
Abstract
Background:
Hammertoe and claw toe are among the most common foot deformities. Proximal interphalangeal (PIP) joint realignment can be performed using specifically designed intramedullary implants. The aim of this study was to assess the clinical outcome of patients with lesser toes deformities undergoing PIP joint realignment using an intramedullary implant.
Methods:
Patients requiring PIP joint realignment were included in this prospective multicenter observational study and followed for 12 months. A total of 156 toes, in 117 patients were implanted with the implants. Complications and radiological and functional outcome were assessed.
Results:
The proportion of joints fused on X-rays was 83.8% (95% CI: 77.8, 89.7) after 1 year. American Orthopaedic Foot and Ankle Society lesser metatarsophalangeal-interphalangeal scale (AOFAS-LMIS) improved from 40.4 (SD = 18.3) preoperatively to 85.5 (SD = 9.2) after 1 year. The proportion of patients with pain was 15.5% after 6 weeks and decreased to 4.7% after 1 year. Of the patients, 98% were satisfied about the operation. In patients with incomplete fusion of the PIP joint after 1 year, AOFAS-LMIS improved from 36.7 (SD = 18.9) preoperatively to 84.2 (SD = 10.1) 1 year postoperatively, while pain was reported by 2 patients (8.3%) after 1 year. Toe malalignment and lack of toe pulp-contact were reported slightly more frequently than for the whole group of patients, but not for the majority of the cases. Overall, complications were reported intraoperatively in 1.3% of the patients (2 cases) and postoperatively in 3.2% (5 cases). Revision was required in 1 case. Mallet toe deformity was found in 2.0% of the patients after 1 year.
Conclusion:
This study showed that the use of an intramedullary implant for PIP realignment led to a high rate of fusion and a good outcome. No need of reoperation was reported for patients with incomplete joint fusion who had a stable joint with no pain.
Level of Evidence:
Level IV, prospective case series.
Keywords
Hammertoe and claw toe are among the most common foot deformities. When nonoperative treatments such as toe pads, strapping devices or specific shoes have failed, arthroplasty or arthrodesis of the proximal interphalangeal (PIP) joint is offered to the patients. PIP arthroplasty aims at realigning the joint with a thorough release, which can even be complemented by associating osteotomies of the metatarsal or the proximal phalanx. The result can be fibrous or bony union, with a stable toe, but malalignment, in any 1 of the 3 planes, and recurrence are often a reason for dissatisfaction.2,4 PIP arthrodesis is technically demanding and ideally needs internal fixation, close contact between phalanges, and a physiological plantar flexion angle, to allow pulp-ground contact. Fixation is classically performed using Kirschner wire transfixion. However, complications such as pin tract infection, pain, and discomfort due to the pin can be encountered. As for arthroplasty, malalignment is the major cause of dissatisfaction, together with a “too straight toe” and a distal interphalangeal joint deformity (mallet toe). Some implants have been developed over the past decade including Ipp-On interphalangeal implant, which has hooks at both ends to anchor the implant to the phalanges. The implant is angulated to obtain anatomic plantarflexion of the toe and to maximize the chances of good alignment.
The aim of the current study was to describe the complications and to analyze the radiological and functional outcome in patients who underwent PIP joint realignment using Ipp-On interphalangeal implant and were followed for 1 year.
Methods
This European, multicenter, prospective, observational study included patients who underwent surgery between July 2009 and May 2011, with a 12 month follow-up period that ended in June 2012. Patients included in the study were at least 18 years old and needed a proximal interphalangeal joint realignment. This was carried out with Ipp-On (Integra LifeSciences, Lyon, France; Figure 1). Patients were included in case of a fixed or rigid hammer or claw-toe, with or without an excess of lengthening of the operated toe; in some other cases, it was a revision of a previous arthroplasty (Figure 2). Patients were not included if they had current or past history of local or systemic infection, severe peripheral vascular disease, insufficient quantity or quality of bone to permit stabilization of the arthrodesis, and suspected or documented metal allergy or intolerance. Each patient could be subjected to more than 1 PIP joint arthrodesis during the same or another operation. Patients were recruited by 5 study centers in France, Belgium, and Switzerland. Study documents received institutional review board approval in each country.

Ipp-On intramedullary implant for PIP joint fusion. Proximal end to the right. The distal end is larger and was specifically designed to fix the implant into the cancellous bone of the middle phalanx.
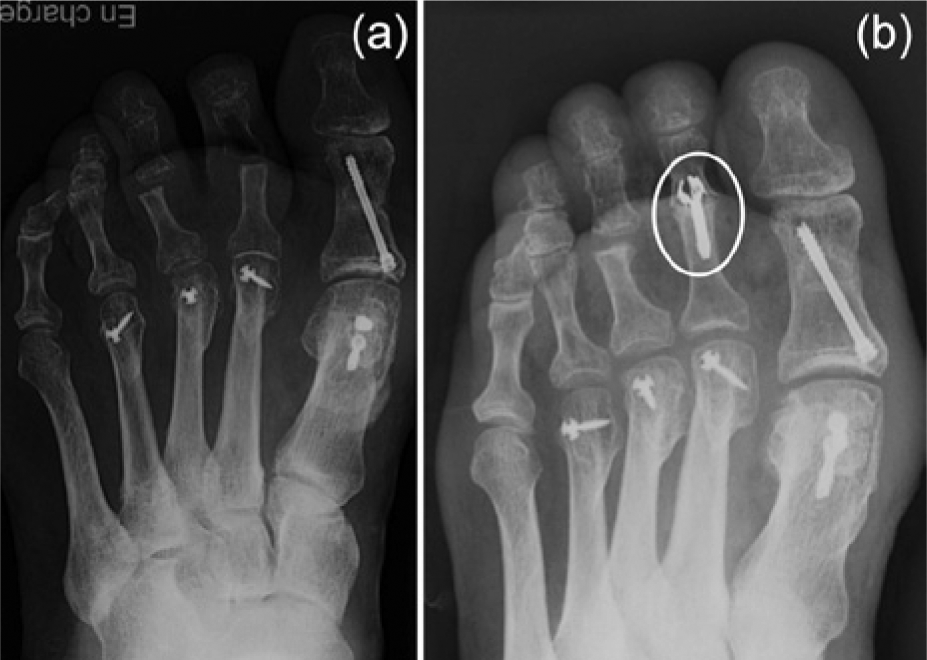
X-rays showing failure of a previous arthroplasty (a) and its treatment using Ipp-On after 9 months of follow-up (b).
Initially, 118 patients were screened for inclusion in the study. In 1 case, the intramedullary device implantation was not possible during the surgery and an arthroplasty of the joint with no fixation was performed. This patient was not included in the subsequent follow-up. A total of 156 toes, in 117 patients were implanted with the Ipp-On device. They were seen at 6 weeks, 6 months, and 12 months postoperatively by the operating surgeons. An additional X-ray evaluation was also performed 3 months postoperatively. Each follow-up assessment included evaluation of joint fusion, X-rays measurement of the PIP joint dorsoplantar angle, American Orthopaedic Foot and Ankle Society Lesser Metatarsophalangeal-Interphalangeal Scale (AOFAS-LMIS), presence of pain, toe alignment, and toe pulp contact to the ground. Patients were asked to rate their satisfaction regarding the operation (excellent = no pain, no shoe restrictions, and no activity limitations; good = occasional pain, shoe modifications, but no activity limitations; fair = pain or deformity limit activities; poor = pain is continuous and activities are restricted, or patient is unchanged or worse than before the operation). Complications encountered either during the surgery or postoperatively were recorded.
Four patients were lost to follow-up during the course of the study: 1 patient (2 toes) before the 6 months visit and 3 patients (5 toes) before the 12 months visit. The implant was exchanged with a K-wire in 1 patient because of implant loosening. This patient was not evaluated after this revision.
Of the 118 patients screened for inclusion in the study, 88.1% were female. They were 65.8 years old in mean (SD = 10.1) and had a mean body mass index (BMI) of 25.1 kg/m2 (SD = 4.0). Of them, 5.3% were smokers.
Operative Technique
A transversal or a midline dorsal longitudinal dorsal incision was performed to expose the PIP joint and perform a thorough arthrolysis. With an oscillating saw, respecting predefined angles, a resection was carried out of the head of the proximal phalanx and 2 mm of the base of the middle phalanx. Then the intramedullary canals were prepared with specific hand reamers, adapted to the different shape and size of the 2 phalanges. The Ipp-On implant was first inserted using the specific handle into the middle phalanx, and then into the proximal phalanx through a swinging movement of the toe. The phalanges were brought into contact by gentle manual impaction. Complementary operative procedures aiming to realign the phalanx relative to the metatarsal were performed during the same operation which could include capsulotomy and tenolysis. In case of associated metatarsalgia, percutaneous or Weil osteotomies were done.
The postoperative care was dictated mainly by the associated surgery to the first ray, which occurred in 108 cases (69.2%). If the patient underwent no realignment of the first metatarsophalangeal joint, immediate full weight-bearing with specific postoperative shoes was allowed.
Statistical Analysis
A descriptive analysis of all the collected data was performed. Results are reported as means and standard deviations or proportions and 95% confidence intervals. Statistical analysis was performed using SAS software.
Results
Concerning the operative procedure, anchorage problems of the intramedullary implant into the bone were encountered in 6 cases. In 1 case, an arthroplasty with no fixation was performed. An additional intramedullary K-wire had to be used in 2 cases, and in the remaining 3 cases the operation was repeated using a new Ipp-On device. During the operation, tenolysis, and metatarsophalangeal capsulotomy were performed in 69.4% of the cases. Metatarsal osteotomy was done in 59.2% of the cases on the corresponding metatarsal bone.
Complications
Intraoperative complications were reported in 2 patients (2 toes out of 156, 1.3%). In both cases, a fracture of the proximal phalanx occurred during preparation of the bone with the hand reamer requiring no fixation in 1 case and a cerclage in the other. Postoperatively, 5 patients (5 toes out of 156, 3.2%) had complications. Three cases of implant loosening were found (Figure 3). In 1 case, an early reoperation was needed and the intramedullary device was exchanged for K-wire fixation 11 days after the initial surgery. In the 2 other cases no secondary surgery was needed. Also, 1 implant breakage, which did not require a secondary surgery, and 1 superficial infection were reported. One year after the operation, a mallet toe deformity was found in 3 cases (2.0%), with pain in 1 case. No reoperation was planned for these patients.

X-rays showing implant loosening; anteroposterior (a) and lateral (b) views.
Clinical Assessment
The proportion of joints fused on X-rays increased during the follow-up (Figures 4 and 5). Six weeks after the operation, 23.9% of the operated joints were fused (95% CI: 17.2, 30.6). This proportion grew to 44.7% (95% CI: 36.8, 52.6) after 3 months (Figure 4), and 67.3% (95% CI: 59.9, 74.8) after 6 months. After 1 year of follow-up, 124 joints were fused (83.8%; 95% CI: 77.8, 89.7). The mean dorsoplantar angle of the PIP joint was 40.3 degrees (SD = 19.1 degrees) preoperatively. It was improved to a mean of 13.7 degrees (SD = 5.0 degrees) immediately after the operation. The angle was maintained at a mean of 14.7 degrees (SD = 5.5 degrees) 1 year after the operation (Figure 6).
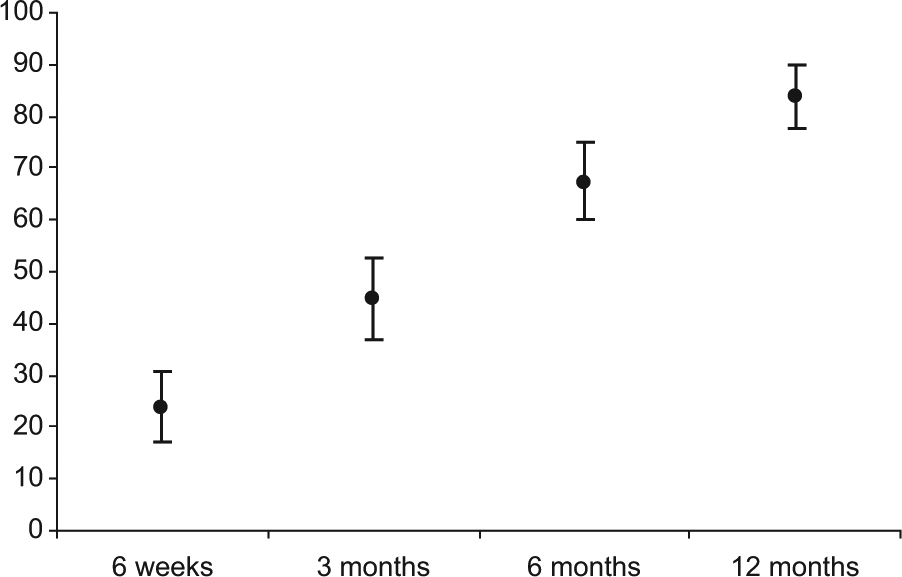
Fusion rate assessed by X-rays 6 weeks, 3 months, 6 months, and 12 months after the surgery. Proportions (%) of fused PIP joints (95% confidence interval) are presented.

X-rays and picture showing postoperative appearance after 3 months (a to c).
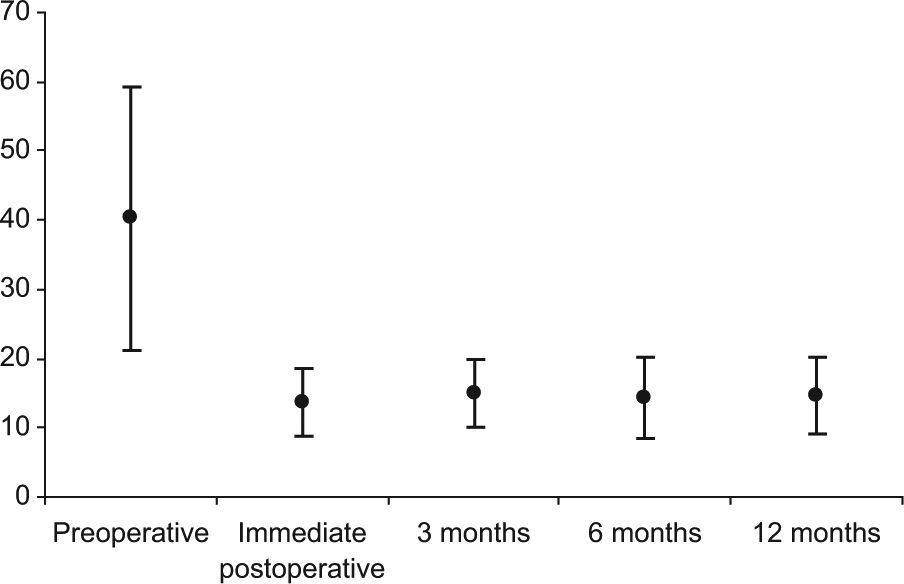
PIP dorsoplantar angle assessed by X-rays preoperatively, immediately postoperatively and 3 months, 6 months, and 12 months after the surgery. Mean angles (°) on X-rays and standard deviations are presented.
Functional evaluation using AOFAS-LMIS showed an improvement from a score of 40.4 (SD = 18.3) preoperatively to 84.3 (SD = 84.0) after 6 months and 85.5 (SD = 9.2) after 1 year (Table 1). The proportion of patients with pain was 15.5% after 6 weeks and decreased to 4.7% after 1 year. The alignment of the toe was satisfactory in 95.9% of the cases after 1 year, and the toe pulp was in contact with the ground in 78.9% of the cases (Table 1). Overall, 98% of the patients were satisfied about the operation (excellent or good; Table 1).
Clinical Assessment Performed by the Surgeons and Satisfaction Evaluated by the Patients at the 12-Month Visit.
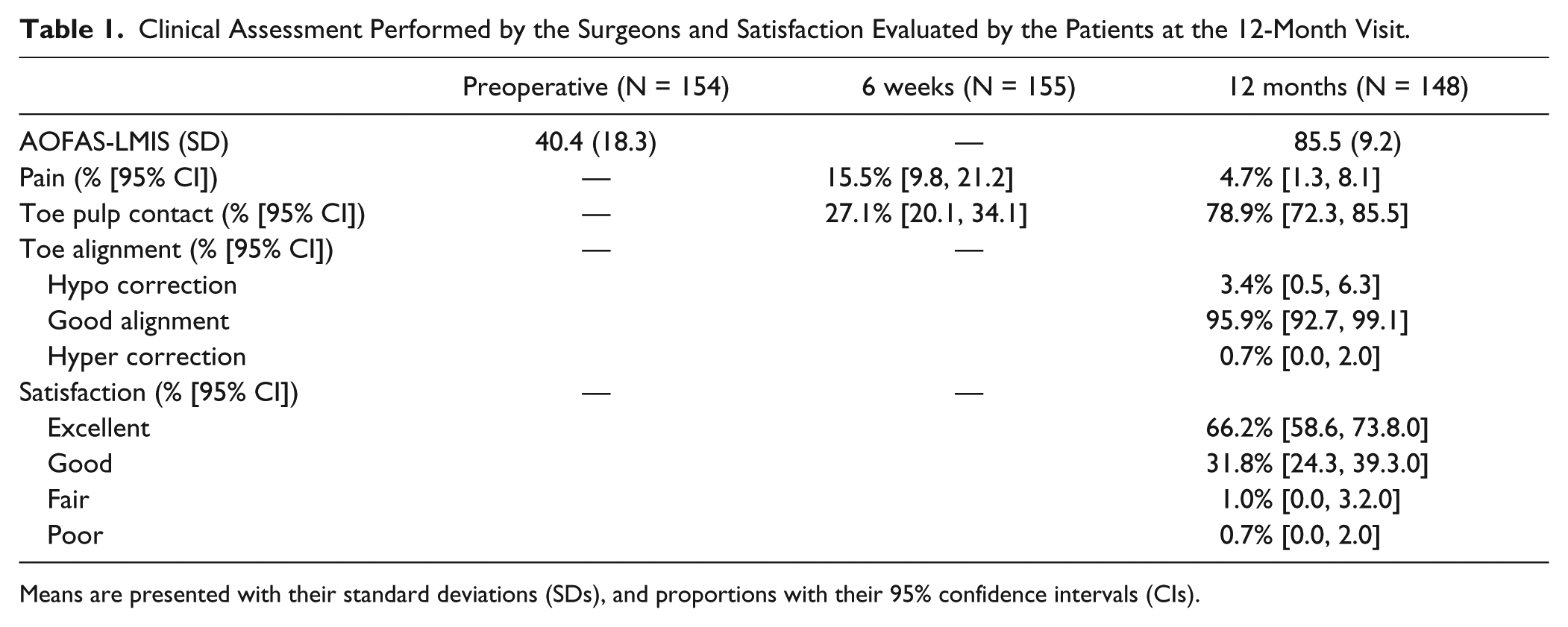
Means are presented with their standard deviations (SDs), and proportions with their 95% confidence intervals (CIs).
Patients with incomplete fusion of the PIP joint 1 year after the operation were analyzed as a subgroup (Table 2). Their AOFAS-LMIS improved from of 36.7 (SD = 18.9) preoperatively to 84.2 (SD = 10.1) postoperatively. These patients reported pain in 8.3% of the cases after 1 year. The alignment of the toe was satisfactory in 87.5% of the cases, and the toe pulp was in contact with the ground in 75.0% of the cases (Figure 7). These patients estimated their satisfaction regarding the operation as excellent or good in 91.6% of cases (Table 2). Only 1 patient (2 operated toes) rated his satisfaction as fair because of pain limiting his activities and incomplete correction on both toes.
Clinical Assessment and Satisfaction for Patients (24 Toes) With Incomplete Fusion at 12 Months.
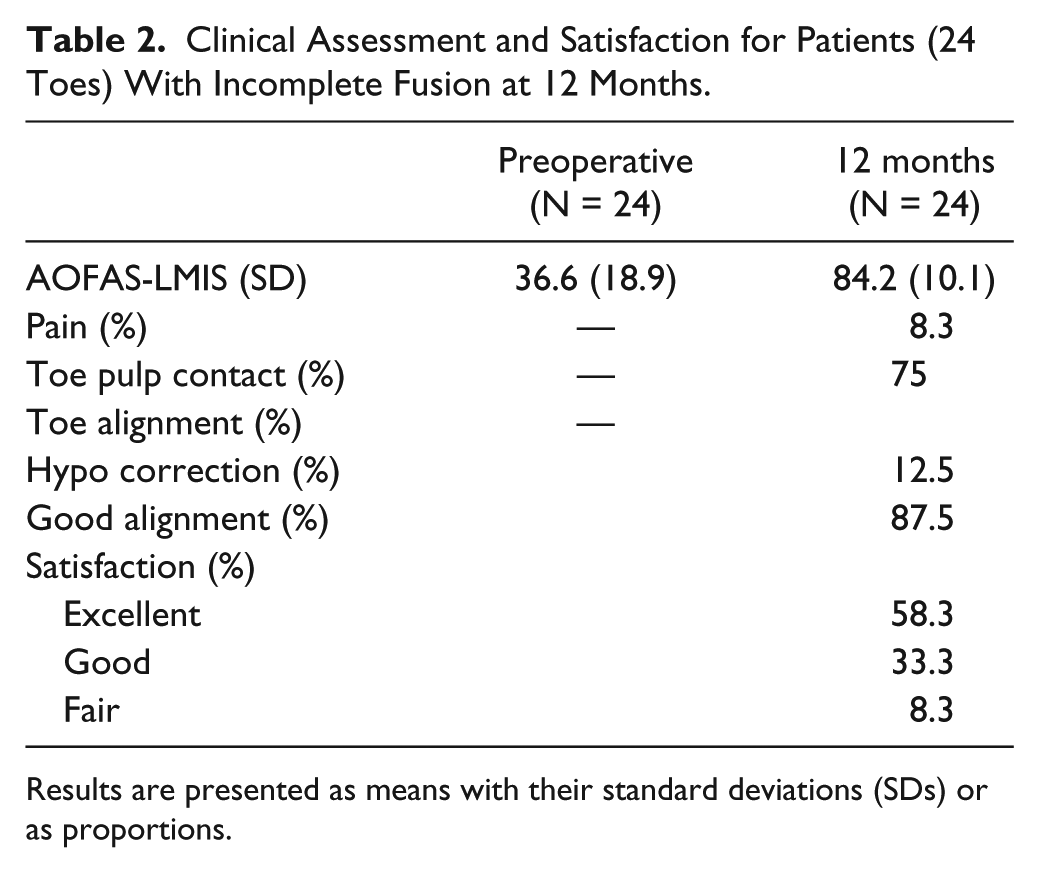
Results are presented as means with their standard deviations (SDs) or as proportions.

Pictures and X-rays showing preoperative appearance (a, b), immediate postoperative X-ray control (c, d), after 12 months with complete healing and pulp contact (e, g).
Discussion
This prospective multicenter study provides clinical data about patients with lesser toe deformities requiring operative correction. An intramedullary implant specifically designed for this indication was used. Indeed, a total of 117 patients with 156 operated toes were followed for 1 year after the operation, which represents a large number of patients. Similar recent studies gathered data on case series of 7 to 47 toes.3,5,7,9,10 Only 1 study published in 2013 reported the results of PIP arthrodeses on 117 toes. 8 Another strength of our study is its prospective design, as most of the publications about lesser toe deformity surgery are retrospective case series. The aim of our study was to provide clinical outcome data after implantation of the Ipp-On intramedullary device. Complications related to the operation and to the device were also assessed.
The number of complications was low (6.5% overall), and a reoperation was required in only 1 case out of 156 because of early recurrence (0.6%). As a comparison, a rate of revision surgery of 8.6% was reported with the SmartToe implant. 8 After PIP arthroplasty, a recurrence rate around 8% can be found.2,4 The cost of the Ipp-On implant is similar to other specifically designed devices that can be found on the market and around 20 times more expensive than a simple Kirshner wire. However, from our results, the very low reoperation rate and the high patient satisfaction could probably balance the extra cost related to the implant. A medico-economic study would be necessary to confirm such a hypothesis.
In the present study, mallet toe deformity was reported in 2.0% of the cases 1 year after the operation. As a comparison, mallet toe can be found at rates as high as 23% with SmartToe implants arthrodesis, 7 or nearly 8% in PIP arthroplasty. 2 This distal interphalangeal deformity is believed to occur because of the too straight position of the PIP joint following realignment. The Ipp-On implant was angulated to obtain adequate plantarflexion of the PIP joint and it could be argued that the limited number of mallet toes reported in our study is related to this plantar angulation.
Among the 156 operated toes, 124 (83.8%) showed a complete fusion on X-rays 1 year after the operation. This proportion is comparable to results reported in the literature, which differ according to the type of fixation used. Konkel et al reported a fusion rate of 83% with absorbable pin fixation, 5 Ellington et al reported a rate of 60.5% with StayFuse implant 3 , and Roukis et al reported a rate of 93% with SmartToe implant, which also included a high rate of mallet toe. 7 The recent article by Scholl et al reported a fusion rate of 68.9% with the SmartToe implant. 8
The PIP dorsoplantar angle was also measured on X-rays. A marked improvement of the mean angle was observed after the operation and maintained throughout the follow-up period. Also, 1 year after the operation, the alignment of the toe was good in more than 95% of the cases. The toe pulp was in contact with the ground in nearly 80% of the cases. After PIP arthroplasties, hyperextension was reported for 13% of toes 2 when temporary fixation was used, and toes not in contact with the ground were reported in 20% of the cases without any fixation. 6 The rate of toe pulp contact was not mentioned in studies about the use of other intramedullary devices designed for PIP arthrodesis. However, we believe that the angulated position of the toe is an important issue for the functional outcome as well as patient satisfaction. Here, we obtained a rate of toes not in contact with the ground comparable to operations preserving PIP mobility but without the complications associated to arthroplasty. Indeed, the Ipp-On design allows for effective fixation of the implant into the middle phalanx. It also provides an angulated position of the PIP joint. Together with appropriate release of tendons, these features lead to an effective fusion with plantarflexion of the toe and pulp contact to the ground. Because of these results, nearly all the patients were satisfied with the operation (98%).
The functional outcome of patients was assessed using AOFAS-LMIS. The score increased above 85 points to reach a level similar to what is found in the literature with other fixation methods.1,5,9 Importantly, patients reported pain only for 7 of the 156 operated toes. The measurements performed for the patients (24 toes) with incomplete radiological fusion 12 months after the operation showed an AOFAS-LMIS similar to the whole group of patients. Toe malalignment and toe pulp not in contact to the ground were reported slightly more frequently than for the whole cohort of patients, but not for the majority of the cases. Of the patients with incomplete fusion, only 2 (8.3%) reported pain. Moreover, these patients were satisfied in more than 90% of the cases, and none of them needed a reoperation. These results showed that even in cases of nonunion, function was restored, pain was absent, and patients’ satisfaction was high.
The technique for Ipp-On implantation is simple and reproducible, even if it requires precision, and the use of a micro-saw. The main difficulty would be the abnormal perforation of the intramedullary canal, which remains rare. The implantation was performed during this study by 5 different surgeons without any difficulty. We believe that a short learning curve is probably required for the first 5 implantations.
Conclusion
Our study showed that the use of the Ipp-On intramedullary implant in PIP joint arthrodesis for lesser toe deformities resulted in a high rate of fusion, a good functional outcome, a low proportion of secondary mallet toe deformity, and no pain 1 year after the operation. Furthermore, patients were highly satisfied with the result of the operation. In patients with no fusion of the arthrodesis site 1 year after the operation, a good outcome and no reoperation were reported, suggesting sufficient stabilization of the PIP joint. However, these data are noncomparative, and further studies are required to allow for a direct comparison between the different fixation devices available.
Footnotes
Acknowledgements
The authors acknowledge Marilyne Blanc and Séverine Oudin.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One or more of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article: JYC and OL are designers from the Ipp-On device. JYC is a member of the Speaker Bureau of Integra LifeSciences Inc.
Funding
The author(s) declared receipt of the following financial support for the research, authorship, and/or publication of this article: Support for the research came from Integra LifeScience Services (France).