
Abstract
Background:
Multiple techniques have been described for reconstruction of the lateral ligaments of the ankle. Most require extensive exposure and dissection, which may lead to potential problems with wound healing, higher risk of nerve injury, fibrosis, and stiffness. This study reports on the results of a minimally invasive method to reconstruct the ligaments using a semitendinosus tendon autograft and achieve a stable ankle while avoiding these problems.
Materials and Methods:
From September 2006 to May 2010, 25 patients (14 males, 11 females) with chronic ankle instability underwent lateral ligament reconstruction. The average age was 32.4 (range, 17 to 62) years old. A semitendinosus autograft was harvested through 2 small knee incisions. For the ankle reconstruction, 4 small incisions of 5 mm each were made at the medial and lateral side of the fibular tip, the talar neck, and the middle of the calcaneus. Anatomical reconstruction of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) was then performed through these small incisions. The mean final follow-up was 32.3 (range, 12 to 56) months. AOFAS questionnaires were used to measure clinical outcomes and donor site morbidity and patient satisfaction are also reported. Preoperative and postoperative stress tests were performed and radiographic parameters were measured.
Results:
The mean AOFAS score increased on average from 71.1 to 95.1 (P < .001). Two patients reported residual instability on uneven ground. No patient reported weakness or disability from the donor site. The satisfaction level was excellent in 20 patients and good in 5 patients. Significant improvement in stress radiographic parameters was noted for the talar tilt angle, with reduction from a mean of 14.0 to 3.8 degrees (P < .001); anterior talar displacement reduced from a mean of 12.3 to 4.6 mm (P < .001).
Conclusion:
Reconstruction of the lateral ankle ligaments using a semitendinosus tendon autograft and a minimally invasive approach can achieve a stable ankle while avoiding extensive exposure and risk of nerve injury.
Level of Evidence:
Level IV, retrospective case series.
Injuries to the lateral ligament complex of the ankle are common in daily life and sports. Most resolve with nonoperative modalities including immobilization and physical therapy. However, approximately 20% to 40% patients present with recurrent instability, which can require surgical correction. Reestablishing ankle stability and proper biomechanics may be important to prevent osteochondral lesions and posttraumatic arthritis. 4
Numerous procedures have been described to correct this problem. Most of them require extensive exposure and dissection, which may lead to potential problems with wound healing and a higher risk of nerve injury, fibrosis, and stiffness. After some years of experience with open procedures, we adopted a new minimally invasive technique for reconstruction of the ligaments of lateral ankle using a semitendinosus tendon autograft. The subjective and objective function as well as radiographic changes of the ankle with this minimally invasive procedure were evaluated in this study.
Methods
Study Sample
Between September 2006 and May 2010, 25 patients who had been diagnosed with chronic ankle instability received minimally invasive reconstruction of the lateral ligaments of the ankle using a semitendinosus tendon autograft. These patients had repetitive ankle sprains and signs of instability despite receiving nonoperative treatment for at least 6 months. The nonoperative modalities included ice, rest, ankle bracing, and activity modification.
This group of patients had at least 1 of the following indications for surgery: repetitive ankle sprains, severe ankle instability (more than 10 degrees of talar tilt or more than 10 mm of anterior drawer), a previously failed Brostrom procedure with a Gould modification, and/or obesity (more than 25 BMI). A contraindication for this procedure included those with functional instability but without mechanical instability on stress radiographs.
The study group included 14 males and 11 females. The average age at the time of surgery was 32.4 (range, 17 to 62) years. The mean final follow-up was 32.3 (range, 12 to 56) months.
Surgical Technique
We performed an arthroscopic examination of the ankle immediately before reconstruction of the lateral ligaments to evaluate and treat any accompanying intra-articular lesions. The patient was positioned supine with a pneumatic tourniquet on the upper thigh. 9
The semitendinosus tendon autograft was harvested with a minimally invasive technique. Two small incisions of 2 cm each were made for tendon harvesting. The proximal one was made at the most medial tendon palpated 2 cm above the joint line, and the distal one was made 2 cm medial to the tibial tuberosity. The 2 ends of the tendon were exposed, and a tendon stripper was applied to free the tendon from the surrounding soft tissue. Then the distal end was released and the tendon was harvested from the proximal incision (Figure 1). The harvested tendon graft was tubularized at both ends with a whip stitch and kept in normal saline solution.
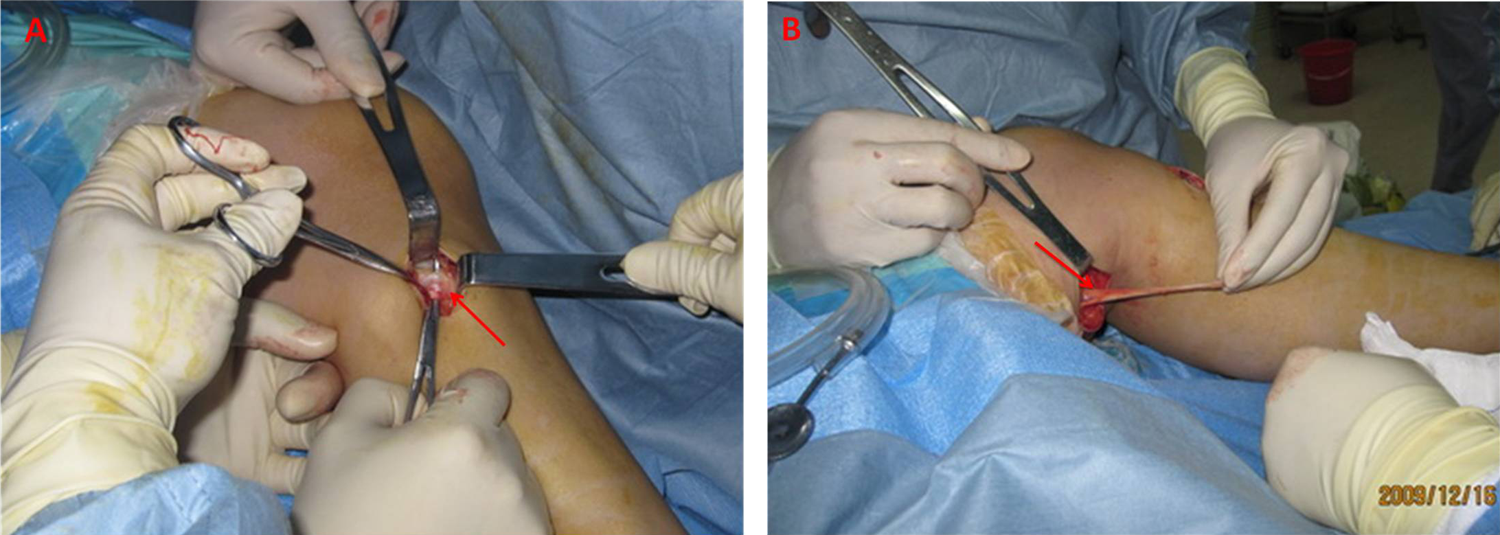
The semitendinosus tendon autograft was harvested with a minimally invasive technique. (A) arrow: distal end of semitendinosus tendon. (B) arrow: proximal end of semitendinosus tendon.
The harvested semitendinosus tendon autograft was used for anatomical reconstruction of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) using a minimally invasive technique. At the recipient site of the ankle, we made 4 small incisions of 5 mm each at the medial and lateral side of the fibular tip, the talar neck, and the middle portion of the calcaneus. Two guide wires were introduced transversely at the distal end of the fibula. Two holes were then drilled over the guide wire from each end to form a tunnel of 4.5 mm in diameter. The prepared semitendinosus tendon autograft was introduced through the tunnel by a long eyelet needle. The ends of the tendon were then passed above the bone surface to the incisions at the talar neck and calcaneus. Guide wires were placed for positioning of talar and calcaneal tunnels under fluoroscopy. A 4.5 mm drill was used to create a tunnel that was widened to 7 mm with an approximate depth of 23 mm. A 7 mm by 23 mm biodegradable inference screw was used to secure the tendon graft in the talar neck initially. Finally, the distal tendon end was inserted into the calcaneus with an interference screw while maintaining tension on the graft without need for transosseous tensioning. The foot and ankle was then examined under fluoroscopy to check the position of the interference screws (Figure 2).
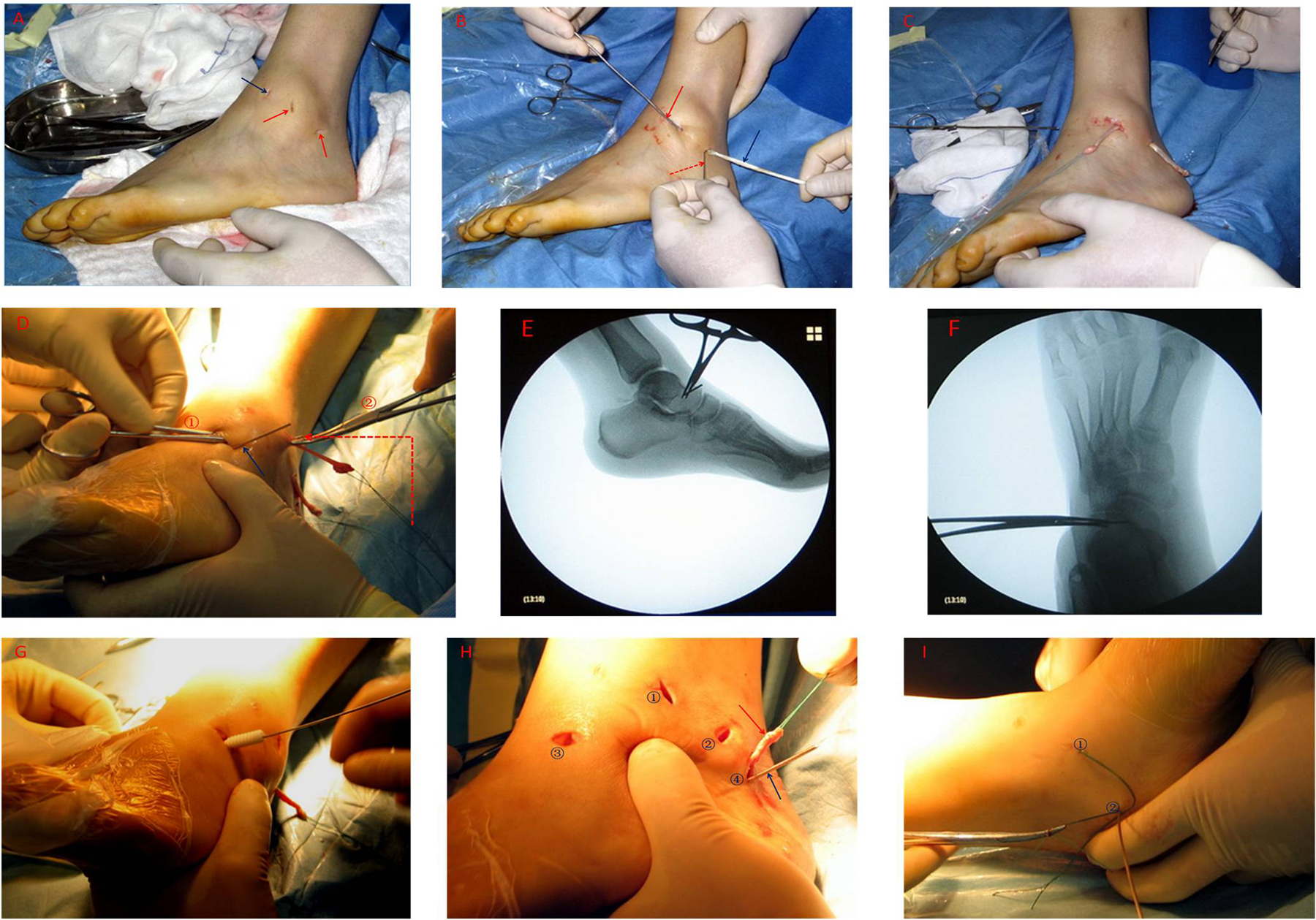
Anatomical anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) reconstruction by semitendinosus tendon autograft with a minimally invasive technique. (A) Red arrows indicate 2 small incisions, 5 mm each, at the lateral malleolus. Blue arrow indicates the lateral arthroscopic portal. (B) Tendon loaded on eyelet needle (red arrow) for passage of the graft traction suture (red dotted arrow) and tendon (blue arrow) through distal fibula. (C) Tendon with traction suture at both ends. Middle part of tendon is inside distal fibular tunnel. (D) Clamp 2 guides clamp 1 through the subcutaneous tunnel. Then clamp 1 holds traction suture and leads tendon through tunnel to talar neck. Blue arrow points the guide pin at talar neck. (E, F) Fluoroscopy of guide pin at talar neck before drilling to ensure proper placement. (G) Interference screw was used to fix one end of tendon to the talus to reconstruct ATFL. (H) The other end of tendon was introduced into body of calcaneus (red arrow). Blue arrow points the guide pin at calcaneus. Numbers 1-4 indicate the 4 small incisions needed for this minimally invasive procedure. (I) The foot was held slightly everted while inserting the interference screw into the calcaneus to keep the tension on lateral ligament. Number 1 is the traction suture through the talus, and number 2 is the traction suture through the calcaneus.
Rehabilitation Protocol
Postoperatively the patient was immobilized in a splint in a slightly everted position for 2 weeks non-weight-bearing, and then allowed to partially bear weight in a walker boot for a further 4 weeks. A period of rehabilitation was required after this immobilization. The patients ambulated in a walker boot full weight-bearing for another 4 weeks. The patients were weaned out of the boot after 10 weeks and were allowed to jog after 12 weeks.
Clinical Evaluation
All patients were evaluated from both the clinical and radiographic perspective. The American Orthopaedic Foot and Ankle Society–Ankle and Hindfoot (AOFAS-AH) questionnaires were completed before surgery and at last follow-up. Patient satisfaction level with the overall outcome was graded as excellent, good, fair, or poor. Donor site morbidity was assessed by subjective feeling of the donor site area, knee movement, and strength. Preoperative and postoperative stress radiographs were taken using a TELOS stress device (TELOS, METAX, Germany) as described by Karlsson. 8 The pressure load applied was 150N. Radiographic parameters included the anterior talar displacement and varus talar tilt.
Statistical Methods
Statistical analysis was performed using SPSS 16.0 (SPSS Inc, Chicago, IL). Wilcoxon signed-rank test was conducted for evaluation of changes in the AOFAS score and radiographic parameters before and after surgery. P values less than .05 were considered to be statistically significant.
Results
The mean AOFAS-AH score increased from 71.1 to 95.1 (P < .001). Two patients reported residual instability on uneven ground. Significant improvement in radiographic parameters was noted for the talar tilt angle, which decreased from a mean of 14.0 to 3.8 degrees (P < .001); the anterior talar displacement reduced from a mean of 12.3 to 4.6 mm (P < .001; Table 1). No patient reported weakness or disability from the donor site. The satisfaction level was excellent in 20 patients and good in 5 patients.
Comparison of American Orthopaedic Foot and Ankle Society–Ankle and Hindfoot (AOFAS-AH) Score and Radiographic Parameters (M ± STD).
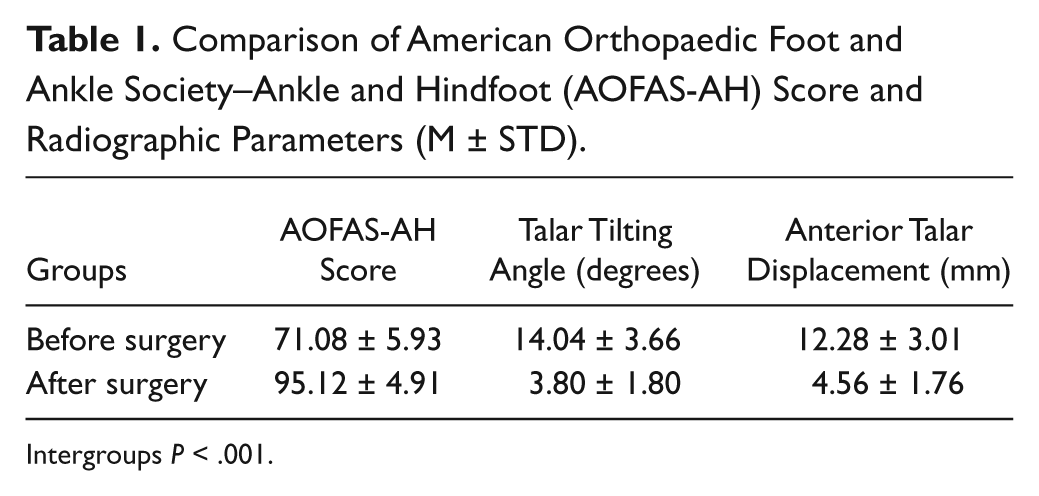
Intergroups P < .001.
Discussion
In this series, our patients preoperatively met at least 1 of the following criteria: repetitive ankle sprains, severe ankle instability (more than 10 degrees of talar tilt angle or more than 10 mm of anterior drawer distance), a previously failed Brostrom procedure with a Gould modification, and/or obesity (more than 25 BMI). The patients achieved both functional and mechanical stability and rapid recovery after lateral ankle reconstruction using a semitendinosus tendon autograft placed using a minimally invasive technique. Only 2 patients reported a residual feeling of instability on uneven ground, which may have been due to combined medial instability. But they thought it was much better than before surgery. This study supports the effectiveness of this approach in this group of patients with severe instability. The minimally invasive augmented repair described in this study may have appeal in clinical situations where the local tissue is insufficient for repair. At the same time, attention should be paid to checking and addressing the medial ligament injury, if present.
For acute tears of the lateral ligaments of the ankle, conservative functional treatment is generally the treatment of choice. Should chronic instability develop, a surgical procedure may be considered.3,4 One can group the procedures into anatomic repair and augmented reconstruction. Anatomic repairs are the most straightforward and involve using the injured ligaments to reconstitute the new lateral stabilizing complex, with a success rate of 88% to 95%. 2 The Brostrom procedure with a Gould modification uses the remaining ATFL and CFL augmented by local extensor retinaculum, allowing restoration of stability. 6 The use of anatomic repairs is limited to patients with local tissues durable enough for repair. Recurrent ankle sprains and multiple previous procedures will often leave local tissues insufficient to perform their role as a restraint to inversion/internal rotation. Contraindications to anatomic repair may include long standing ankle instability, high athletic patient demands, revision surgery, generalized ligamentous laxity, unfavorable patient habitus, and cosmetic consideration of surgical scars. 4 Under these circumstances, an augmented reconstruction may be the technique of choice.
Augmented reconstructions include nonanatomic and anatomic reconstruction. Nonanatomic includes Chrisman-Snook, Evans, and Watson-Jones tenodesis procedures, requiring the harvesting of the peroneus brevis tendon, either whole or in part. Suboptimal results include persistent instability, decreased range of motion, and a low rate of return to full activities after nonanatomic reconstructions.7,11,13 From a biomechanical perspective, the nonanatomic reconstructions reduce subtalar motion, and do not restore proper ankle mechanics. In the short term, this manifests as stiffness, and longitudinal studies have demonstrated tibiotalar osteoarthritis in 19% to 28% of patients. 12 There are also reports of excellent results using peroneus brevis augmentation without sacrificing any eversion strength. Girard et al used a modified Brostrom technique augmented with a portion of the peroneus brevis tendon to restore ankle stability. The isometric eversion strength was measured using a Cybex 340 Isokinetic device, and functional testing, using a lateral lunge test, revealed no significant loss of peroneal strength. The authors concluded that chronic lateral ankle instability in the general population can be successfully managed with a modified Brostrom procedure augmented with a portion of the peroneus brevis. 5
Anatomic reconstruction using various graft choices produces a lower rate of recurrent instability with improved patient outcomes over nonanatomic reconstruction. Choices for grafts have included semitendinosus, gracilis, plantaris, palmaris, fascia lata, bone-patellar tendon, and allografts.4,14 Coughlin et al achieved excellent results by using plantaris and gracilis graft for lateral ankle reconstruction.3,4 Graft choice must take into account any associated harvest site morbidity. We prefer the use of semitendinosus tendon with a minimally invasive method for the following advantages. The semitendinosus tendon autograft is easy to harvest. In addition, it is long and strong enough for simultaneous reconstruction of the ATFL and CFL. It is also inexpensive and leads to minimal tissue reaction compared to allograft. The extensive application of semitendinosus tendon in anterior cruciate ligament repair of the knee has demonstrated minimal donor site morbidity.1,10 The 4 small incisions, less than 1 cm each, and limited exposure reduce the likelihood of damage to branches of the superficial peroneal nerve. The small incisions also have cosmetic appeal to many young patients. In contrast, the incision for harvesting the peroneus brevis tendon is long, and the larger exposure may lead to potential problems with wound healing and a higher risk of nerve injury, fibrosis, and stiffness. If the peroneal tendons are left intact, eversion strength should be unaffected by the procedure, and consequently functional as well as static stability should be optimized.
The use of interference screw technology allows the surgeon to modulate the tension of each ligament independently. This is advantageous because isometric tension of each ligament can be realized. It is important that ligaments are taut during the end of normal excursion of the respective joint it stabilizes.
Conclusion
There are many techniques to address lateral ankle instability. For the treatment of chronic ankle instability requiring augmentation of the local tissue, we found good outcomes with a new minimally invasive reconstruction of the lateral ligaments using a semitendinosus autograft to achieve a stable ankle.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.