
Abstract
Background:
Metatarsophalangeal joint (MPJ) instability, which often involves the second ray, may result in dorsal translation and coronal drift of the proximal phalanx, with subsequent crossover of the first and second toe. After traditionally described soft tissue and osteotomy procedures are used to treat this deformity, coronal plane malalignment may persist, but few additional surgical options have been described to address this problem.
Methods:
We present a retrospective series of 5 patients who underwent a supplemental technique to augment coronal plane MPJ realignment. All patients underwent preplanned concomitant procedures. Crossover angulation of the second MPJ, amount of coronal translation required, and overall first-second ray alignment were compared pre- and postoperatively.
Results:
Depending on the severity of refractory deformity after soft tissue release and decompressive metatarsal osteotomy, 1.5 to 4.5 mm of coronal plane metatarsal head translation was required to achieve 3 to 20 degrees of overall valgus correction at the MPJ and complete correction of the crossover toe deformity. All patients were satisfied and had good function at last follow-up, a mean of 10.2 months, although 3 patients exhibited some level of second MPJ stiffness. One patient ended up with a component of residual floating toe deformity that was considered more of an incomplete correction of dorsal MPJ subluxation rather than any technical complication of this translational osteotomy modification designed to primarily correct coronal plane malalignment. A second patient had asymptomatic angular malalignment through partial (coronal plane) malrotation of the metatarsal osteotomy before it had healed.
Conclusions:
We have found this technique modification to be a very effective and simple means of treating recalcitrant lesser MPJ coronal plane malalignment when traditional soft tissue and bony techniques fail to fully restore anatomic MPJ position.
Level of Evidence:
Level IV, retrospective case series.
Metatarsophalangeal joint (MPJ) instability is a common clinical dilemma for foot and ankle surgeons. This condition is an important component of many lesser toe deformities and has a particular predilection for the second ray. From an etiological standpoint, idiopathic capsulitis, chronic MPJ overload, and attenuation with eventual failure of the plantar plate are typically associated with dorsal translation and, ultimately, dislocation of the proximal phalanx at the MPJ.3,5,8,11 Varus or valgus deviation, however, is also quite common in these settings, due to concomitant deficiency of the collateral ligaments and progressively unbalanced muscular forces across the joint, as originally described by Deland and Sung. 6 The combination of dorsal translation and coronal (usually medial) drift of the proximal phalanx at the second MPJ often results in symptomatic impingement or overt crossover deformity between the first and second toes.5,6 It can be extremely challenging to not only obtain but also maintain satisfactory reduction of this deformity. No clear consensus for the optimal operative management of crossover deformity exists, although multiple procedures have been proposed,1,4,9,10,12,15 and additional correctional translation of the metatarsal osteotomy in the transverse (coronal) plane, to our knowledge, has been mentioned in the literature only rarely.2,7
The most common initial operative approach for second MPJ instability involves soft tissue rebalancing with various capsulotomies and tendon procedures. With varus deformity at the MPJ, for example, dorsal/medial pericapsular releases in addition to extensor release/centralization, lengthening, and/or transfer (eg, intrinsicplasty) can be undertaken to address dorsomedial subluxation of the second MPJ. If a valgus deformity is present, soft tissue releases are alternatively performed on the contracted lateral side of the MPJ. When substantial deformity remains refractory to soft tissue procedures alone, decompressive metatarsal (MT) osteotomy often becomes necessary to shorten the MT, reduce tension across the MPJ, and enable more acceptable MPJ reduction and realignment. 8 As described by Maestro et al, 14 the need for and degree of shortening may be judged based on the harmonious forefoot morphotype.
Although soft tissue releases in conjunction with the several traditionally described osteotomies remain adequate choices for most crossover toe deformities, in our experience complete correction of varus/valgus (coronal plane) alignment may remain inadequate in some of these cases, necessitating further intervention. Few additional surgical options, however, have been described. Although Barouk 2 introduced the concept of transverse plane translation after distal MT osteotomy in 2005, Devos Bevernage et al 7 were the first to present clinical results using this additional translational bony correction of the MT head after traditional Weil osteotomy and soft tissue release for an overriding second toe. Patient-reported outcome scores were improved substantially, with no recurrence of metatarsalgia, 1 case of transfer metatarsalgia, and no reoperations. Thirty percent, however, still experienced a floating toe phenomenon and some exhibited residual laxity. In light of such findings, it should be noted that investigation of alternative surgical efforts is currently underway by several authors to determine the merits of enhancing postoperative stability at the MPJ via direct plantar plate repair. 16 In the small case series by Devos Bevernage et al, 7 however, no recorded measurement of the required coronal translation or any detailed radiographic description of the second ray coronal plane correction was provided. The current investigation presents a radiographic and short-term outcome analysis of a slightly modified medial translational technique after Maceira osteotomy (as preferred by the senior author, C.W.D.). 13 We believe that when standard interventions are insufficient for complete MPJ correction, this procedure renders a stable and powerful supplemental coronal plane correction to an otherwise refractory second crossover toe deformity.
Methods
Between July 2011 and March 2013, consecutive patients who met inclusion criteria and had been treated with second distal MT osteotomy for a first-second crossover toe deformity were retrospectively identified. A chart review was performed to confirm that all patients met inclusion and exclusion criteria. Patients must have had first-second crossover toe deformity with dorsal dislocation or subluxation of the second MPJ that was irreducible on physical examination, experienced substantial pain and/or callus formation on the plantar aspect of the affected second MT, failed conservative measures, and opted for operative management. Furthermore, included patients must have undergone a second distal MT translational osteotomy due to the severity of their crossover toe deformity. Patients were included whether or not they required any other preplanned procedures for concomitant pathologies, including hallux valgus, hallux valgus interphalangeus, adjacent MPJ instability, hammer toe, or other deformities (Figure 1). Patients were excluded if they required only a standard distal MT osteotomy without translation or had undergone previous second metatarsal osteotomy for a first-second crossover toe deformity.

Preoperative weight-bearing (a) anteroposterior and (b) lateral radiographs. Note subtle dorsomedial translational deformity of the proximal phalanx at the second metatarsophalangeal joint (MPJ), consistent with early crossover impingement and second MPJ instability. Second MPJ angle was defined as the angle between line A, the second metatarsal (MT) shaft, and line B, the second ray proximal phalanx shaft. Overall first-second (crossover) alignment was defined as the angular relation between line C and line B. (Note: For the latter measure, line B would be shifted slightly on the second ray to pass from the base of the proximal to tip of the distal phalanx.)
Of 30 consecutive patients reviewed who had overriding second toes, 5 met all these criteria and were available for follow-up. Patients were aged 56 to 84, all 5 were female, and 4 had a left-sided and 1 a right-sided deformity. All 5 patients required other preplanned procedures at the time of second ray correction, and these included chevron osteotomy (n = 3), Akin osteotomy (n = 4), third metatarsal Maceira osteotomy (n = 1), second ray hammertoe correction (n = 3,) and bunionette (n = 1). One patient had undergone previous chevron osteotomy while another had a prior first MPJ fusion, but otherwise these interventions represented other index procedures for these patients.
Pre- and postoperative clinical notes as well as standard weight-bearing radiographs were analyzed. Patients’ subjective assessment of pain, stiffness, and overall clinical function at last follow-up was determined. Several radiographic parameters were recorded both preoperatively and at last follow-up. Angulation at the second MJP was measured on the standing anteroposterior view and was defined as the angulation of the second ray proximal phalanx shaft relative to the second MT shaft. The amount of coronal translation required intraoperatively was measured on the postoperative standing anteroposterior view and defined as the horizontal distance from the distal MT shaft cortex to the final position of the cortex on the adjacent translated MT head. Overall first-second (crossover) alignment of the first ray relative to the second was also recorded. This was defined as the angle between lines drawn from the base of the proximal phalanx and tip of distal phalanx on the first and second ray, respectively. Examples of these radiographic measurements are included (Figure 1a). Finally, the development of any complication or need for additional surgery related to the index procedure(s) was recorded.
Technique
In terms of the operative procedure, in all cases first ray alignment was restored via either a Modified McBride or transarticular soft tissue release, followed by a chevron or scarf osteotomy. When appropriate, an Akin procedure was included to correct residual hallux valgus interphalangeus. To ameliorate extensor overrecruitment and extrinsic-intrinsic imbalance (tightness), the long extensor to the second ray was transected proximally while the short extensor was cut distally, just proximal to its insertion, and a complete medial or lateral capsular and collateral ligament release was performed to the level of (but not including) the plantar plate, for varus or valgus deformities, respectively.
If residual MPJ contracture was present at that point, a Maceira 3-step modified Weil shortening osteotomy was performed to further decompress the MPJ, allow for congruent joint reduction, and restore MPJ dorsal-plantar competence. Adjacent lesser rays were also addressed with similar procedures if they remained malaligned or had inappropriate lengths in terms of the Maestro parabola, in which lesser metatarsal lengths should decrease by a geometric factor of 2. 14
In the setting of persistent coronal plane MPJ drift and malalignment (Figure 2a), to augment and exact more anatomic realignment, the MT head was displaced in the coronal plane prior to fixation. A dental pick, Anteater rongeur, or Freer elevator was used to adjust and maintain proper MT head position while coronal plane alignment was checked both clinically and radiographically with fluoroscopy. Coronal plane adjustments were made as necessary. For fixation, a single 2-mm solid cortical screw was placed in lag fashion across the osteotomy site following satisfactory reduction (the senior author’s preferred technique). Screw trajectory was slightly offset from the pure sagittal plane in the direction of translation to maximize central purchase within the MT head. Care was taken to ensure that the MT head shift resulted in a purely translational rather than angular (coronal plane) realignment, with adjustments made as necessary prior to fixation until the final MPJ alignment was deemed anatomically congruent.

(a) Intraoperative clinical anteroposterior image after soft tissue releases and decompressive Maceira osteotomy but prior to medial metatarsal (MT) head translation. Note position of second toe and residual medial metatarsophalangeal joint (MPJ)crossover. Dorsal (sagittal plane) translation had already been resolved with the above steps. A simulated “push-up” test was used to simulate the foot’s appearance with weight-bearing. (b) Final intraoperative clinical alignment after the MT head translation procedure.
Finally, the foot was evaluated clinically (Figure 2b) as well as by intraoperative fluoroscopy (Figure 3) to ensure satisfactory alignment of the metatarsals and congruent reduction of the MPJs. Upon completing the bony realignment, the short extensor was transferred to the long extensor for effective intrinsicplasty as per the senior author’s preference for rebalancing, and all incisions were subsequently closed.
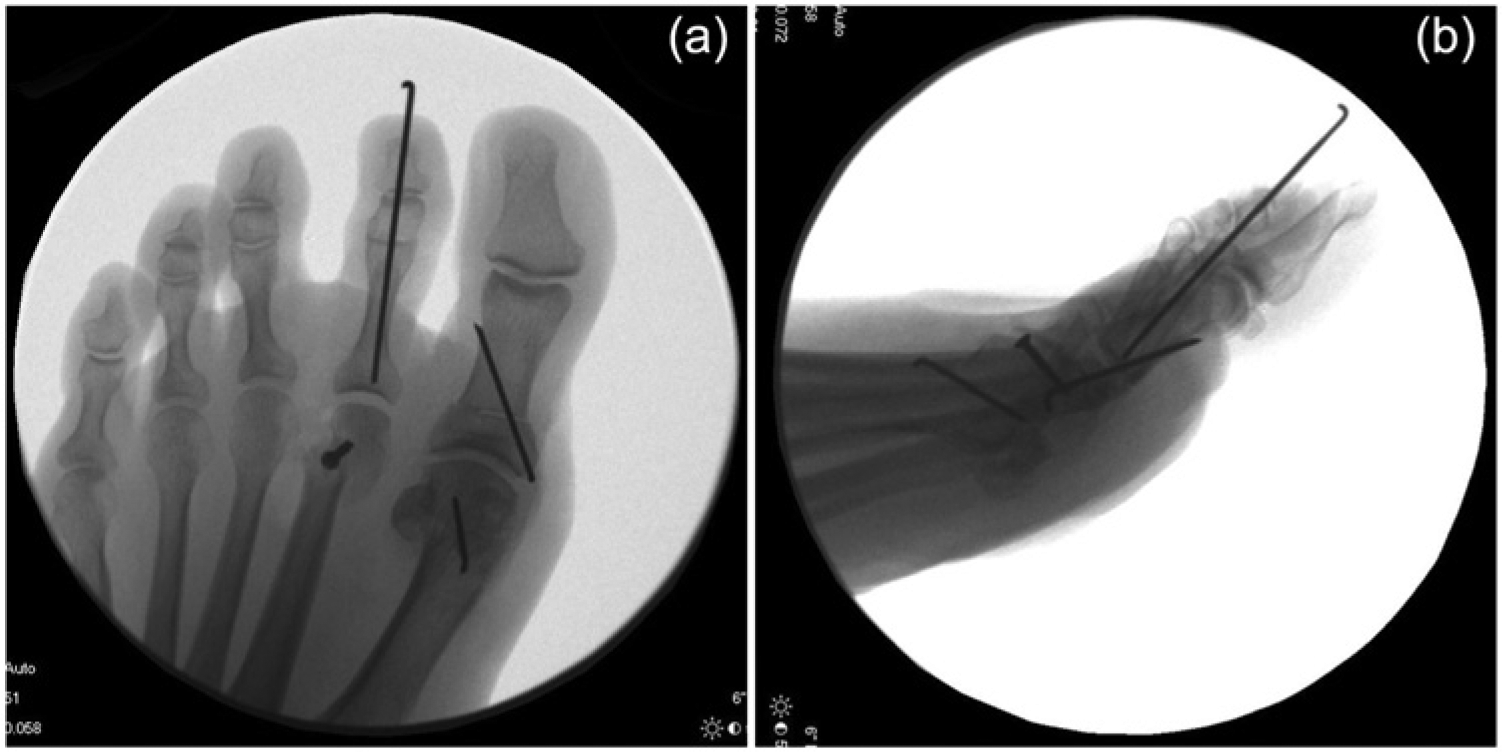
Final intraoperative radiographic alignment: (a) anteroposterior and (b) lateral.
Results
Over the past 2 years, this modified technique of translational distal MT decompressive osteotomy has been used in 5 patients for recalcitrant coronal plane malalignment. In terms of angular deformity at the second MPJ, initial standing anteroposterior radiographic analysis revealed 0 to 27 degrees of varus angulation. Intraoperative medial translation of the second MT head after Maceira osteotomy ranged from 1.5 to 4.5 mm and resulted in a final 3 to 20 degrees of overall valgus correction at the MPJ. Final angulation at the MPJ ranged from 7 degrees of varus to 11.5 degrees of valgus. Overall crossover alignment of the first ray relative to the second changed from 10 to 24 degrees of convergence preoperatively to 2 to 6.5 degrees of divergence after surgery (Table 1).
Pre- and Postoperative Coronal Translation and Angulation a .
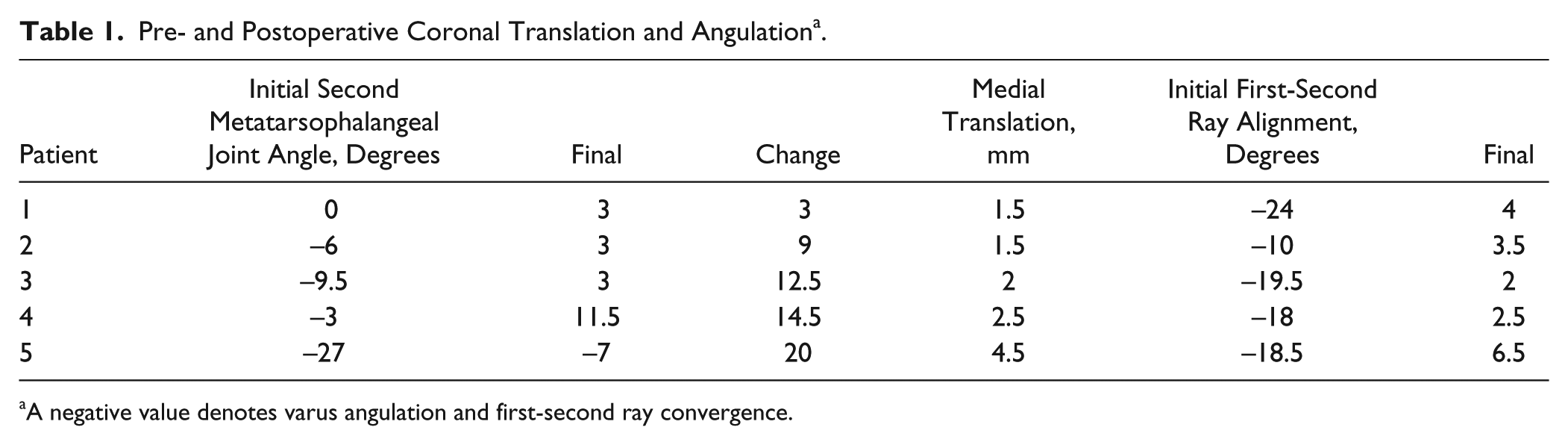
A negative value denotes varus angulation and first-second ray convergence.
All 5 patients maintained reasonable correction of the first-second crossover deformity as well as overall acceptable alignment of all 5 rays at an average follow-up of 10.2 months (range, 4.1-23.3 months). Although all 5 patients proclaimed themselves to be satisfied clinically and to have good function at most recent follow-up, 1 of the 5 patients exhibited a mild residual floating toe deformity and another was found to have developed some mild angular malrotation of the MT head (coronal plane) despite maintenance of initial translational correction at the osteotomy site and overall alignment. Three patients also reported some degree of stiffness but did not feel that this was limiting them functionally. One patient developed irritation and ulceration from a fifth metatarsal Kirschner wire used for bunionette correction, and this hardware required removal at 6 months postoperatively, resulting in symptom resolution. Figures 4-6 demonstrate the clinical and radiographic appearance of a foot before and after surgery.

Preoperative standing radiographic (a, anteroposterior; b, lateral) alignment of a patient with a first-second crossover toe deformity. Note in this case the essentially pure translational rather than angular component of second metatarsophalangeal joint (MPJ) malalignment, which contributed to this patient’s presenting complaint. Also note medial MPJ translation in remaining lesser MPJs.

Final standing postoperative radiographic (a, anteroposterior; b, lateral) alignment after first-second crossover toe correction. Note that this patient also had translational correction through the third metatarsal (MT) because of similar complaints as well as the need to provide adequate “recovery” space for the second ray following its correction. Also note that post correction, these lesser metatarsophalangeal joints (MPJs) maintained reasonably neutral alignment while the undercorrected fourth and fifth MPJs remain persistently medially translated (but clinically asymptomatic).

Final standing postoperative clinical (a, anteroposterior; b, lateral) alignment of the same patient following first-second crossover toe deformity correction, demonstrative of typical final result.
Discussion
Chronic second ray overload and subsequent plantar plate insufficiency lead predominantly to dorsoplantar instability of the second ray. The ultimate imbalance created, however, often leads to a progressive degree of coronal plane malalignment as well. In the worst cases, the stabilizing force of the plantar plate as well as the structural integrity of the collateral and intermetatarsal ligaments is lost, and unimpeded dorsiflexion forces incurred through ambulation lead to dorsal subluxation of the proximal phalanx. The action of the intrinsic muscles then shifts from plantar flexion to dorsiflexion at the MPJ, exacerbating this deformity. Medial drift of the second proximal phalanx and lateral shift of the second metatarsal head, with eventual contracture of the medial structures, develop as a further result of these abnormal biomechanics, including the eccentric pull of the lumbrical muscle and toe flexors. 6
Girdlestone-Taylor-type flexor-to-extensor transfer procedures are still commonly used to augment alignment and stability for crossover toe correction after pericapsular release and standard osteotomy, but results have not approached 80% good to excellent, partly due to the presence of frequent residual deformities.9,15 For split transfer of the flexor digitorum longus to the dorsum of the second proximal phalanx, in one series, 27% of patients exhibited persistent medial deviation and 37% persistent dorsiflexion contracture at the MPJ. 15 In terms of extensor digitorum brevis (EDB) transfer under the transverse metatarsal ligament, residual deformity was common in treated patients, including more than 14% with persistent medial deviation. 9 Kirschner wire fixation has been proposed as an additional technique to augment stability and retention of MPJ alignment, and wires are typically left in place for 2 to 3 weeks postoperatively. It remains unclear, however, whether the addition of such fixation improves long-term results versus traditional bony and soft tissue procedures alone.9,15
Intraoperatively, the effect of standard axial decompressive osteotomy and soft tissue reconstruction for these deficient pericapsular second MPJ structures may be insufficient to correct these aberrant forces and enact proper anatomic realignment. This rationale parallels the manner in which surgeons now approach hallux valgus correction and first MPJ realignment. Historically, experience has shown that soft tissue correction alone (ie, McBride, Silver) for first MPJ coronal plane malalignment is usually insufficient for obtaining and maintaining long-term coronal plane anatomic repositioning of the joint. In fact, successful hallux valgus correction today is rarely performed in the absence of some form of coronal plane translational osteotomy proximal to the MPJ. In cases of residual transverse (coronal plane) second MPJ malalignment, our experience mirrors that of Barouk 2 and Devos Bevernage et al 7 in supporting the addition of coronal plane translation as a further modification of the Maceira or Weil osteotomy to gain more MPJ correction. Even in the presence of an essentially neutral MPJ angle, some degree of preoperative translational malalignment may still be present at the second MPJ and contribute to the deformity. This situation is well demonstrated in the pre- and postoperative radiographs in Figures 4 and 5. In our opinion, patients with such deformity variation benefit equally well from translational osteotomy to fully correct their crossover malalignment.
Radiographic analysis demonstrated that the amount of coronal plane MT head translation required was commensurate with the severity of the crossover deformity and change in coronal angulation required to achieve acceptable alignment. Based on the senior author’s limited experience with this approach, it is believed that the potential risks posed by this technique are no different from those encountered when using the more traditional osteotomies, such as the Weil or the Maceira procedures, and that the learning curve for this technique for the foot and ankle surgeon will be short. Except for 1 case of residual floating toe deformity and 1 case of loss of angular alignment at the MT osteotomy site, no other specific adverse event was encountered.
Attention should be paid to maintaining rigid rotational stability of the translated MT construct. Figure 7 demonstrates healing with partial loss of coronal plane angular alignment in 1 patient despite maintenance of translational correction and overall alignment (compare with Figure 3a). To reduce the risk of such an outcome, it is recommended that in these more extensive corrections the use of 2 screws be considered to augment the osteotomy fixation. While we do not yet have enough clinical experience with this technique to provide any basis for scientific opinion on the advantages or disadvantages of a 2-point fixation approach, we theorize that it may have helped in the case of this patient, who was also the only one in our series to neither perform our routine postoperative therapy protocol nor follow our progressive, graduated weight-bearing program.

Postoperative anteroposterior standing radiograph of patient who developed partial loss of angular alignment with subsequent rotational (coronal plane) malunion through the original osteotomy site who was noncompliant with early restricted weight-bearing precautions.
Based on some recent literature, we are now using and recommend consideration of adding plantar plate repair to this translational osteotomy modification—particularly for the more severe crossover deformities that typically occur in conjunction with significant plantar plate attenuation or tear. 16 This combination of procedures may further enhance MPJ stability and correction and ultimately fare better than historic standards (ie, Girdlestone-Taylor, EDB tendon transfer) in lowering the incidence of postoperative residual floating toe or recurrent malalignment. We are increasingly incorporating both techniques into our operative algorithm for crossover deformity, although we recognize the need for greater patient numbers and longer follow-up to draw any definitive conclusions regarding the efficacy of this approach.
It is acknowledged that this analysis is limited by its small patient pool, relatively short-term follow-up, and its retrospective nature. However, we still consider our early experience to be promising. Over the past 20 years of performing first-second ray crossover corrections in our patients, we have often been dismayed by a lack of complete correction after the varied operative approaches and techniques we have used. Although we neither expect nor purport that this simple modification is going to dramatically alter the outcome after first-second crossover surgery, our early experience with this modification does suggest that it can make a qualitative difference by empowering more traditional approaches without the addition of significant operative time or risk.
In summary, our early experience with this translational MT osteotomy modification has been positive, and we have found it a very effective and simple means of fine-tuning recalcitrant lesser MPJ malalignment after traditionally used soft tissue and bony techniques fail to promote full restoration of anatomic alignment. Although further study incorporating a larger scale, randomized controlled prospective study will be necessary to definitively confirm these initial impressions, we propose that this translational osteotomy technique modification might represent a potentially useful complement to either the more standard approaches or those which now also include plantar plate repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.