
Abstract
Surgical repair of an acute Achilles tendon rupture is indicated in active individuals who wish to return to a high level of activity.3,9 To achieve high functional outcomes, surgery is aimed at restoring the resting length of the gastrocsoleus muscle-tendon unit. However, retraction of the proximal tendon segment and aggressive intraoperative debridement of the tendon edges can result in substantial ankle equinus at the completion of the procedure. Resting muscle length imbalance may affect postoperative rehabilitation as well as tendon function. Moreover, it may predispose to rerupture, with reported rates ranging from 0% to 5%.2,4,9
We describe a simple technique that allows mobilization of the proximal tendon segment and decreases the intrinsic tension on the tendon repair. In addition to restoring resting tendon length and facilitating postoperative rehabilitation, this may minimize the incidence of rerupture and decrease pressure beneath the incision.
Operative Technique
The patient is placed in the prone position. Although surgery may be performed under general anesthesia, the authors prefer spinal or regional anesthesia as it allows for patients to self-adjust the upper extremities and cervical spine, decreasing the likelihood of brachial plexus injuries and pressure-induced wound complications. 3 The Achilles is approached through a posteromedial longitudinal incision, and the paratenon is opened. The tendon “mop ends” are minimally debrided to retain tissue and to minimize shortening.
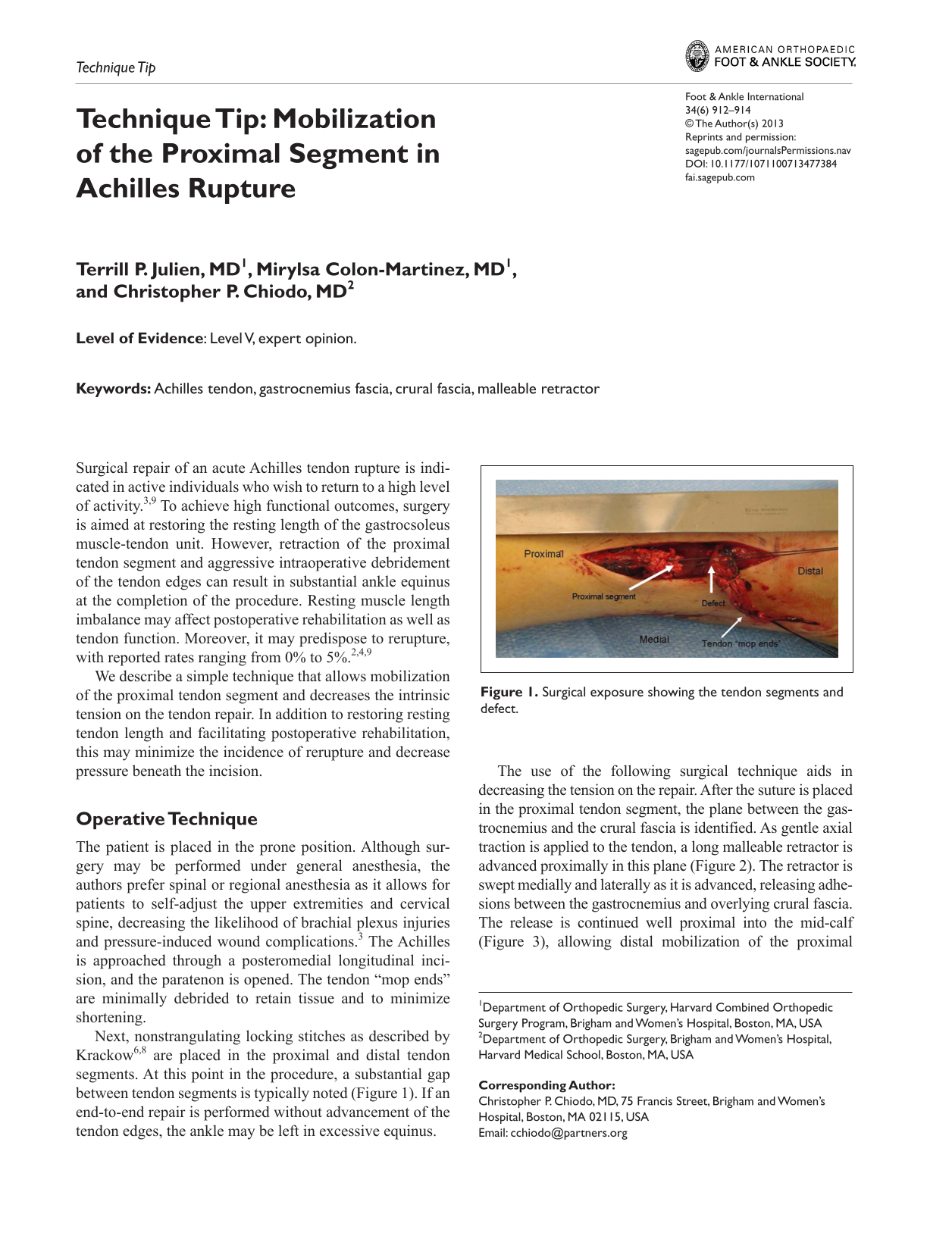
Next, nonstrangulating locking stitches as described by Krackow6,8 are placed in the proximal and distal tendon segments. At this point in the procedure, a substantial gap between tendon segments is typically noted (Figure 1). If an end-to-end repair is performed without advancement of the tendon edges, the ankle may be left in excessive equinus.
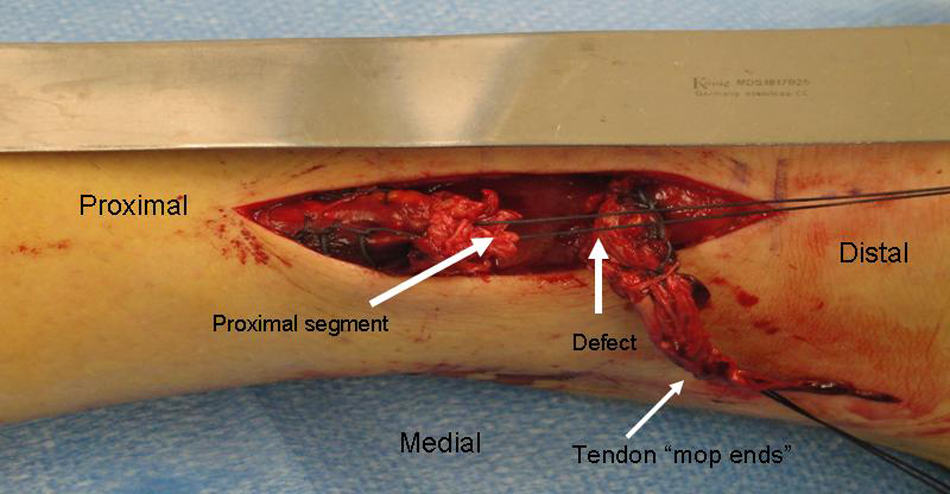
Surgical exposure showing the tendon segments and defect.
The use of the following surgical technique aids in decreasing the tension on the repair. After the suture is placed in the proximal tendon segment, the plane between the gastrocnemius and the crural fascia is identified. As gentle axial traction is applied to the tendon, a long malleable retractor is advanced proximally in this plane (Figure 2). The retractor is swept medially and laterally as it is advanced, releasing adhesions between the gastrocnemius and overlying crural fascia. The release is continued well proximal into the mid-calf (Figure 3), allowing distal mobilization of the proximal tendon segment. There are few if any perforating vessels in this plane, so bleeding is rarely a problem.

Insertion of the malleable retractor.

Proximal extent of release.
With adequate soft tissue release, the ends of the tendon can usually be apposed with little or no tension on the repair (Figure 4). The Krackow stitches are then securely tied down with the ankle in slight (5-10 degrees) plantar flexion. A posterior compartment fasciotomy is performed to facilitate closure of the paratenon.
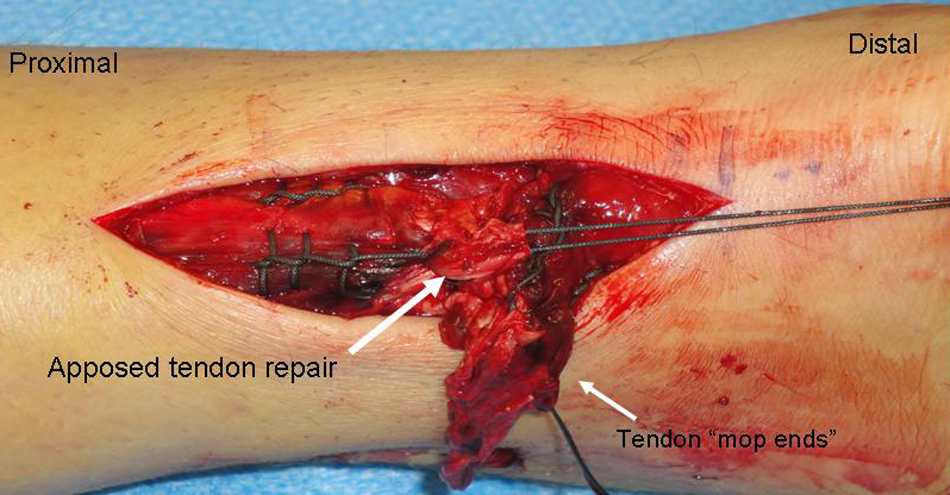
Final apposition of the tendon segments. Note advancement of the proximal segment.
Our postoperative protocol consists of 10 to 14 days of strict non-weight-bearing in the mildly plantar flexed postoperative splint with suture removal 2 weeks after surgery. Active range of motion exercises and partial weight-bearing in a walking boot with a ¼- to ½-inch heel lift are begun at this time as advocated in prior research. 7 At 6 weeks, isotonic resistive exercises may be initiated. Gradual resumption of running is permitted at 12 weeks postoperatively.
Discussion
We have found this technique to be both safe and effective. Typically, 1 to 2 cm of tendon length can be regained. It is acknowledged, however, that we have not systematically measured the amount of tendon excursion gained by this technique. Mobilizing the proximal tendon segment as described often allows us to repair ruptures that are 4 to 6 weeks old without resorting to a V-Y advancement or repairing the tendon with the ankle in excessive equinus.
What is released with this technique? Closer to the rupture, acute adhesions form within 7 to 14 days. 11 It is likely that more proximally, we are releasing adventitial connections between the Achilles and paratenon and as well as between the gastrocnemius and crural fascia. It is also possible that chronic pathological adhesions are being released. Acute Achilles tendon ruptures have been associated with occult tendinopathy,1,5 which, in turn, results in the formation of adhesions between the tendon and paratenon. 10
In addition to previously validated techniques such as the use of nonabsorbable sutures, optimal suture construct, minimal debridement of the tendon edges, augmentation of the repair with a circumferential epitendinous suture, and early range-of-motion exercises, our mobilization technique may aid in decreasing rerupture. Finally, although we have found our technique advantageous, it is important to note that gastrocnemius recession or even V-Y advancement is occasionally necessary in instances with gaps over 3 centimeters. We advocate either of these if a substantial gap persists after mobilization of the proximal segment.
Successful Achilles tendon repair requires meticulous attention to detail. The use of a malleable retractor to mobilize the proximal tendon segment is a safe and straightforward technique that can minimize the gap often encountered during Achilles tendon repair. This decreases the tension on the repair, thereby facilitating the postoperative rehabilitation and potentially decreasing the rate of rerupture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.