
Abstract
Background:
Osteochondral lesions of the talar dome (OLT) involve the articular cartilage and/or subchondral bone. The subchondral bone plate plays an important role in cartilage metabolism. We hypothesized that the findings of subchondral bone on CT image would be related to the cartilage damage of OLT. The purpose of this study was to evaluate the relationship between the arthroscopic and CT findings focused on subchondral bone.
Methods:
Thirty-one ankles diagnosed as OLT were analyzed. All patients underwent CT, MRI, and arthroscopic surgery. The CT findings for both the cystic and fragment lesions were classified into 3 types. The 3 types for the cystic lesion ankles were irregular shape, round shape with sclerotic wall, and irregular shape with opening to an articular cavity. The 3 types for the fragment lesion were no bone absorption, bed absorption without fragment absorption, and bed sclerosis and fragment absorption. The subchondral bone findings on CT were compared with International Cartilage Repair Society (ICRS) grades and arthroscopic grading.
Results:
All round and sclerotic cystic lesions revealed cartilaginous flap lesions with a nearly normal cartilage surface. An irregular shape with opening revealed an unstable lesion with severely damaged cartilage. As for fragment lesions, no absorption revealed a stable lesion with a nearly normal cartilage surface. Bed absorption revealed an unstable lesion with a nearly normal cartilage surface. Fragment absorption with bed sclerosis showed an unstable lesion with severely damaged cartilage. There was a significant difference between CT findings and ICRS grade or arthroscopic findings (both P < .01), while there was no significant difference with MRI grading. The diagnosis of cartilage status by CT was better than MRI.
Conclusion:
CT findings for OLT based on subchondral bone related to cartilage damage. This study showed that CT was a useful tool for evaluating cartilage damage in OLT.
Level of Evidence:
Level III, comparative case series.
Osteochondral lesions of the talar dome (OLT) involve the articular cartilage and/or subchondral bone, and there are several patterns of lesions. In 1959, Bernt and Harty classified the different lesions into 4 stages based on their biomechanical experiments: 3 subchondral impaction, partly detached fragment, nondisplaced free fragment, and fragment with 180-degree shift. Advancement of radiographic image technology enabled cystic lesions to be added to the Bernt and Harty classification. 16 In operative treatment for OLT, the operative procedure is determined by the stability of the lesion, the extent of cartilage damage, and the condition of the subchondral bone. According to this information, 1 of the following treatment strategies is selected: the bone marrow stimulation technique, fixation of osteochondral fragment, osteochondral bone graft from the knee joint, talar osteochondral allografting, or autologous chondrocyte implantation.12,14,21,23,27,28 Since it is important to diagnose the correct stage of the lesion, several studies evaluated the usefulness of MRI comparing MRI findings with arthroscopic findings directly.7,15,18 Although the usefulness of MRI to diagnose OLT was shown, MRI might overdiagnose or overestimate the extent of OLT due to bone edema. 8 Although MRI could evaluate the stability of the osteochondral fragment and revealed a good correlation with arthroscopic staging, MRI could not clearly detect the state of the articular cartilage surface because the articular cartilage of the ankle is 0.4 to 2.1 mm thick. 7 Computed tomography (CT) is also used to assess the stage of OLT. CT can provide information on the bone condition such as the size and shape, but it is not able to evaluate the articular cartilage in OLT. 9
In the pathogenesis of OLT, the importance of the subchondral bone plate was well discussed. The subchondral bone plate plays an important role in cartilage metabolism, which means that a damaged subchondral bone plate is not able to support the overlying cartilage, resulting in a subsequent loss of proteoglycans and glycoprotein.6,20 Trauma causes microfracture of the subchondral bone plate and it allows liquid flow into the subchondral bone. Continuous high fluid pressure induces osteolysis. Uozumi et al reported that the histology of initial change of osteochondral dissecans was bone necrosis, followed by absorption and replacement by viable subchondral trabeculae in the human knee. 24 Bone absorption due to high pressure liquid causes an unstable osteochondral fragment and enlargement of the cystic lesion. When bone absorption stops, bone remodeling occurs. This bone remodeling indicates hypermetabolism, which creates dense subchondral bone. 25 According to this evidence, focusing on the condition of the subchondral bone plate may be important in diagnosing OLT by CT, and we hypothesized that there may be a distinct relationship between the CT findings and arthroscopic findings, especially the state of cartilage damage. The purpose of this study was to evaluate the relationship between the arthroscopic findings including articular cartilage surface and the CT findings, focusing on the subchondral bone.
Methods
In the patients who had been diagnosed as having OLT between August 2004 to July 2013, 31 patients who met our inclusion criteria were included in this study. Twenty-five males and 6 females were included in this study, and their mean age was 28.9 years (range 14 to 59 years). Inclusion criteria comprised diagnosis as OLT radiologically and no ligamentous instability. Both CT and MRI were taken before surgery. OLT patients with a systemic disease such as rheumatoid arthritis were excluded from the study.
CT scans of the involved ankle were performed within 1 week before operative treatment in all patients. CT images in the coronal, sagittal, and axial planes were obtained with a multi director-row CT scanner (LightSpeed QX/I; General Electric Medical Systems, Milwaukee, WI, USA). The patient was placed in a supine, neutral position. Then, 3D volume data sets of the ankle were obtained. The scan parameter included a 512 × 512 matrix, 0-degree gantry tilt, 1.25-mm prospective slice thickness, 3.75 mm per rotation table speed (multi helical pitch of 3), 0.8-s gantry rotation, 120 kV (peak), and 120-200 mA. After this, 2-dimensional images were reconstructed with a 25-cm field of volume, 1.25-mm retrospective slice thickness, and 0.63-mm overlap. The total table motion was 30-40 cm, and finally 350-450 slices were obtained.
With a focus on the OLT’s subchondral bone, the CT images of all coronal, sagittal, and axial slices were observed. In the case of a bone fragment such as Bernt and Harty stage 3 or 4 classification, bone absorption or sclerotic change of the fragment, bone absorption or sclerotic change of the bed, were evaluated. In the case of a subchondral bone cyst, opening through the subchondral bone plate to the articular cavity, a round or irregular shaped cyst, and a sclerotic rim around the cyst were evaluated.
MRI scans were performed using a Signa 1.5-T device or a Signa HDxt 3.0-T device (GE Yokogawa Medical Systems Ltd, Tokyo, Japan) with a wraparound surface coil designed for the ankle. Proton density SE and T2-weighed SE images were collected. The conditions for the T2 weighed images were repetition time, 2600 ms; echo time, 98 ms; section thickness, 4.0 mm. Those for proton weighed images were repetition time, 2000 ms; echo time, 20 ms; section thickness, 4.0 mm. The OLT was classified according to the grading system by Anderson and Crichton: 1 0, normal; 1, subchondral trabecular compression and marrow edema; 2A, subchondral cyst; 2B, incomplete separation fragment; 3, unattached, nondisplaced fragment with synovial fluid surrounding it; 4, displaced fragment. All images of CT and MRI, as well as arthroscopic findings, were evaluated by 2 experienced orthopaedic surgeons independently.
All patients underwent arthroscopic surgery by 2 surgeons (NA and TN). They were placed in a supine position, and standard anterolateral and anteromedial portals were established under joint distraction using an Ankle Distractor (Smith & Nephew, Memphis, TN, USA). A 2.7-mm 30-degree oblique arthroscope was used. The arthroscopic evaluation was graded using the arthroscopic operative rating system by Ferkel and Cheng et al: A, smooth and intact, but soft and ballottable cartilage; B, rough surfaces; C, fibrillations or fissures; D, flap present or bone exposed; E, loose, undisplaced fragment; F, displaced fragment. 10 Moreover, the surface of the articular cartilage surface including osteochondral fragment and chondral flap was evaluated by the International Cartilage Repair Society (ICRS) grading system: ICRS grade 0, normal; grade 1, nearly normal: superficial lesions, soft indentation and/or superficial fissures and cracks; grade 2, abnormal: lesions extending down to <50% of cartilage depth; grade 3, severely abnormal: cartilage defects extending down >50% of cartilage depth as well as down to the calcified layer and down to, but not through, the subchondral bone; grade 4, severely abnormal: osteochondral injury, lesions extending just through the subchondral bone or deeper defects down into the trabecular bone. 5 CT and MRI findings were compared with the ICRS grade and arthroscopic operative rating system. Correlation between the duration of symptom and ICRS grade, and the differences between each type of CT findings and duration of symptom were statistically analyzed.
Statistical Analysis
Differences in accuracy between subgroups were tested for statistical differences with χ2 test. Statistical differences between the 3 groups were calculated using the Tukey–Kramer’s post hoc test. Spearman’s correlation coefficients were used to explore the relationship between the duration of symptoms and the ICRS grade. A P value of less than .05 was considered significant.
Results
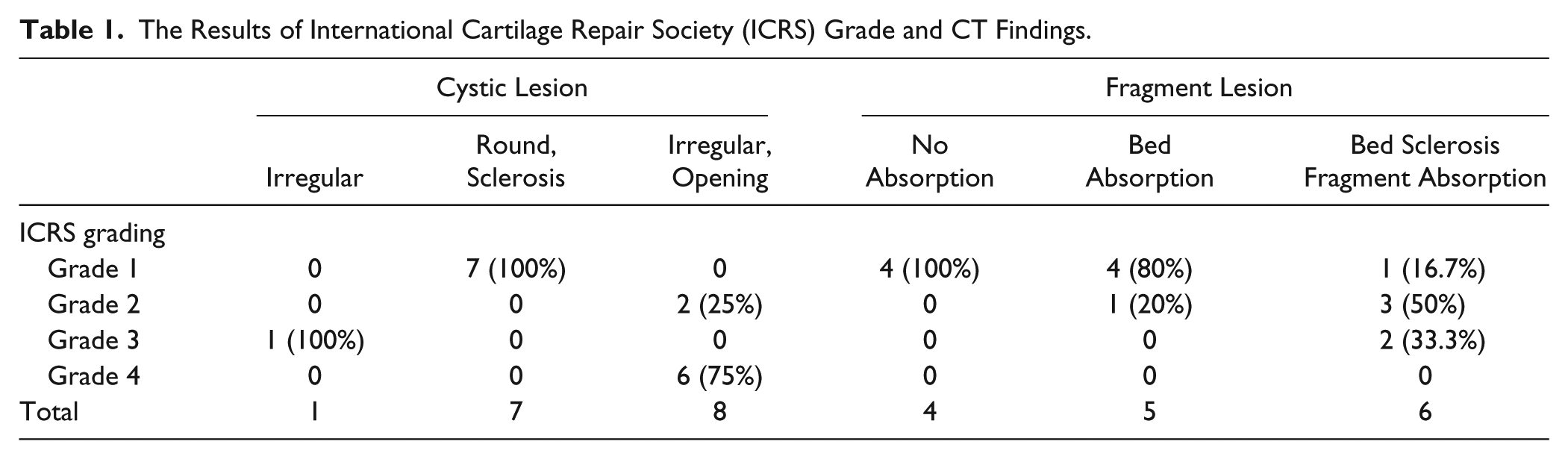
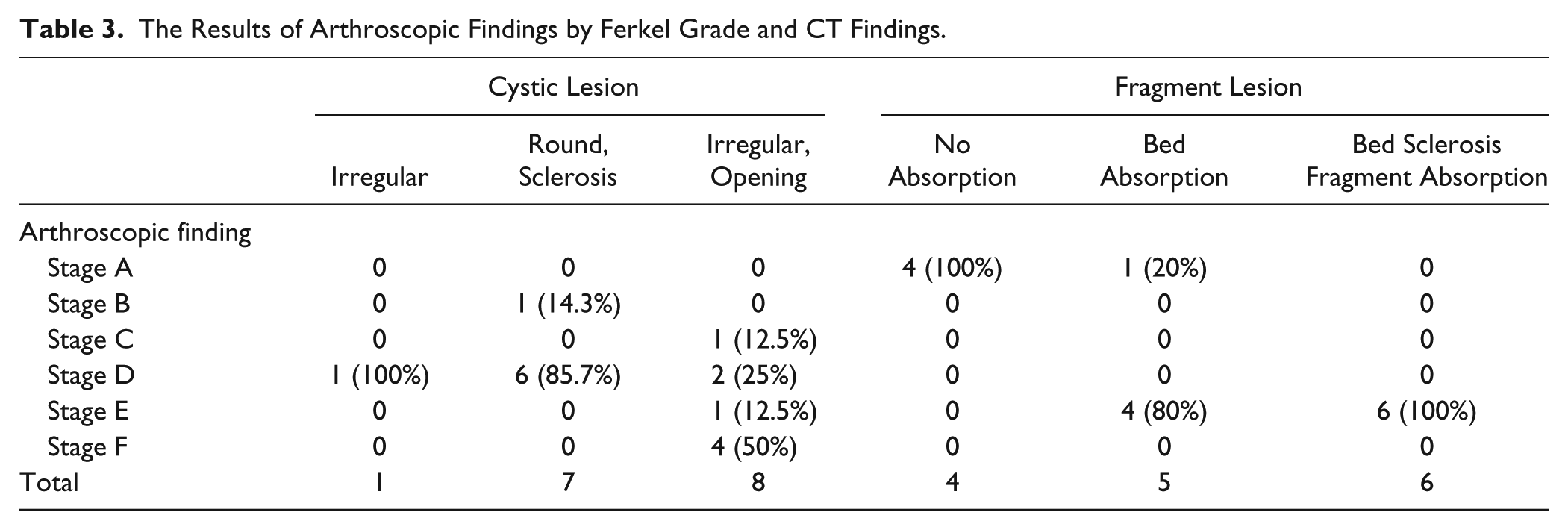
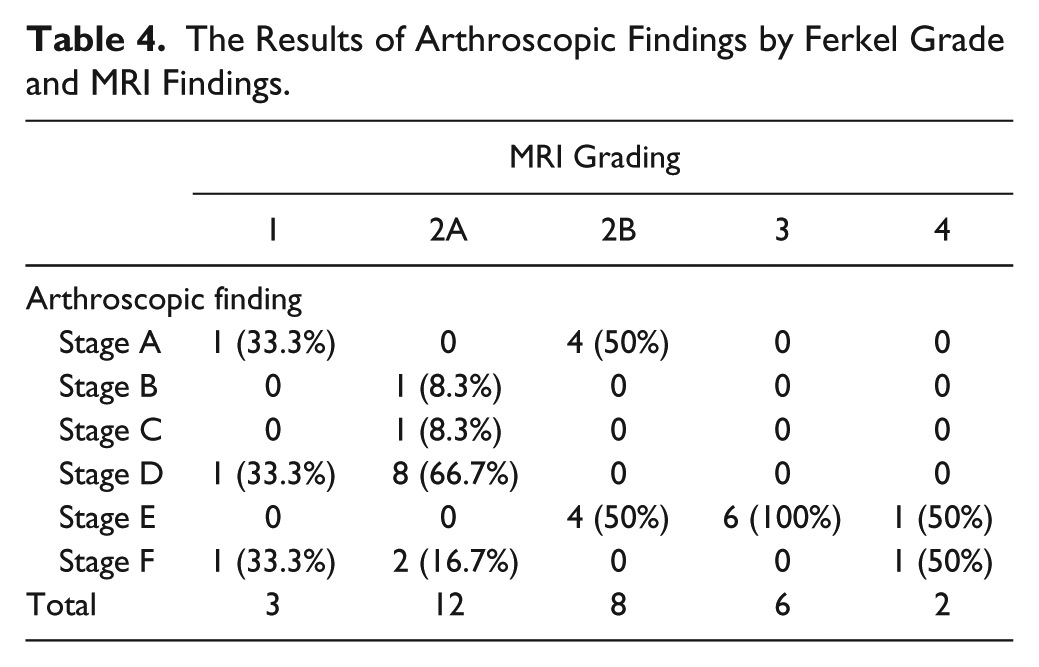
In the cystic lesion group (16 ankles), the CT findings were classified into 3 types: irregular (1 ankle), round sclerotic (7 ankles), and irregular opening (8 ankles). CT findings of bony fragment lesions (15 ankles) were classified into 3 types: no absorption (4 ankles), bed absorption (5 ankles), and bed sclerosis and fragment absorption (6 ankles; Figure 1). As for ICRS grade, all cases with round and sclerotic wall lesion (7/7 cases; 100%) and contact fragment with its bed (4/4 cases; 100%) revealed ICRS grade 1. Of the ankles with bed absorption, 80% also were ICRS grade 1. The irregular opening lesions consisted of 2 grade 2 cases (2/8 cases; 25%), and 6 grade 4 cases (6/8 cases; 75%). The results of relationship between ICRS grading and CT or MRI findings were shown in Tables 1 and 2. In arthroscopic findings by Ferkel’s classification, 85.7% ankles with round and sclerotic wall lesions (6/7 ankles) revealed stage D, 50% of irregular and opening cystic lesions (4/8 ankles) were Stage F, in fragment lesion, 80% ankles (4/5 ankles) with bed absorption were stage E, and all ankles with bed sclerosis and fragment absorption (6/6 ankles) were stage E. Tables 3 and 4 show the results between arthroscopic findings and CT or MRI findings.
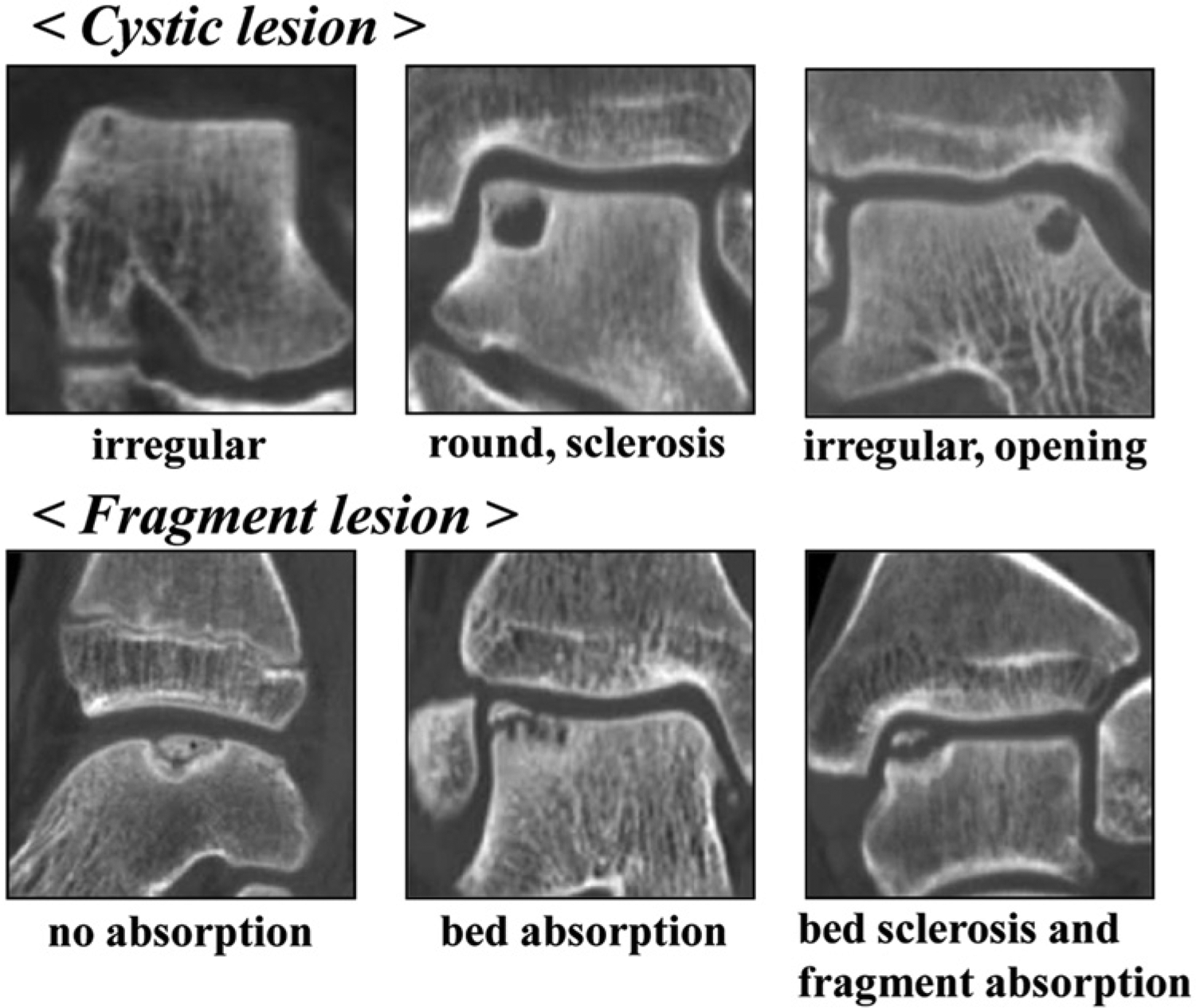
Classification of CT findings based on subchondral bone findings in osteochondral lesion of talus. Cystic lesion was classified into 3 types: irregular shape, round shape with sclerotic wall, and irregular shape with opening to articular cavity. Fragment lesion was also classified into 3 types: no absorption, bed absorption without fragment absorption, and bed sclerosis and fragment absorption.
The Results of International Cartilage Repair Society (ICRS) Grade and CT Findings.
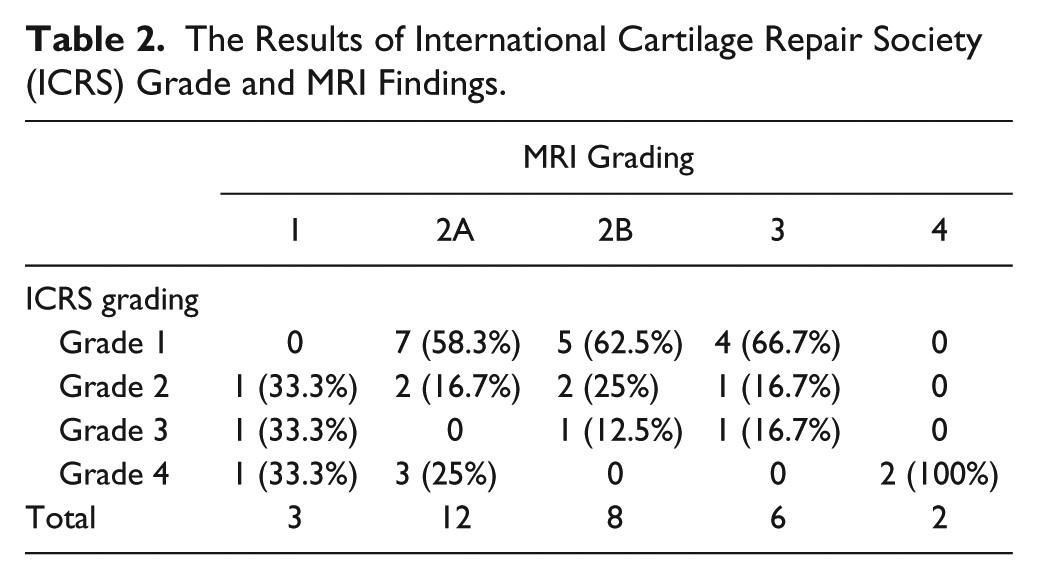
The Results of International Cartilage Repair Society (ICRS) Grade and MRI Findings.
The Results of Arthroscopic Findings by Ferkel Grade and CT Findings.
The Results of Arthroscopic Findings by Ferkel Grade and MRI Findings.
To summarize the cystic lesion group, round-shaped cystic lesions with sclerotic walls revealed cartilaginous flap lesions with a nearly normal cartilage surface. Irregular-shaped lesions, especially with an opening to an articular cavity, revealed unstable lesions with severely damaged cartilage. In the fragment lesion type, the cases where the fragment had contact with its bed revealed a stable lesion with a nearly normal cartilage surface. Bed absorption but no fragment absorption revealed an unstable lesion with a nearly normal cartilage surface. Fragment absorption with bed sclerosis showed an unstable lesion with severely damaged cartilage (Figure 2).
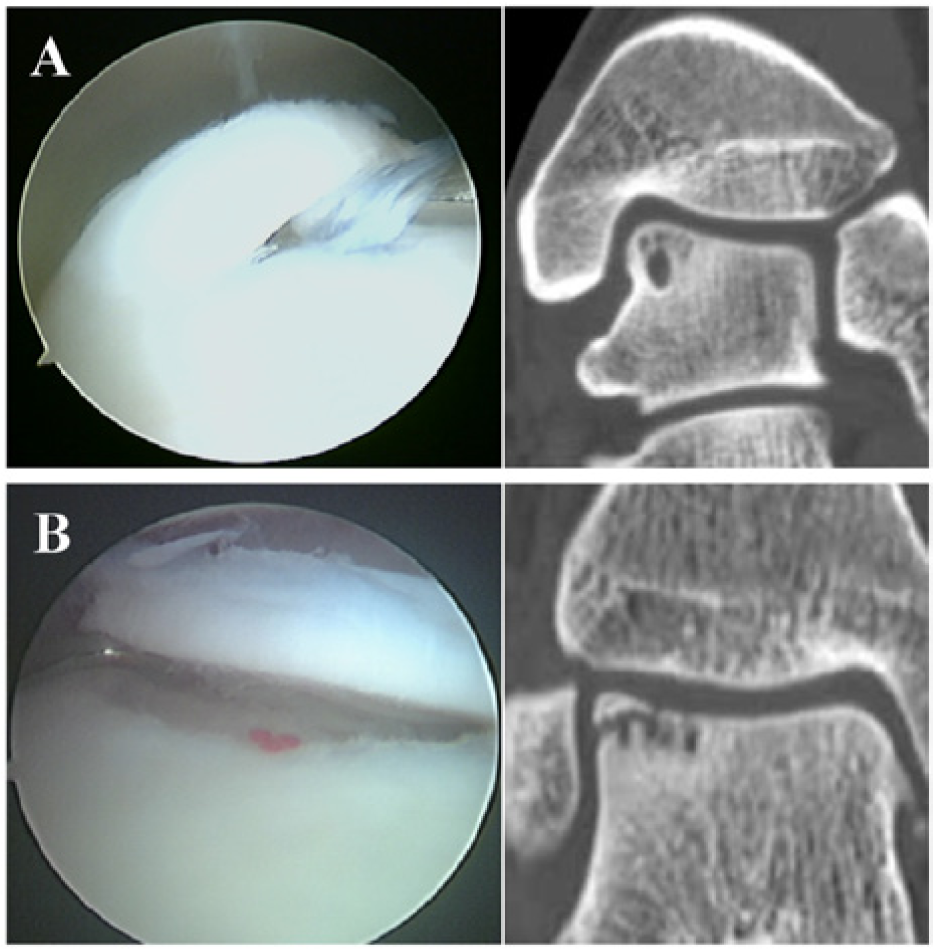
Representative cases in cystic and fragment lesions. (A) A case of cystic lesion. A 32-year-old man had right ankle pain for 7 months. The CT findings classified his lesion as being of round shape with a sclerotic wall. Arthroscopic findings showed ICRS grade 1 and stage D. (B) A case of fragment lesion. An 18-year-old man had right ankle pain for 4 months. CT findings classified his lesion as being that of bed absorption. Arthroscopic findings showed ICRS grade 1 and stage E.
Comparing the ICRS grade or arthroscopic findings to CT, χ2 test revealed that there was a significant difference (both P < .01). On the other hand, diagnosis by MRI revealed that there was no significant difference by χ2 test for ICRS grading and arthroscopic findings. These results indicated that classifying ICRS grading and arthroscopic findings using CT was superior to that by MRI.
The relationship between the CT findings and duration of symptoms was analyzed. There was no significant correlation between the duration of symptoms and the ICRS grade (r = .033, P = .43) in all cases. In both the cystic and fragment lesions, there was no significant difference of symptom duration between the types of CT findings.
Discussion
The current study has revealed that the CT findings, classified according to the condition of the subchondral bone, correlate to the arthroscopic findings. In the cystic lesion, the round shape with a sclerotic wall indicates that pressured fluid through the damaged subchondral bone plate no longer flows into the cyst, and bone remodeling occurs. Therefore, since the lesion did not advance, the subchondral bone plate could support the laying cartilage, which resulted in low graded articular cartilage. Monden et al evaluated 29 ankles with chondral fragment separated from the subchondral bone using CT, MRI, and arthroscopic findings. 19 In their reports, 6 large cysts, 9 micropores, and 7 honeycombs were existed in subchondral bone. Gathering of the microcysts leads to the honeycomb formation, which eventually evolved into a single large cyst. Therefore, these cystic subchondral bone lesion indicated that chondral fragment was separated from subchondral bone. On the other hand, an irregular shape with an opening to the subchondral bone plate through the articular cavity caused advancing bone resorption, which if prolonged induced a fragile subchondral bone plate, which could not maintain the metabolism of articular cartilage. Thus, this type of lesion showed severe articular damage. There was no significant difference in the duration of symptoms, therefore the difference between the long-term bone absorbing phase and the bone remodeling phase might influence articular cartilage damage and stability of the lesion.
In the lesion with an osteochondral fragment, the condition of the cartilage in the bone fragment group without bone absorption was almost intact, and the lesion was stable. This might be due to the fact that the lesion switched toward bone repair in the early phase, rather than to lasting bone absorption. A lesion with bone absorption in its bed suggested that bone resorption in its bed by constitutive fluid pressure caused an unstable lesion, but no bone absorption of the fragment could maintain cartilage metabolism. Thus, this type lesion revealed an unstable lesion but a good cartilage condition. A lesion with bone absorption of the fragment and sclerosis of its bed revealed an unstable lesion and severe cartilage damage. A fragment with bone absorption no longer maintained normal cartilage metabolism, and mechanical stress by an unstable lesion also caused severe cartilage damage. Sclerotic lesions of the bed indicated bone remodeling, but it was largely focused on bone metabolism, which could not expect bone union between the fragment and its bed during a natural course of events.
The accuracy of MRI for staging OCL of the talus ranges from 65.9 to 92%.2,7,15,18 Although the correct cartilage staging is important to determine the treatment options, MRI is limited to the evaluation of cartilage stability. 22 Bae et al 2 reported a relatively low correlation rate of MRI staging for OLT because arthroscopic grade C lesions could not be diagnosed due to thinness of the articular cartilage. In our results, the correlation rate was low except for grade 3 lesions. Previous reports mentioned that it was difficult to evaluate precisely the status of the articular cartilage on MRI because of its thinness.15,18 CT has been also applied for evaluation of OLT, but it could not assess the cartilage condition. Its advantage is to obtain bony information such as precise size, shape, and displacement. 9
In cartilage injury including OCL and osteoarthritis, it has become clear that the changes to the subchondral bone plate affect disease progression.4,13 Therefore, there should be a correlation between cartilage injury and subchondral bone. The present study showed that the evaluation of subchondral bone using CT is a useful tool for predicting the state of cartilage injury. Verhagen et al 26 reported that there was no significant difference between helical CT and MRI for diagnosis of OLT. MRI diagnosis associated with information on the state of subchondral bone on CT would be more useful for diagnosis of OLT including damage of the cartilage surface. Recently, the usefulness of SPECT-CT for the additional information in diagnosing OLT was reported. 17 As for MRI, Griffith et al 11 demonstrated that high-resolution MRI of talar osteochondral lesions could depict clinically pertinent features not detectable with standard MRI. These new technologies combined with the subchondral bone appearance in OLT would allow more accurate diagnosis of OLT.
One of the limitations of this study is that the number of patients is small. It should be investigated whether more patients enrolled in this study would affect the results of this study or not. Second, it is unclear that the extent and/or mechanisms of the initial injury might affect the relationship between the CT findings and cartilage status in the current study. Finally, histopathology of subchondral bone was not confirmed because the biopsy for osteochondral lesion was not performed. Further studies to clarify not only the relationship between the histological findings of osteochondral lesion and CT findings of subchondral bone but also the influence of osteochondral damage at initial injury will be needed for validation of the results in this study.
In conclusion, CT findings on OLT based on the state of the subchondral bone correlated to the damage of cartilage and stability of the lesion. MRI was useful for the assessment of OLT staging, but it was difficult to evaluate the cartilage surface condition. This study suggests that CT reinforces the MRI capability, resulting in a precise diagnosis for OLT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.