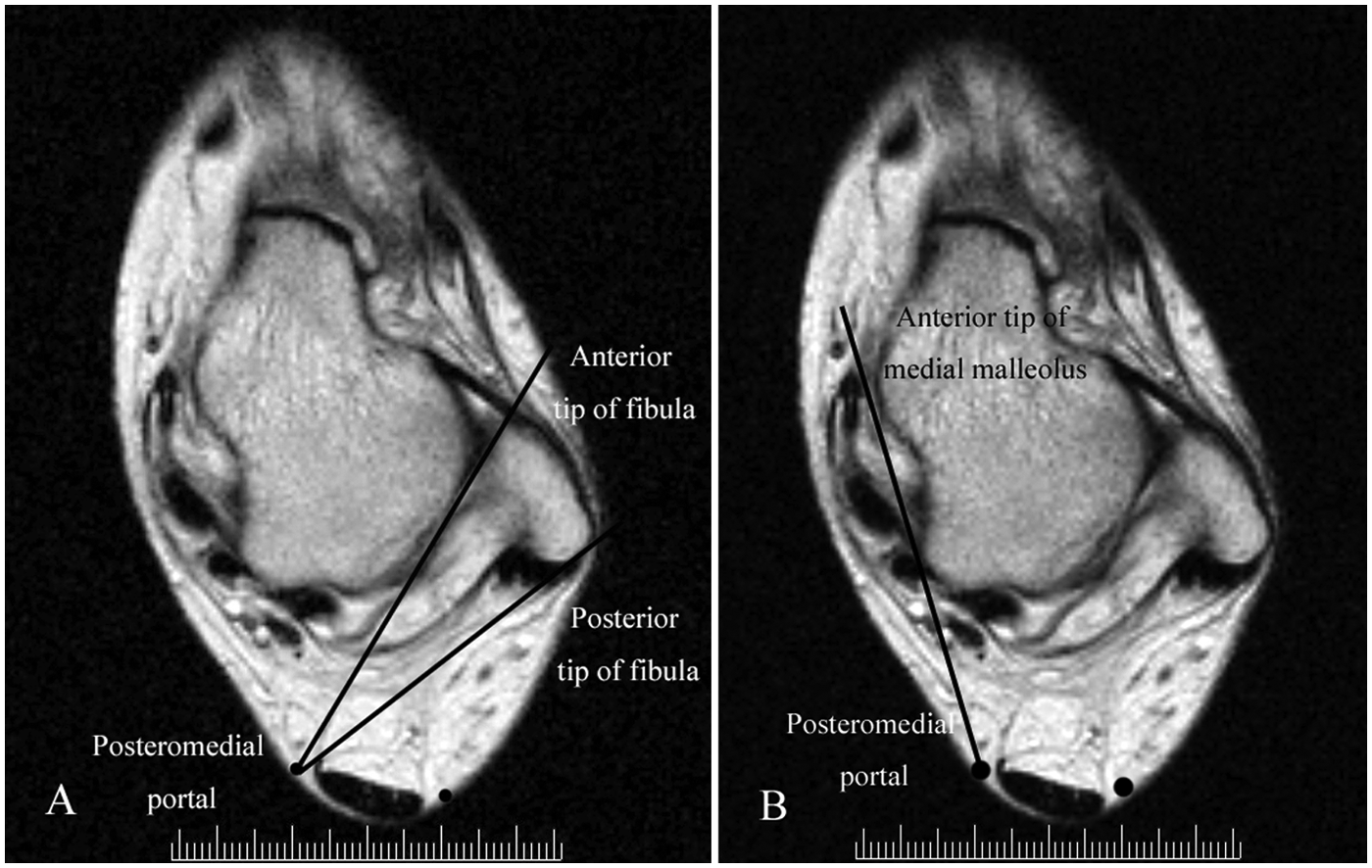
(A) Region between the anterior tip of fibula to the posteromedial portal and the posterior tip of the fibula to the posteromedial portal. (B) Line running from the anterior tip of the medial malleolus to the posteromedial portal.
Results
The mean distances and standard deviations were calculated to determine the distance between the posterior portals and neurovascular structures between each portal and structure (Table 1). The angles of the portals to the posterior neurovascular structures and the malleoli were also determined (Table 2) and were shown to vary widely. In all 40 ankles (100%), there were no neurovascular structures lying within the region between the anterior tip of the fibula and the posteromedial portal or between the posterior tip of the fibula and the posteromedial portal. In 32 ankles (80.0%), the medial neurovascular structures were present on the medial side of the line running from the anterior tip of the medial malleolus to the posteromedial portal. In 8 ankles (20%), the medial neurovascular structures were present along the line running from the anterior tip of the malleolus to the posteromedial portal.
Distance Between the Portals and the Neurovascular Structures
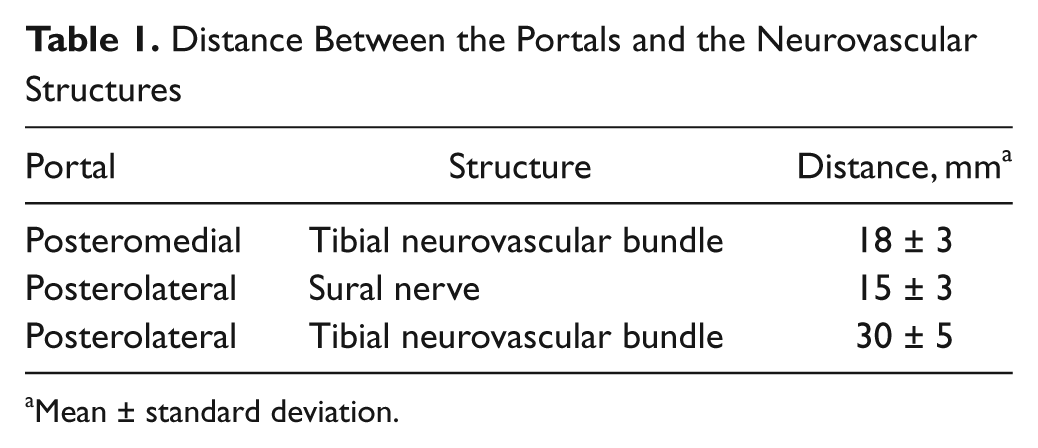
Mean ± standard deviation.
Angles Between the Portals and the Neurovascular Structures
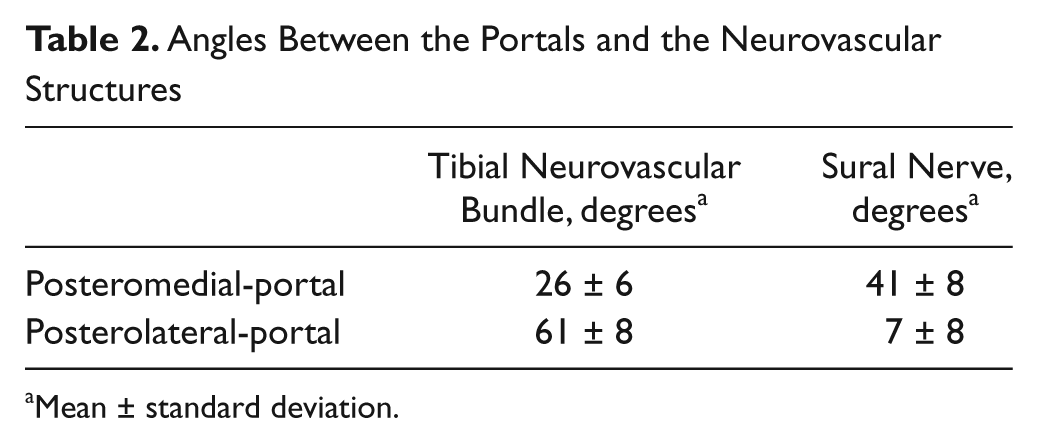
Mean ± standard deviation.
Discussion
In line with previous studies,3,4,8,12,15,16,18,21 we have demonstrated that posteromedial and posterolateral portals can be used with relatively low risk to neurovascular structures in the ankle provided that the instruments are directed toward the fibula from the posteromedial portal when visualization or palpation is impaired or when a reference angle for the posterior ankle structures cannot be attained.
Previous cadaveric studies reported that the distance between the posteromedial portal and the tibial nerve ranged from 7.5 to 14.7 mm, whereas the distance between the posterolateral portal and the sural nerve ranged from 6.0 to 12.6 mm.3,8,18,21 These studies concluded that posteromedial portals should be used with caution. However, the heights of the posterior portals were not published in these studies. Interestingly, several authors advocated for the safety and efficacy of posterior portals in relation to the anatomical position of structures within the ankle, with studies validating the safety of the 2-portal arthroscopic approach for posterior portals.8,17 In cadaveric studies, the distances between the portals and the neurovascular structures are variable, because a clear definition of the posterior portals has not been made. In cadaveric specimens, the posteromedial portal is located on average 13.3 mm from the tibial nerve, 14.7 mm from calcaneal branch of the tibial nerve, and 17.3 mm from the tibialis posterior artery, indicating the relatively low risk of injury from this portal to the surrounding neurovascular structures. In addition, the posteromedial portal is described as being located 1 cm more proximally, making it on average 2.9 mm closer to neurovascular structures. The height of the posteromedial portal also affects the distance between the portals and the neurovascular structures in the posterior ankle. The results of the present study showed similar distances between the posterolateral portal and the sural nerve as well as between the posteromedial portal and the tibialis posterior neurovascular bundle, as observed in other studies. 8 In this study, the presumed portals were defined similarly to those previously defined. 8
MRI has been used to investigate the effect of ankle and hindfoot motions on portal nerve distances. 16 The sural and tibial nerves approached the posterior portals in the dorsiflexion-varus, dorsiflexion-valgus, dorsiflexion-neutral, and neutral-varus positions, indicating that placing the foot in a neutral position provided the greatest margin of safety to the tibial nerve (17 ± 6 mm) and the sural nerve (13 ± 3 mm) using the 2-portal arthroscopic technique. 17 In contrast, others have reported that posteromedial and posterolateral portals could be used with relatively small risk to the neurovascular structures if the patient was placed in the prone position during posterior ankle arthroscopy, assuming a cautious placement of the portals. 14
Most studies have simply investigated the distances between the portals and the neurovascular structures. However, when arthroscopy is performed, it is also important to know the safest direction in which to orient the instruments as well as the safest position for the portals; we could not find other reports investigating the former. The angles of the posterior portals and the position of neurovascular structures vary widely, and thus it is important that surgeons find an appropriate reference angle while performing a posterior ankle arthroscopy. In the 2-portal arthroscopic approach, 17 the flexor hallucis longus is an important landmark to use in preventing damage to the more medially located neurovascular bundle. Usually, the tendon of this muscle can be readily detected through passive mobilization of the big toe. However, in rare cases, such as in patients with a large os trigonum, it is difficult to identify the tendon. In contrast, the medial and lateral malleoli are excellent, safe landmarks for procedures, as they are easily palpable in the prone position during surgery. The findings of our study suggest that if instruments are directed toward the fibula from the posteromedial portal, the surgeon can avoid neurovascular injury in the absence of being able to properly visualize, palpate, and/or find a reference angle for the posterior ankle structures. The instruments should not be angled toward the medial side of the anterior tip of the medial malleolus until the posterior structures are readily visualized. Considering these anatomical data, we too propose that the posteromedial and posterolateral portals can be used with relatively low risk to neurovascular structures in the ankle.
There were several limitations to our study. The first is the use of measurements from MRI scans of 40 ankles with ankle disorders. It is possible that the ankle disorders may have affected the results. The second limitation of this study is that we focused solely on imaging analysis without anatomical analysis using cadaver specimens. Third, the MRI scans of the patients in this study were taken in the supine position, without traction. However, posterior ankle arthroscopy is performed with patients placed in the lateral or prone position. This change in position may alter the soft tissues around the ankle owing to fluid distension, and it is therefore likely that the relationship between the portals and posterior neurovascular structures may be different with different ankle positions. Further investigation is necessary to provide accurate information in this regard.
Conclusion
The results of this study suggest that in the absence of being able to properly visualize or palpate structures in the posterior aspect of the ankle, orienting the surgical instruments toward the fibula from the posteromedial portal will help to avoid neurovascular injury. The instruments should not be directed toward the medial side of the anterior tip of the medial malleolus until the posterior ankle structures can be readily visualized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.