
Abstract
Background:
Tibiotalocalcaneal arthrodesis is a salvage option for severe ankle and hindfoot deformities, arthritis of the ankle and subtalar joints, avascular necrosis of the talus, failed total ankle arthroplasty, and Charcot arthropathy. This multicenter study reports clinical experience with the hindfoot arthrodesis nail (HAN) in the treatment of patients with severe ankle and foot abnormalities.
Methods:
Seven participating clinics from Europe and North America recruited 38 patients who underwent ankle/subtalar arthrodesis using retrograde nailing with the HAN. Information was collected regarding technical details, complications, and functional and quality of life outcomes (Short Form-36 [SF-36], American Academy of Orthopaedic Surgeons—Foot and Ankle Outcomes [AAOS-FAO], and numeric rating scale [NRS] for pain) after an average of 2 years of follow-up.
Results:
The rate of superficial wound infection was 2.4%. No deep soft tissue or bone infections were reported. The overall union rate was 84%. At the time of follow-up, low pain levels were reported, with a mean NRS of 2.2; the mean AAOS-FAO score was 38; and the SF-36 mean physical and mental health component scores were 41.2 and 52.5, respectively. All 13 patients who were unable to work prior to surgery were able to fully return to work.
Conclusions:
The HAN offered a safe and reliable salvage option for tibiotalocalcaneal arthrodesis in patients with severe ankle and hindfoot disease. It achieved acceptable functional outcome and low complication rates despite the challenging patient cohort. A considerable socioeconomic benefit appeared to result based on the high proportion of patients who were able to return to work postoperatively.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Tibiotalocalcaneal arthrodesis results in a completely stiff ankle and hindfoot, considerably limiting global foot function. It is therefore reserved as a salvage option in cases of severe malfunction and arthritis at both the ankle and subtalar joints and in otherwise intractable deformities in rheumatoid arthritis, Charcot arthropathy, or paresis. Loss of the talus after trauma, infection, tumor resection, or a failed total ankle replacement requires either direct tibiocalcaneal arthrodesis or the interposition of a structural bone graft.12,21,31 The aim of tibiotalocalcaneal fusion is elimination of pain and instability with the creation of a stable, plantigrade foot for ambulation.
In 1906, Lexer 20 reported on several cases in which the fibula of the same patient or cooked autograft fibula was used as a strut graft to achieve tibiotalocalcaneal fusion in paralytic joints. The grafts were introduced like a nail in a retrograde fashion from the calcaneus through the talus into the distal tibia. 20 Tibiotalocalcaneal and tibiocalcaneal fusion have been achieved with multiple screws5,27,40 and by external fixation alone14,30 or supplemented by intramedullary pins 34 or screws, 26 intramedullary nails,8,16 and anterior32,41 and posterior plates.1,2,11
The use of a retrograde intramedullary nail was first described by Gerhard Küntscher 19 in 1967 and offered a stable construct with a load-sharing device and broad, intrinsically stable cortical contact. The use of straight nails is associated with the potential risk of injury to the lateral plantar artery and nerve, cortical hypertrophy or stress fractures at the tibia, and plantar breakout because of poor cortical anchorage in the medial part of the calcaneus.16,22,28,36 The entry point for straight nails lies on the medial edge of the anterior process of the calcaneus, which has a physiological valgus of about 12 degrees with respect to the tibia. Therefore, less bone anchorage is offered by straight nails compared with their curved counterparts, which are introduced along the calcaneal axis. Introducing straight nails may also lead to increased stress at the tip of the nail and residual hindfoot varus. To avoid these problems, several curved nail designs have been investigated,8,10 and previous studies with a curved nail design have reported promising results.3,24
The aim of this study was to examine the clinical experience with a curved nail design and various locking options in the tibia, talus, and calcaneus of the hindfoot arthrodesis nail (HAN; Synthes AG, Bettlach, Switzerland) by different surgeons as well as to document the functional and quality of life outcomes for patients treated with HAN for severe ankle and foot abnormalities.
Methods
A multicenter case series was conducted involving retrospective baseline data acquisition and prospective functional and quality of life outcome assessment of patients with diseases affecting both the ankle and hindfoot after failed nonoperative or previous operative treatment. Seven participating clinics including 4 European sites and 3 US-based hospitals were involved, and approval of the respective ethics committees was obtained for all centers. Between December 2009 and March 2011, 38 patients who underwent ankle arthrodesis using HAN more than 12 months prior to entering the study, who were at least 18 years of age, and who provided informed consent to participate in the follow-up evaluation surveys were included. There were no restrictions regarding the inclusion of patients based on the cause of their underlying ankle and hindfoot disease. For the prospective part of the study, eligible patients were contacted either by telephone or by mail to ask whether they would participate in the study; 26 patients contacted by phone provided their oral consent and participated in the telephone interview to assess their functional outcome and quality of life status. The remaining patients (n = 12) were able to sign and complete a written informed consent form and the outcome/status questionnaires and return them by mail.
Patient Characteristics
The study included an equal number of men (n = 19) and women (n = 19), who had a mean age of 53 years (range, 27-81 years) (Table 1). Two-thirds (66%) were nonsmokers, half were employed, and only 2 patients were living at home with required caregiver support. As a result of their ankle or foot condition, 13 patients (34%) were on sick leave for a minimum of 48 days up to a maximum of 635 days (Table 1).
Sociodemographic Characteristics of the HAN Study Population.
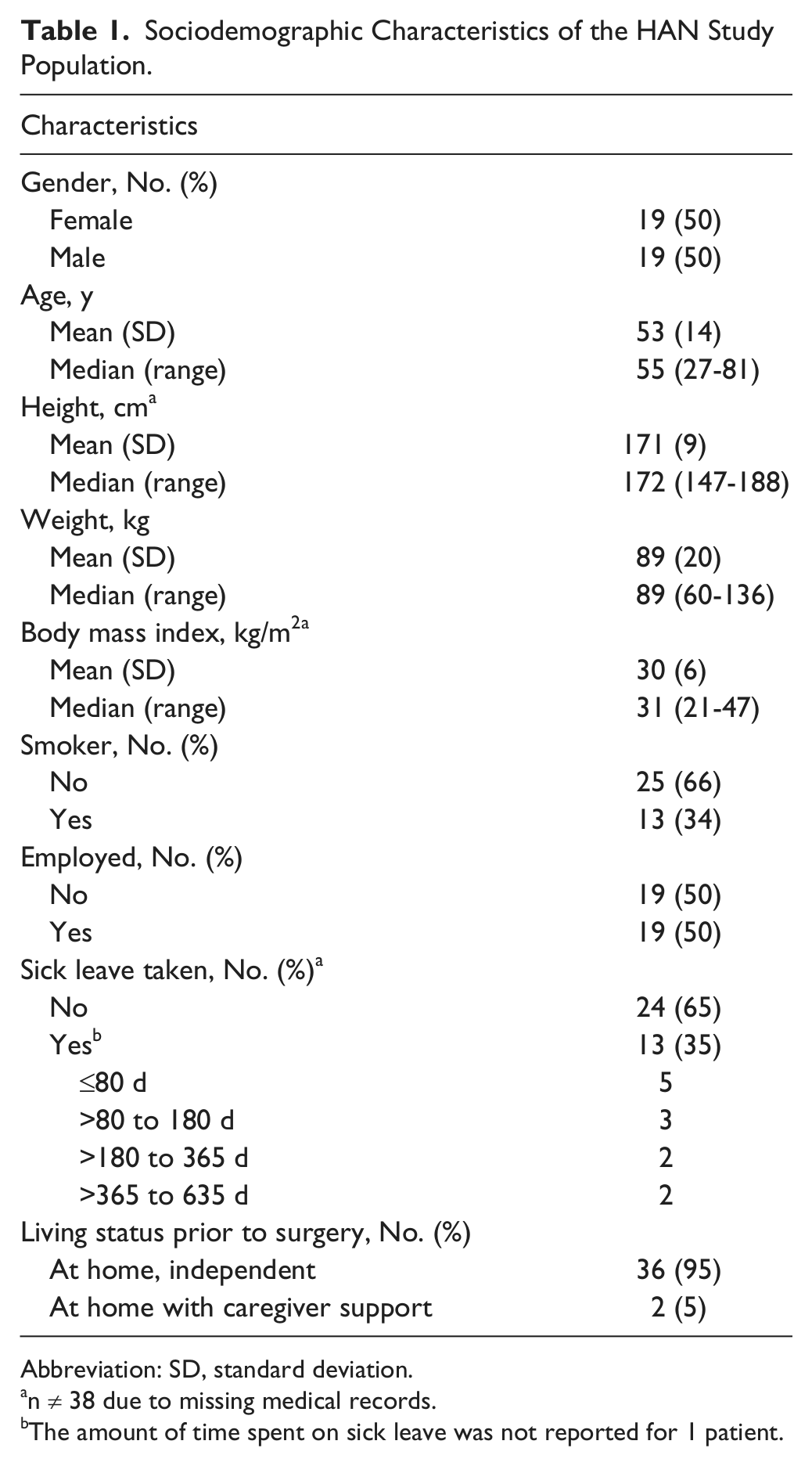
Abbreviation: SD, standard deviation.
n ≠ 38 due to missing medical records.
The amount of time spent on sick leave was not reported for 1 patient.
Ten patients (26%) were diabetic, 2 patients (5%) had a history of alcohol abuse, and almost half (n = 17) were taking continuous pain medication for their condition. Of these 17, 15 were taking nonsteroidal anti-inflammatory drugs, 5 were taking aspirin, and a single patient was undergoing systemic glucocorticoid therapy. Thirteen patients (34%) were smokers. Only 7 patients (18%) were still involved in recreational activities such as walking prior to surgery.
Nonunion (32%) after previous surgery was the most common indication for HAN implantation, followed by arthritis of the ankle and subtalar joints (18%), severe ankle/foot deformity (16%), Charcot foot (13%), and failed total ankle replacement (13%) (Table 2). Eight patients had other pathological ankle and hindfoot conditions, including single cases of a calcaneus fracture; gross lateral varus instability of the lower leg; Charcot-Marie-Tooth disease; idiopathic arthritis; 2 cases of infected hindfoot nonunion; and malunions after talus and ankle fractures. Sixty-six percent (25/38) of the patients had undergone an earlier operative procedure for their affected leg, which involved osteosynthesis of a pilon, calcaneal or talar fracture (n = 15), total ankle replacement (n = 5), or ankle fusion (n = 5).
Patient Characteristics.
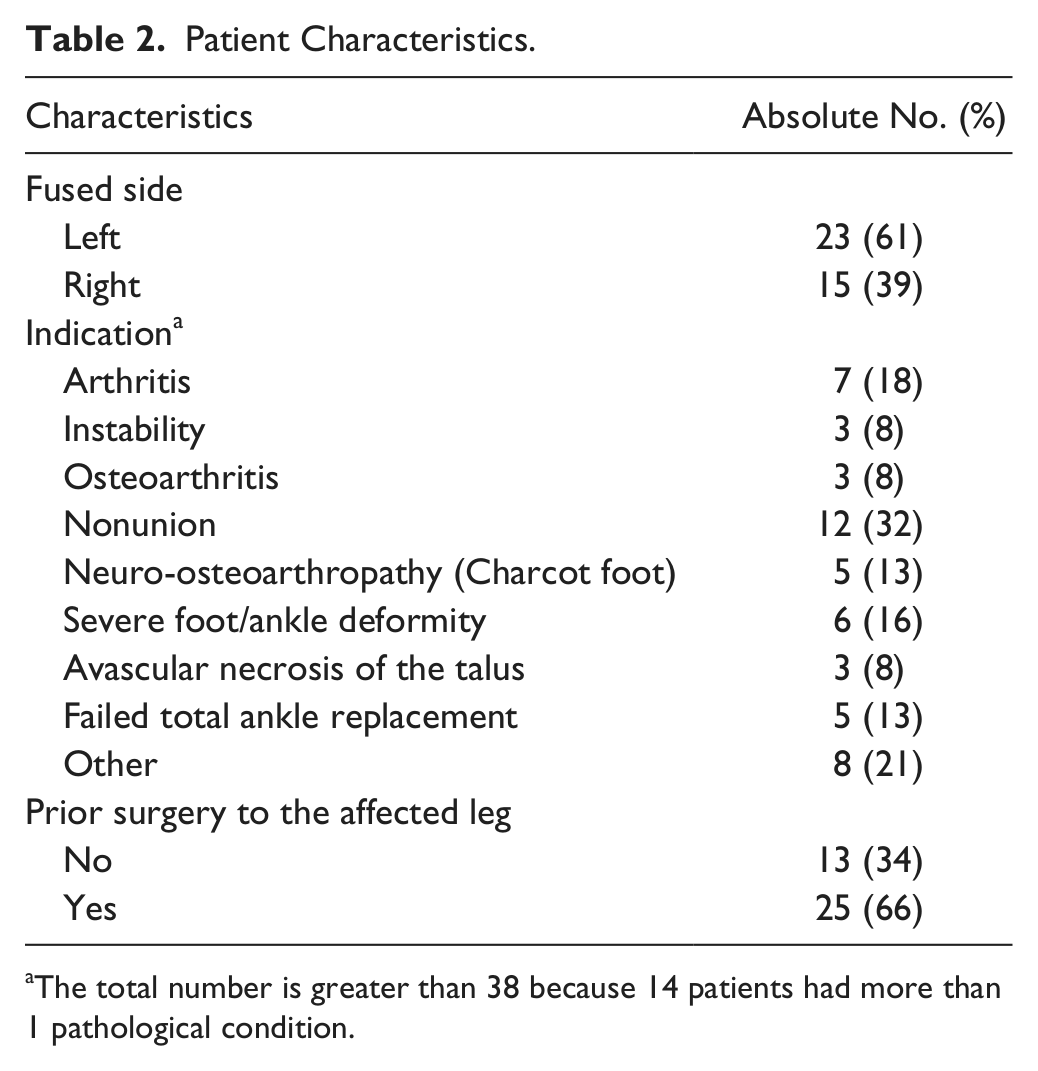
The total number is greater than 38 because 14 patients had more than 1 pathological condition.
Surgical Procedure
Arthrodesis was performed using the titanium cannulated HAN. The nail has a diameter of 10, 12, or 13 mm; a length of 150, 180, or 240 mm; and a curvature of 12 degrees in the frontal plane in order to match the physiological hindfoot axis in relation to the lower leg.
The patient was placed in either a prone or a supine position at the discretion of the treating surgeon. An anterior approach to the ankle joint in combination with a lateral approach (curved or oblique) to the subtalar joint was used in 30 cases, and a lateral transfibular approach was used in 8 cases. Fibulectomy was performed 6 times. The ankle and subtalar joints were debrided completely of remaining cartilage and all sclerotic or necrotic bone. The foot was brought into neutral alignment with respect to the lower leg and secured with a Kirschner wire. A Steinmann pin was then introduced as a guide wire under fluoroscopic control parallel to the lateral border of the calcaneus in the anteroposterior view and centered on the tibial axis in the lateral view via a plantar stab incision (Figure 1). The pin was introduced in a retrograde manner into the calcaneus and talus up to the level of the ankle joint and overdrilled. The transfixing K-wire was then removed, the heel was brought into varus, and the guide wire was advanced centrally into the distal tibial metaphysis and diaphysis. Care was taken to avoid anterior-posterior translation and to maintain a plantigrade position of the foot. After overdrilling, the nail was inserted, bringing the heel back into the physiological valgus position. Locking options included a spiral blade and/or screws inserted from the posterior into the calcaneus, 1 screw inserted from the posterior into the talus, and static and dynamic locking screws inserted from the medial into the distal tibia. No specific compression method was used, but with the dynamic locking option, dynamic compression with weight-bearing could be achieved. Bone graft was used in 11 cases without extenders to fill defects that resulted from resection of infected, sclerotic, and/or necrotic bone. Correct hindfoot alignment was controlled clinically and with intraoperative fluoroscopy.

(a) Case example of severe ankle and subtalar arthritis after a malunited malleolar fracture with subsequent infection leading to partial necrosis of the talar dome and the distal fibula. (b) After debridement of all necrotic bone, the ankle and hindfoot were brought into neutral position and fixed temporarily with a K-wire. The guide wire for the retrograde nail (dotted line) was introduced along the calcaneal axis in the frontal plane to achieve its physiological valgus position and centered beneath the tibia in the sagittal plane. (c) Radiographs at follow-up show solid fusion with correct axial alignment. (d) Computed tomography at follow-up shows the position of the nail within the calcaneus, talus, and tibia.
All factors associated with the operative procedure were documented including the experience level of the surgeon, the technique used to determine the nail length, the total time for the surgery as well as radiographic control, implant details (ie, nail length and diameter, type of locking), and any intraoperative complications (eg, iatrogenic fracture, malpositioning of the nail or locking bolts).
Follow-Up Evaluation
Standard radiographs documenting anatomical alignment of the ankle and hindfoot were obtained in the immediate postoperative period. In addition, weight-bearing status, length of hospital stay, the patient’s living status, and any early postoperative complications (eg, implant or implant component breakage, disassembly, loosening, or migration; wound infection; or secondary intervention) prior to hospital discharge were documented.
Follow-up examination data were obtained by the treating surgeons after a mean period of 23.6 months (range, 3.7-39.3 months) and included information regarding final weight-bearing status, the occurrence of postoperative complications (ie, implant failure, nonunion, infection) since the operative procedure, and any reports of implant removal, dynamization, amputation, and revision surgery. Solid fusion was verified by obliteration of the joint space and trabecular continuity from the tibia to the talus on lateral and anteroposterior weight-bearing radiographs of the ankle at 3 months after surgery. Nonunion was defined as radiographic evidence of incomplete fusion more than 9 months after surgery.
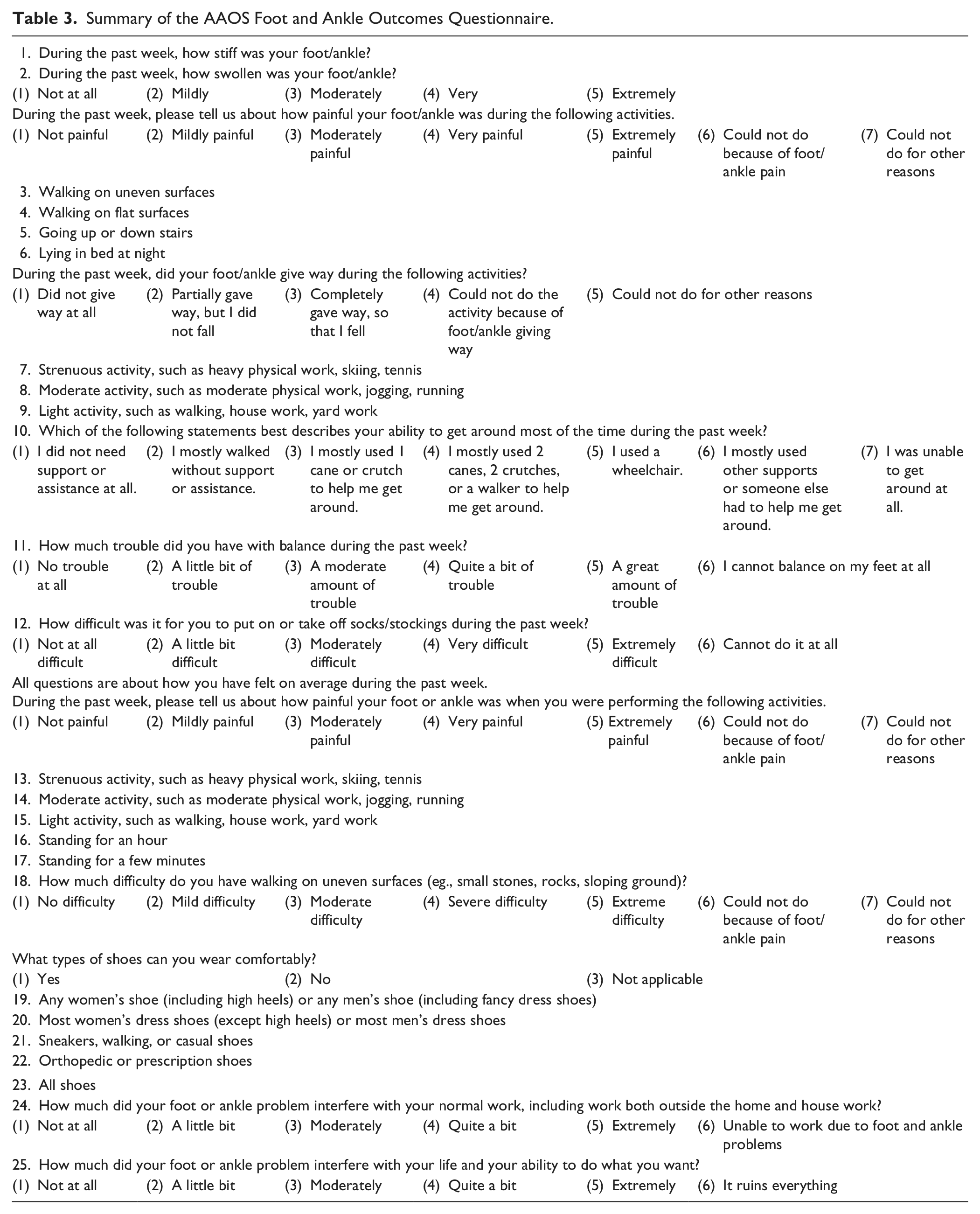
Each patient was asked to assess his or her functional outcome and quality of life status using the American Academy of Orthopaedic Surgeons—Foot and Ankle Outcomes (AAOS-FAO) 13 and Short Form-36 (SF-36) 38 questionnaires, respectively. The AAOS-FAO (Table 3) assesses functional outcome based on the patient’s subjective evaluation and consists of 4 subscales of pain, function, stiffness/swelling, and giving way. The final standardized score ranged from 0 to 100 points, with the lower the score, the greater the disability. Furthermore, normative scores of the AAOS-FAO were calculated from the standardized values as outlined by AAOS (http://www.aaos.org/research/outcomes/outcomes_documentation.asp#refs) based on the general US reference population (normative mean, 50 points; standard deviation, 10), where a patient scoring above 50 was above the general population’s average, and a patient scoring below 50 on a scale was below the general, healthy population’s norm. A maximum of 30 points was specifically allocated to the “function” subscale, which was focused on the patient’s difficulty with getting around, balance, putting on socks or stockings, walking on uneven surfaces, and normal work and life activities.
Summary of the AAOS Foot and Ankle Outcomes Questionnaire.
The SF-36 patient-rated health status instrument assessed quality of life based on the 4-week recall period. All items were scored and summed, and the resulting scale score was then transformed linearly to a value ranging from 0 (poorest health) to 100 (best health). Scores for the mental and physical component summary measures were generated as described in the SF-36 manual using norm-based scores. 38 Summary component scores were directly compared with the US reference population (mean, 50 points; standard deviation, 10 points), where values above and below 50 represent those above and below the average reference population, respectively. In addition to completing the SF-36 and AAOS-FAO questionnaires, patients were asked about their current employment and living status as well as whether they had taken sick leave and/or had undergone any additional foot surgery since the index procedure. The degree of pain was also assessed using the 0 to 10 numeric rating scale (NRS) 7 where 0 indicated “no pain” and 10 represented “worst possible pain.” The average follow-up time between the surgery and completion of the patient surveys was 24.7 months (range, 11.3-41.4 months).
Statistical Analysis
All analyses were performed using Intercooled Stata Version 11 (StataCorp LP, College Station, TX). Based on the observational nature of this study, all analyses were made in a descriptive, nonconfirmatory, hypothesis-generating manner using standard descriptive statistics. SF-36 physical and mental composite scores were computed using the US population-based norms. Complication risks were calculated for each class and type by dividing the number of patients having experienced a complication over the total number of enrolled patients treated with HAN. Statistical inferences were made by reporting exact-binomial 95% confidence intervals for complication risks.
Results
The majority of HAN operations were undertaken by experienced consultants (47%) or chief surgeons (37%) who most often used the preoperative technique using a template on both ankles to determine the nail length. The total mean operative time was 168 minutes (range, 86-333 minutes).
The HAN with a length of 180 mm (53%) and diameter of 10 mm (50%) was most commonly used for about half of the surgeries. Proximal locking screws were most frequently applied to both the static locking hole (84%) and dynamic slot (83%), whereas fewer than 50% of the nails were locked distally using the talar-navicular hole and a posterior-anterior locking screw. The spiral blade was used for 66% of the patients in conjunction with an end cap (61%) inserted on the nail end.
Two patients (5%) had an iatrogenic fracture that occurred during surgery. For 1 of these patients, a technical problem was also reported and replacement of the original HAN implant was required.
Anatomical alignment was achieved by the majority (92%; 35/38) of patients. For the remaining 3 patients, valgus deviations of 8 and 10 degrees and a single varus deviation of 6 degrees were measured on the immediate postoperative radiographs.
Of the 37 patients with available baseline weight-bearing data immediately after surgery, 15 patients could not bear weight but were able to be mobilized out of bed, 18 were able to bear partial weight up to 30 pounds, 2 could bear weight up to 60 pounds, and another 2 patients could bear weight soon after surgery. A removable splint was applied postoperatively and exchanged for a cast after wound healing, usually between 10 and 14 days after surgery. By the final follow-up evaluation, the majority of patients (92%; 35/38) achieved full weight-bearing.
The mean length of time spent as an inpatient was 8.4 days (range, 2-36 days) with the majority (92%) of HAN patients being discharged within 2 weeks after the operative procedure. Only 4 patients required intensive care unit treatment for a minimum of 4 days and up to a maximum period of 8 days. The in-hospital times were influenced by comorbidities of the patients and partly reflect the current practice at the participating centers in Europe.
After hospital discharge, 26 patients (68%) returned to their home and were considered independent as they did not require any caregiver support, whereas 8 patients (21%) did require aid in their activities of daily living. The remaining 3 patients (8%) entered either a nursing home or rehabilitation facility, and for the last case, no further information was available.
Complications
Nine patients (24%) experienced at least 1 complication between the immediate postoperative period and final follow-up (Table 4). A total of 6 patients with nonunion (16%) were documented for the entire patient cohort. The union rate did not appear to be affected by smoking. One nonunion patient underwent 2 unplanned secondary operations; the first intervention involved resection of necrotic tissue and bone graft transplantation without nail removal, and in the second procedure the nail was removed followed by bone graft and osteosynthesis with a tibial nail introduced in a retrograde manner 14 months later. Four additional patients also required revision surgery for nonunion. The HAN implant was completely removed followed by osteosynthesis and bone graft in 1 patient. The second patient underwent talonavicular fusion with a bone graft and screws 8 months after HAN implantation. The third patient received a bone graft and additional screw fixation of the fibula, and the fourth patient underwent a second operation 12 months after the primary procedure that involved bone grafting and a Dwyer osteotomy of the calcaneus to correct varus malalignment as well as exchanging the HAN spiral blade for a more proximal locking screw. Another patient experienced a nonunion associated with a series of complications including a systemic and localized infection and a disassembly-related complication. The patient underwent a 2-stage procedure involving (1) removal of an intramedullary nail and broken plate followed by application of a spacer containing bone cement and gentamycin; and (2) reimplantation of the HAN with bone grafting 2 months later. The latter, however, resulted in persistent nonunion that required another bone grafting procedure and addition of a lateral plate to provide further stability 9 months after the primary HAN operation.
Postoperative Complications Reported for the HAN Study Population.
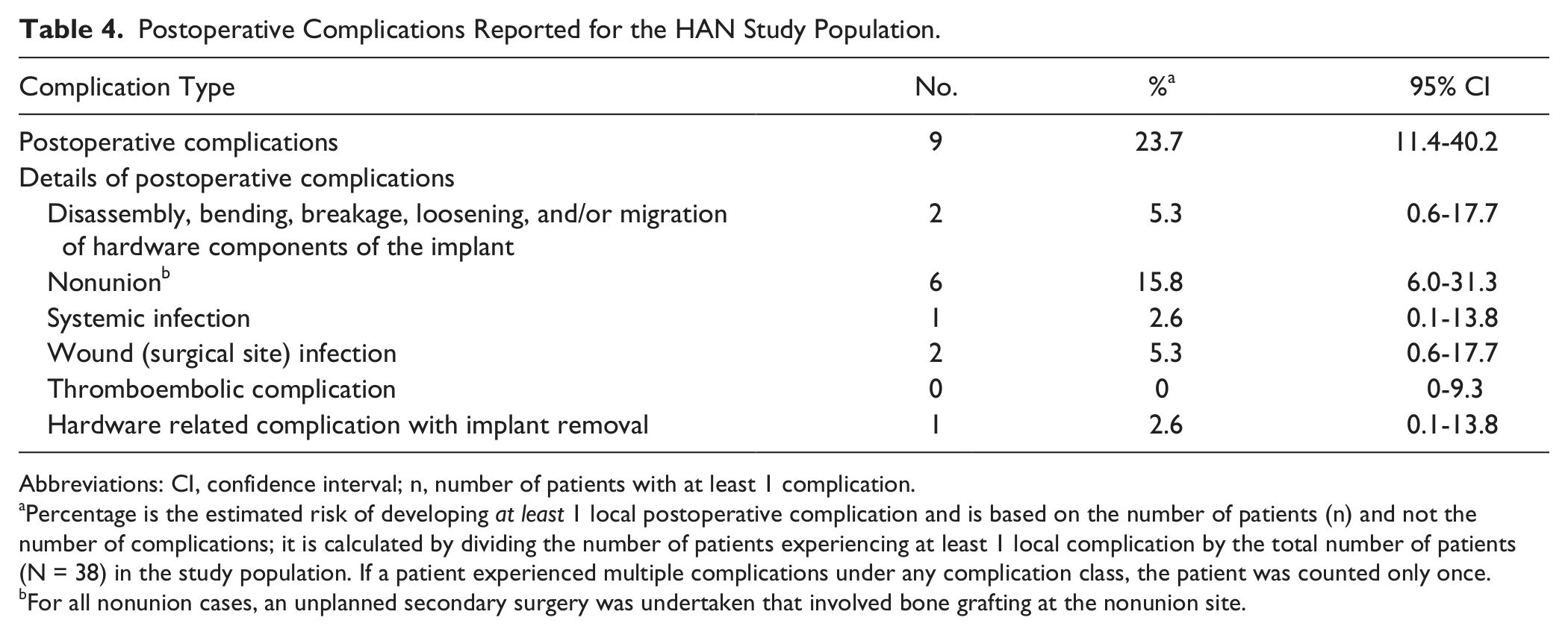
Abbreviations: CI, confidence interval; n, number of patients with at least 1 complication.
Percentage is the estimated risk of developing at least 1 local postoperative complication and is based on the number of patients (n) and not the number of complications; it is calculated by dividing the number of patients experiencing at least 1 local complication by the total number of patients (N = 38) in the study population. If a patient experienced multiple complications under any complication class, the patient was counted only once.
For all nonunion cases, an unplanned secondary surgery was undertaken that involved bone grafting at the nonunion site.
Two patients experienced a single implant-related complication. A combination of spiral blade and screw was used for distal locking in 1 patient; the screw broke after completion of the surgery. For the second patient, the reported hardware-related complication stemmed from screws that were intended to provide compression and additional stability to the fibula. Because the patient complained of local soft tissue irritation, these screws were removed.
One patient had a small wound dehiscence at the anterior approach 2 months after surgery. There was no severe bone infection or material involvement, so the local infection was treated by antiseptic wound dressing until complete wound healing was obtained. This patient together with the patient described above who had experienced a local infection provided an overall rate of superficial and deep infections of 5.3%.
The risk of experiencing at least 1 postoperative complication after HAN surgery was 24% (95% confidence interval, 11.4%-40.2%), with nonunion being the most common postoperative complication (16%) (Table 4).
Follow-Up Outcomes
At the time of follow-up evaluation, 15 of the 19 initially employed patients retained their working status, 3 became unemployed, and the last patient retired after the foot surgery. The 19 patients who were either unemployed or retired before their surgery remained as such, except for 1 patient who found work during the follow-up period.
All 13 patients who were previously on sick leave were no longer taking time off because of their condition; 1 patient who had not previously taken sick leave reported that he had taken 400 days of sick leave during the follow-up period.
In the follow-up assessment, 4 patients indicated that their living status had changed from being independent at home to being at home with support provided by a caregiver since the surgery.
The mean SF-36 physical and mental health component summary scores for the whole patient cohort were 41.2 points (range, 19.5-64.3 points) and 52.5 points (range, 26.0-70.2 points), respectively (Figure 2). The median normative AAOS-FAO score was 37.8 points (range, –14.1 to 54.7 points). The mean level of pain rated by HAN patients was 2.2 (range, 0-9) on the NRS, with 61% (23/38) having minimal to no pain (NRS = 0-2); only 1 patient experienced an almost maximum degree of pain (NRS = 9) at the follow-up evaluation (Figure 3).
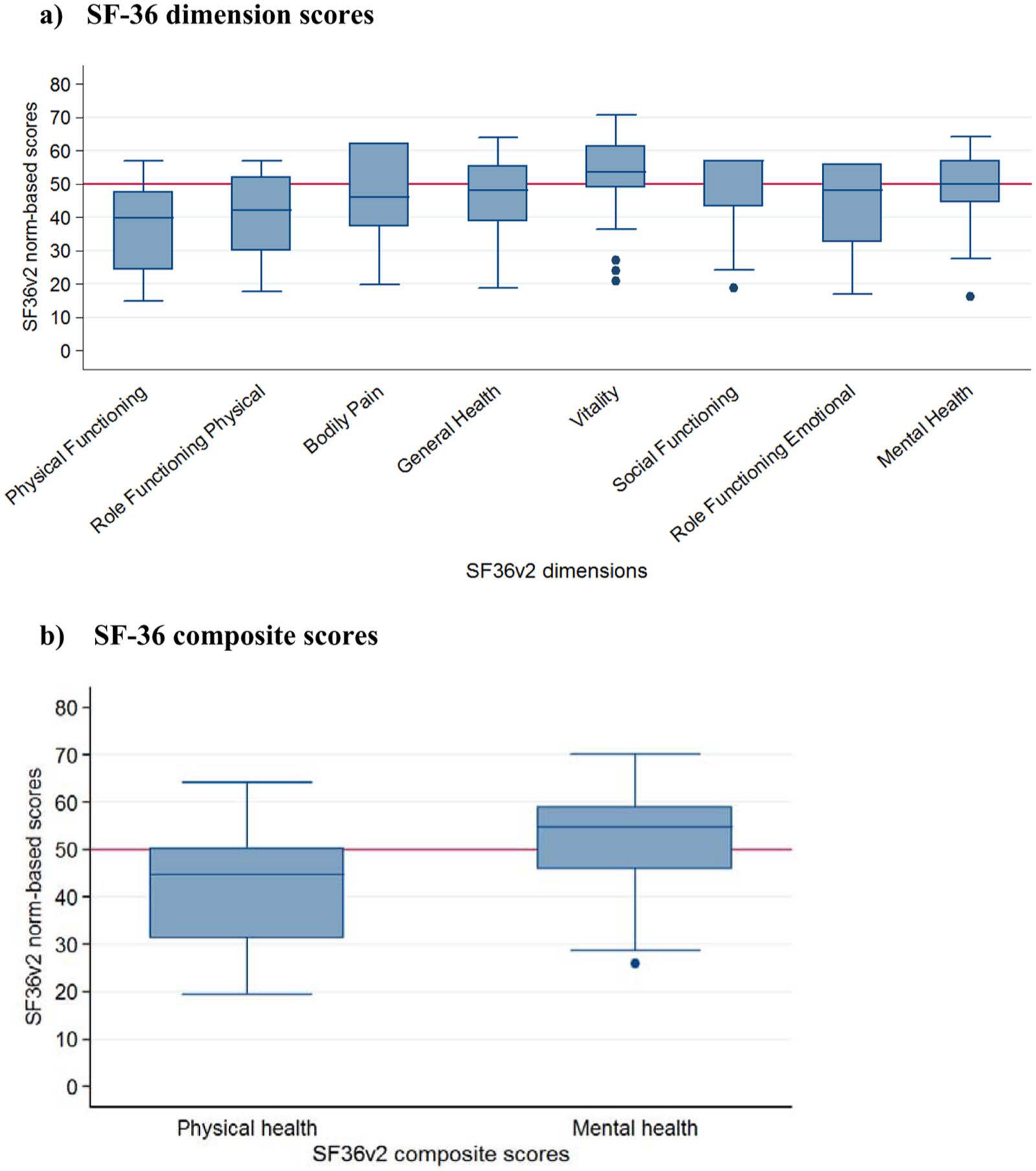
Box plots representing the final SF-36 quality of life status. The ends of each rectangle correspond to the upper and lower quartiles. The line drawn through the rectangle corresponds to the median value. The whiskers, starting at the ends of the rectangle (or points representing extreme values), indicate minimum and maximum values. The mean SF-36 individual dimension and composite scores showed that the HAN study population achieved a moderate level of health at the final follow-up examination.
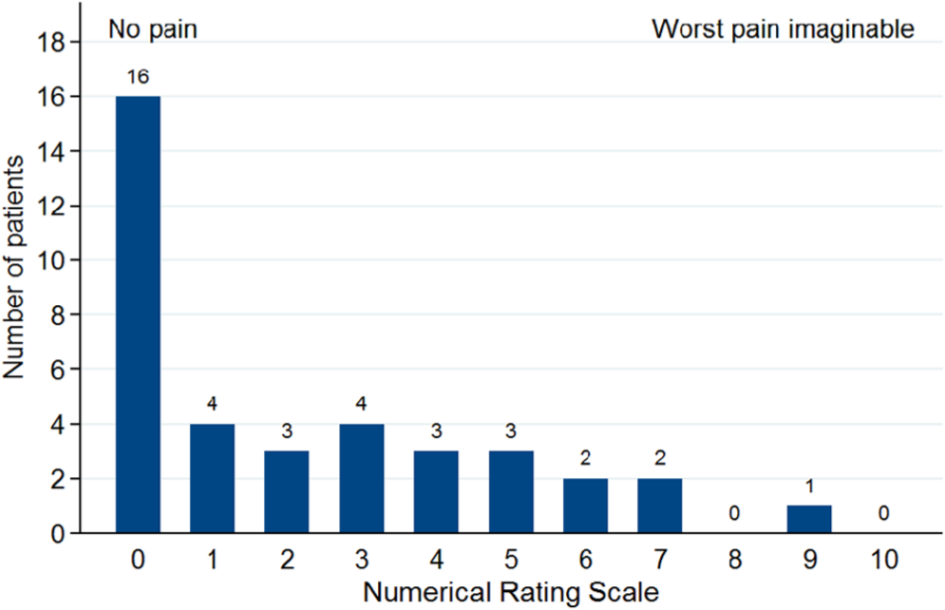
Distribution of HAN patients according to the degree of pain as measured using the 0-10 numeric rating scale at their final follow-up examination.
Discussion
The present study summarizes the experience of several surgeons from Europe and North America who used the HAN. The fusion rate was 84%, the rate of superficial wound infections was 5.3%, and no deep infection or osteomyelitis was reported. Our patients with severe ankle and hindfoot conditions were therefore adequately treated using this implant and usually achieved union with low pain levels at the mean follow-up of 2 years, even though the final SF-36 physical and mental health component summary scores reflected some remaining impairment of a combined ankle and subtalar fusion.
Hindfoot fusion remains a salvage option for severe ankle and hindfoot conditions that cannot be addressed sufficiently with other measures. 31 A comparison among different published studies is problematic because of the heterogeneous patient cohorts and different outcome measurements used. Despite its lack of validation, the American Orthopaedic Foot & Ankle Society (AOFAS) ankle/hindfoot scale is still the most widely used score and allows some comparison between the various studies. The mean AOFAS score after tibiotalocalcaneal arthrodesis in previous studies has ranged from 54 to 80 points, which corresponds to a good to fair result.5,9,24,33,37 Union rates after hindfoot fusion range between 65% and 100%.3,6,8,9,14,15,23,24,27,35,37 Despite the sometimes critical preoperative conditions and severe deformities, the infection rates with retrograde nailing of the hindfoot are lower than 10%.5,17,21,23 The results of our current study compare favorably with the literature. A 16% nonunion rate can be considered low for this select group of patients with severe ankle and hindfoot conditions including previous nonunion, Charcot arthropathy, and severe deformities.
From a socioeconomic point, a considerable number of patients (15/19) were able to return to their previous occupation. Furthermore, all 13 patients who were previously on sick leave could return to work. Given the severe nature of the preoperative ankle and hindfoot condition leading to the necessity for a tibiotalocalcaneal fusion, this can be considered a remarkable result.
Special features of the HAN are the 12-degree angulation that corresponds to the physiological hindfoot valgus with respect to the tibia and the different locking options in the tibia, talus, and calcaneus. The latter includes locking screws, a spiral blade, and a combination of both that offers the highest stability in biomechanical cadaver studies.4,18 Furthermore, Chiodo et al 4 found the combination of a blade plate and a 6.3-mm lag screw to be more stable than an intramedullary nail with distal locking in a lateral to medial direction. This locking option was shown to be inferior to posteroanterior locking because of the smaller mediolateral diameter of the calcaneus.
The use of straight nails carries a potential risk of injury to the lateral plantar artery and nerve, residual hindfoot varus, cortical hypertrophy, or stress fractures of the tibia.16,22,28,36 Because of the physiological valgus of the calcaneus with respect to the tibia, the entry point for straight nails lies on the medial edge of the anterior process, resulting in less bony anchorage than with curved nails. To avoid these problems, several curved nail designs have been investigated, such as the retrograde distal femoral nail 8 and the ACE nail. 10 Previous studies with a curved nail design have reported high union rates and favorable outcomes.3,24
In the present study, 10 patients (26%) had diabetes mellitus. Diabetes increases the risk of postoperative complications in foot and ankle surgery. 39 Furthermore, the presence of diabetic complications such as nephropathy and neuropathy leading to Charcot arthropathy at the foot and ankle represents a considerable risk factor.26,41 A recent study comparing ankle and hindfoot fusions in 70 diabetic patients versus 74 healthy patients revealed a higher overall rate of complications in the former group, who had an associated history of tobacco use and peripheral neuropathy. 25 The infection rate was significantly increased in the diabetic patients and those with poor long-term glucose control. 25 When hyperglycemia can be controlled and longer healing times are respected, hindfoot fusion with retrograde nailing is a viable alternative to amputation because solid fusion can be attained in these patients. 29 The high fusion rate and the absence of deep infections in a complicated patient cohort as seen in our study support these findings.
There are several limitations of the present study, including the lack of a control group and the relatively low number of patients. However, the patient population that we included lies within the range of recently published studies on hindfoot arthrodesis with other nail designs. Further studies with more patients would allow for a more detailed analysis of prognostic factors. Because of the multicenter study design, the procedures were carried out by several physicians, leading to an inherent heterogeneity of individual implantation techniques. However, this study reflects the reality of surgical care for this particular patient cohort rather than a single surgeon’s experience. The majority of surgeons with a senior consultant level were experienced with tibiotalocalcaneal arthrodesis with other nail designs.
In conclusion, tibiotalocalcaneal fusion with a curved intramedullary nail (HAN) resulted in a high fusion rate, no osseous infections, a low pain level, an adequate quality of life, and a return to work rate comparing favorably with those of previous studies on tibiotalocalcaneal arthrodesis. Retrograde intramedullary nailing with a curved HAN offers a safe and reliable salvage option and a viable alternative to amputation patients with severe ankle and hindfoot deformities.
Footnotes
Acknowledgements
The authors would like to thank Alexander Fuchs, MD (University Hospital Dresden, Germany) for his help in data collection and Melissa Wilhelmi-Mock, PhD (AO Clinical Investigation and Documentation, Dübendorf, Switzerland) for her thorough review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was conducted as a multicenter clinical study by the AO (Arbeitsgemeinschaft für Osteosynthesefragen) Clinical Investigation and Documentation and supported by Synthes. Drs Ågren, Cronier, Hansen, and Sands were involved in the development of the device described in this paper. Dr Fircia receives royalties from Orthohelix and is a consultant for Arthrex. The department of Dr Hartsock receives research grant support from Synthes, Medtronic, Styker, and Globus. He himself does not receive any direct payments or royalties. The other authors do not report any potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.