
Abstract
Background:
A few studies report correlations between radiographic and anatomic measurements of the distal metatarsal articular angle (DMAA). However, little is known about how the DMAA correlates with the hallux valgus angle (HVA) and with anatomic and clinical radiographic measurements.
Methods:
We dissected, measured, and radiographed 39 cadaveric feet for evidence of hallux valgus and the DMAA. We then correlated these values with paired clinical radiographic measurements made by physician evaluators.
Results:
Physician measurement of DMAA and anatomic measurement of DMAA were significantly correlated with a mean r = 0.64 (evaluator range, 0.44-0.66). Pairwise correlation between physician evaluators ranged from r = 0.63 to 0.84. Sixty-six percent of physician-measured DMAAs were within 5 degrees of anatomic DMAA.
Conclusion:
The percentage of radiographic DMAAs that were within 5 degrees of anatomic DMAAs was only 66%. Additionally, the DMAA was increased in the specimens with moderate and severe hallux valgus compared with those with normal or mild hallux valgus angles.
Clinical Relevance:
The DMAA is an important consideration in patients with hallux valgus. While it is less reliable than other radiographic measures, it was correlated to deformity severity in specimen with hallux valgus.
First described in 1960 by Piggot, 21 the distal metatarsal articular angle (DMAA) is an important consideration in the treatment of hallux valgus. In his review of 216 adolescent bunions, Piggot recognized that 9% of these patients retained a congruous, well-aligned hallux metatarsophalangeal (MTP) joint despite the bunion. He noted that this congruous hallux valgus deformity was typically stable and did not appear to progress with time. Since then, several authors have confirmed a radiographic relationship between the DMAA and a congruent MTP joint in 2% to 9% of patients with hallux valgus.7,8,11,12 This relationship is important clinically. When one is considering correction of a hallux valgus deformity, if there is a large deformity associated with an increased DMAA, correction through a proximal osteotomy or an MTP joint arthrodesis and a distal soft tissue procedure may result in an incongruent joint. In this case, while the hallux valgus angle (HVA) may be reduced, the joint becomes incongruent and an extra-articular realignment of the joint surface may make more clinical sense.2,5,9,17,18
While a few studies report correlations between radiographic and anatomic measurements of the DMMA,1,4,27 few report correlations in first rays with an increased HVA or with weight bearing. 1 The aim of this study was to investigate the relationship between the anatomic DMAA measurement, the radiographic DMAA measurement, and the correlation between observers. We also examined the relationship between the DMAA and the HVA.
Materials and Methods
Thirty-nine cadaver limbs were obtained that included an intact foot and ankle with at least 20 cm of tibia remaining. Specimens with previous surgery or other notable pathologic abnormalities were excluded from the study. The mean age of the donors was 79 years (range, 45-95 years). The age was unknown in 6 specimens. There were 12 male and 22 female specimens. The gender was unknown in 5 specimens. Twenty-one left and 18 right lower extremities were included. There were 6 matched pairs.
The specimens were thawed to room temperature. Simulated weight-bearing AP and lateral radiographs were obtained using a previously described device that placed a vertical weight of 35 kg on each specimen while the radiograph was obtained. 15 For the AP view, the beam was inclined 15 degrees from vertical at a distance of 100 cm and centered on the second metatarsocuneiform joint. For the lateral view, the beam was projected horizontally toward the long axis of the foot at a distance of 100 cm and centered at the midpoint of the navicular.
After standard weight-bearing radiographs were obtained, the specimens were disarticulated at the MTP joint and the articular surfaces were marked with metallic beads, the margins of which were agreed upon by 3 foot and ankle fellowship–trained orthopedic surgeons. Repeat weight-bearing AP radiographs were then obtained with the metallic beads.
The HVA and 1-2 intermetatarsal angle (IMA) were measured and recorded using mid-diaphyseal reference points. 14 The radiographic DMAA was also recorded, and 6 foot and ankle fellowship–trained orthopedic surgeons evaluated the relationship of the articular surface of the distal first metatarsal to the diaphysis of the first metatarsal, as described by Richardson et al. 23 The anatomic DMAA was measured from the radiographs that included the metallic beads using a commercial computerized digital templating software package, Orthoview (version 6.0.14).
Correlations between anatomic DMAA and radiographic DMAA and correlations in DMAA measurements between physicians were obtained using the Pearson product moment correlation coefficient r. Correlations were also tested using linear regression extended by the generalized estimating equation method to account for pairs of feet; all significant results remained significant in retesting. 16 An Anderson Darling test was used to establish normality of the data. Student t test was used to compare means between groups. Statistical tests were performed at the .05 significance level. All statistical analysis was performed with R version 2.11.1 software (http://cran.r-project.org/).
Results
Radiographic measurements revealed a mean HVA of 23 degrees (range, 8 to 64 degrees), a mean 1-2 IMA of 11 degrees (range, 6 to 18 degrees), and a mean DMAA of 9 degrees (range, −2 to 21 degrees). Twenty-nine of 39 specimens were considered to have a hallux valgus deformity characterized by an HVA of 15 degrees or greater. Ten of these had an HVA of less than 15 degrees, 8 had an HVA of 15 to 20 degrees, 12 had an HVA of 21 to 30 degrees, and 9 had an HVA of greater than 30 degrees. The mean anatomic DMAA was found to be 8 degrees (range, −6 to 26 degrees). The mean radiographic DMAA was found to be 9 degrees (range, −3 to 21 degrees). With the numbers available, no significant difference was detected between the mean anatomic DMAA and the mean radiographic DMAA (P = .27).
Correlation Between Anatomic and Radiographic DMAA
Correlations between the anatomic DMAA and the radiographic DMAA are shown in Table 1. Significant correlations were found between radiographic DMAA and anatomic DMAA, with correlations ranging from 0.44 to 0.66. Anatomic DMAA was significantly correlated with mean radiographic DMAA (r = 0.64, P < .001).
Estimated Pearson’s Correlation Coefficient (r) Between Anatomic and Radiographic DMAA.
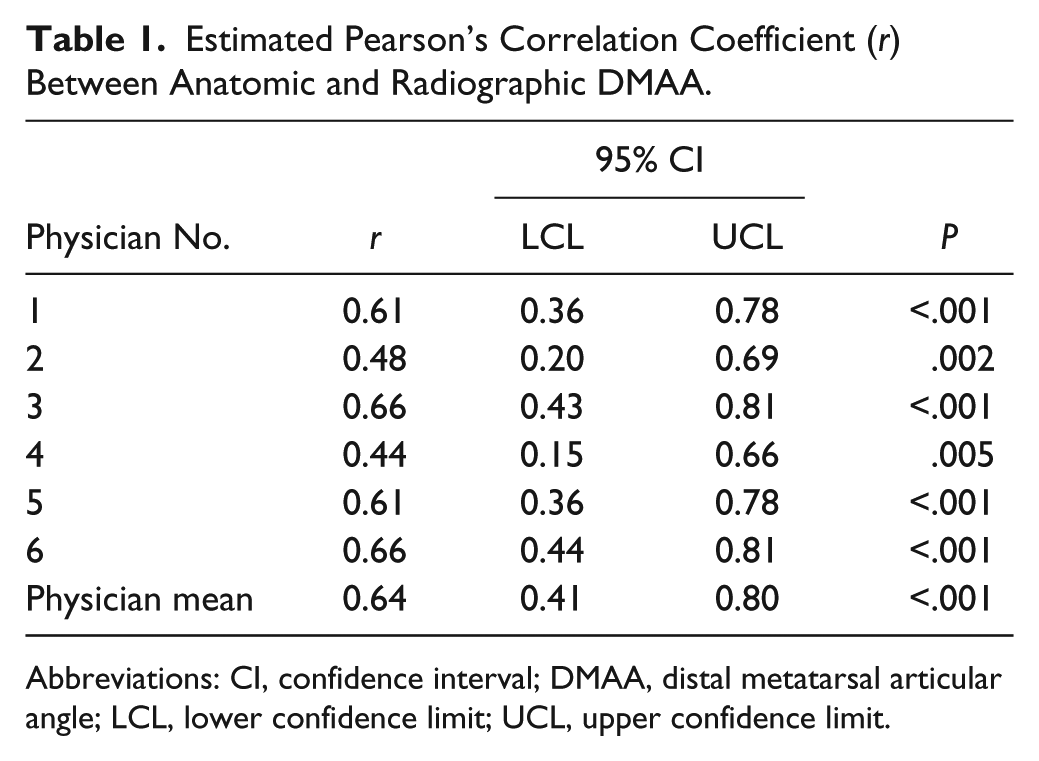
Abbreviations: CI, confidence interval; DMAA, distal metatarsal articular angle; LCL, lower confidence limit; UCL, upper confidence limit.
Difference Between Anatomic and Radiographic Measurements
The mean difference between the anatomic DMAA and the radiographic DMAA measurements was 4.1 degrees with a standard deviation of 4.0 degrees. Figure 1 shows the mean absolute difference between the anatomic and mean radiographic measurements for each specimen. For 22 of the 39 specimens, the difference between the measurements varied by 4 degrees or less. The other 17 of the 39 specimens differed by more than 4 degrees with 2 outliers. Excluding the 2 outliers, the mean difference was 3.4 degrees with a standard deviation of 2.6 degrees. The percentage of radiographic DMAAs that were within 5 degrees of anatomic DMAAs was 66%.
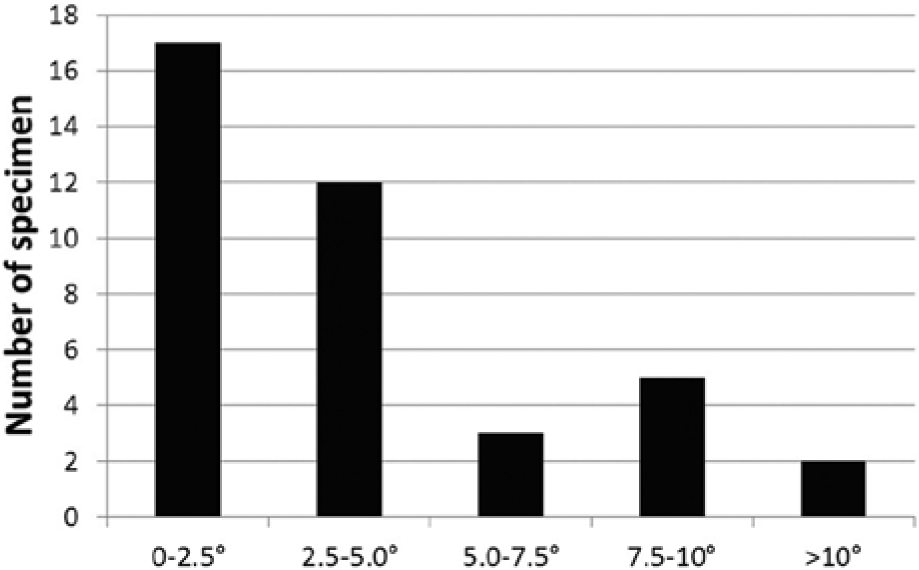
Difference between anatomic and radiographic distal metatarsal articular angle.
DMAA and Hallux Valgus
The mean anatomic DMAA in the specimens with a normal or mild HVA (HVA ≤20 degrees) was 3.2 degrees, with a standard deviation of 4.7. This mean was statistically lower than the anatomic DMAA in those specimens with a moderate or severe HVA (>20 degrees), mean 12.4 degrees and standard deviation 6.6 (P < .001). The relationship between the anatomic DMAA and HVA was examined. The correlation coefficient between the anatomic DMAA and HVA was r = 0.78, which shows a moderately strong relationship. Even without excluding incongruent hallux valgus deformities, a relationship exists between larger HVAs and larger anatomic DMAAs.
Interobserver Reliability
Interobserver reliability, or the degree to which there is agreement among physicians, was explored as shown in Table 2. A significant positive correlation was found between all pairs of physicians.
Pairwise Linear Correlation (r) in Measured DMAA Between Physicians.
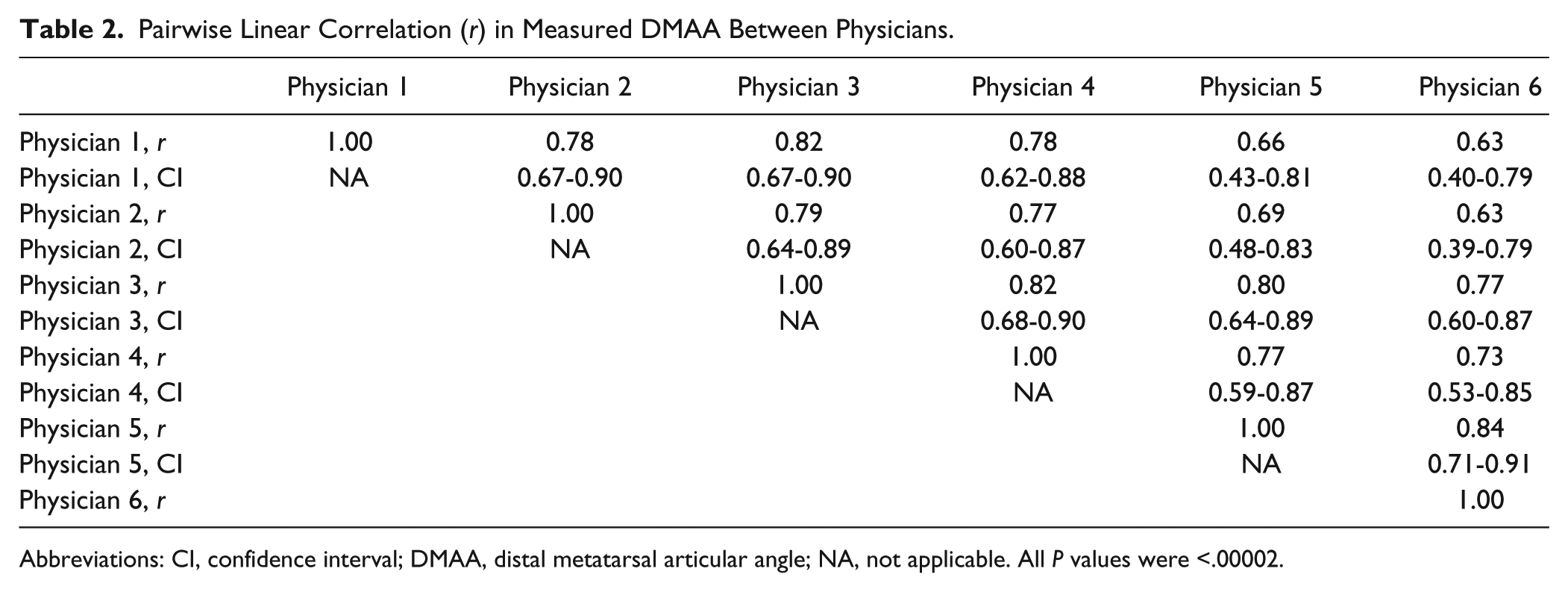
Abbreviations: CI, confidence interval; DMAA, distal metatarsal articular angle; NA, not applicable. All P values were <.00002.
Discussion
The purpose of this study was to examine the relationship between radiographic DMAA measurement, anatomic measurement, and their relation to hallux valgus. The ability to identify and quantify a congruent first MTP joint in hallux valgus is important when considering operative treatment of hallux valgus deformity because it can influence the choice of surgical procedure.6,11,12,20 We found a correlation between anatomically measured DMAAs and radiographic DMAAs. We found that those specimens with a greater HVA also had a greater DMAA, which provides additional data on DMAA measurements in the hallux valgus population.
The published literature on the DMMA, its interpretation, and its role in clinical treatment is variable. Richardson 23 studied 100 cadaveric feet without hallux valgus and found the DMAA to average 6.1 degrees with a range from −3 to 26 degrees. This is consistent with subsequent studies.1,3,19,25
Hallux valgus itself is a complex deformity. Six degrees of freedom contribute to the anatomic description of the first ray, yet most clinical tools use only 2 dimensions. Robinson et al 24 demonstrated this effect, showing that rotating the first metatarsal 30 degrees altered the DMAA by about 10 degrees. However, the DMAA values of their specimens varied by up to 40 degrees for any given degree of rotation, which makes their results difficult to extrapolate. 24 These results are in direct conflict those of Vittetoe et al, 27 who found that the DMMA was relatively insensitive to changes in longitudinal rotation and varus deviation of the first metatarsal. Those investigators found good intraobserver reliability between radiographic DMMA calculation with and without metallic beads marking the articular surface and good interobserver reliability with metallic bead markings but poor interobserver reliability on standard radiographs. 27
Even with the poor reliability reported by Vittetoe et al, 27 the difference between the standard clinical method of measuring the DMMA and the investigators’ best radiographic estimate of the true DMAA averaged only −0.9 ± 2.4 degrees. This implies that clinicians will estimate the DMAA within 5 degrees 95% of the time. The observers in the current cadaver study did not produce this degree of precision in measurement.
Amarnek et al 1 determined that preoperative radiographic measurements of the DMAA varied notably from measurements made intraoperatively: Preoperative DMAA measurements were on average 7 degrees less than intraoperative measurements, although the investigators were only able to measure intraoperatively to the nearest 5-degree increment. Sullivan et al 26 showed poor interobserver reliability for DMAA measurement in 8 different weight-bearing AP radiographs. Those investigators demonstrated 95% confidence intervals between 3 and 8 degrees of interobserver variability. 26 Chi et al 4 similarly reported difficulty in consistently and accurately assessing the DMAA, although their reporting method has been questioned. 10 To help improve interobserver variability, Pique-Vidal et al 22 introduced computerized angular measurement and showed improved reliability compared with a standard goniometer. Pique-Vidal et al made 2 additional important observations. First, they included varying degrees of hallux valgus deformity in their study, and second, they observed that while computerized measurements were more reliable than a goniometer, in patients with larger HVAs the 2 techniques demonstrated similar angular measurements. The current study further contributes to this literature by combining the use of computerized measurement with anatomic dissection and marking in patients with hallux valgus.
Coughlin and Freund 13 found variable accuracy in measuring the DMAA in their study of 25 weight-bearing radiographs. They found that physicians were 96.7% reliable in the measurement of the 1-2 IMA, 86.2% reliable in the measurement of the HVA, and only 58.9% reliable in the measurement of the DMAA, further questioning the interobserver reliability of the DMAA. Coughlin and Freund noted that some reviewers were more accurate than others and also found that some radiographs were more difficult to assess than others. In a similar way, our findings support the concept that the DMAA is less accurate than values reported by Coughlin and Freund for the HVA and 1-2 IMA and that some radiographs are more difficult to assess than others. Figure 2 shows 2 radiographs, one that had good agreement between reviewers and the anatomic measurement and one that did not. Our findings also support the conclusions of Coughlin and Freund, in that we believe it is inappropriate to compare the reliability and accuracy of angular measurements such as the HVA and the 1-2 IMA with the DMAA because the landmarks for measuring the DMAA are decidedly more difficult and variable to measure. The reference points may vary depending on the posture of the foot, which can alter the alignment or rotation of the first metatarsal.
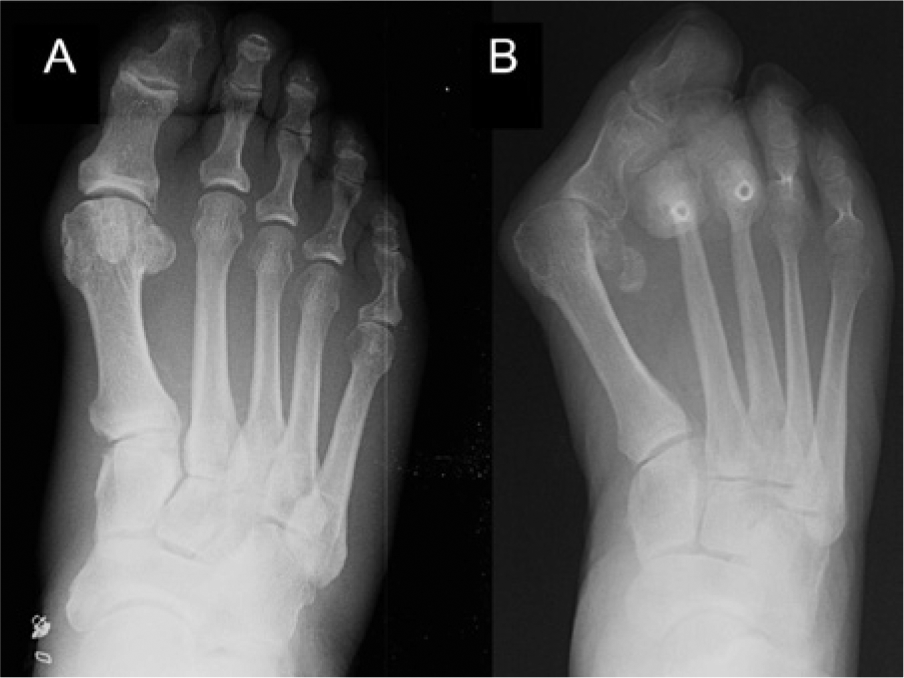
(A) AP radiograph of a cadaver specimen with good agreement between clinical and anatomic distal metatarsal articular angle (mean difference, 0.4 degrees), and (B) poor agreement (mean difference, 20.7 degrees).
In the current study, we noted 2 outlying specimens when examining the difference between anatomic and physician-measured specimens. In one specimen a difference of 21 degrees was observed, and in the other a difference of 12.7 degrees was observed. Both of these specimens had severe hallux valgus deformities (55 and 64 degrees, respectively) with degeneration of the first MTP joint (Coughlin-Shurnas grade 4), which we suspect contributed to error in clinical radiographic measurement. This may be an important factor to consider in surgical decision making as well. This is important because in cases of severe MTP degeneration or severe hallux valgus, the clinical value of the DMAA is diminished.
This study has several limitations. First, it is a cadaver study, which does not take into consideration patient symptoms related to hallux valgus and limits the applicability of the study results to living subjects. Second, an attempt was made to create a gold standard by which to compare clinical radiographic DMAA values. We did this by having 3 fellowship-trained surgeons mark the articular surface and by using computer software to measure the angle. There still may be inaccuracy in this method.
Conclusion
The mean difference between the anatomic DMAA and the radiographic DMAA measurements was 4.1 degrees with a standard deviation of 4.0 degrees. However, the percentage of radiographic DMAAs that were within 5 degrees of anatomic DMAAs was only 66%. Although statistically significant correlations were observed between anatomic DMAA and radiographic DMAA, interobserver reliability was lower than for other published values of first ray radiographic measurements. Additionally, the DMAA was increased in the specimens with moderate and severe hallux valgus compared with those with normal or mild HVAs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.