
Abstract
Background:
Lateral ankle sprain is one of the most common injuries. Since the structural and pathological differences in mechanical ankle instability (MAI) and functional ankle instability (FAI) may not be the same, it may be better to treat these as separate groups. The purpose of this study was to compare the difference in postural sway between MAI and FAI in patients with chronic ankle instability (CAI).
Methods:
Twenty-six patients with CAI and 14 healthy control participants were included in the study. The CAI patients were subdivided into MAI (15 patients) and FAI (11 patients) groups. Patients who were diagnosed with lateral ankle ligaments rupture by magnetic resonance imaging and ultrasonography were assigned to the MAI group. All participants performed single-limb postural sway tests 3 times on each leg with eyes closed and open. The average distances from the mean center of pressure position in the mediolateral and anteroposterior directions were recorded and compared among the 3 groups.
Results:
The unstable ankles in the MAI group showed significantly greater postural sway in the anterior, posterior, and medial directions compared with those in the control group with eyes closed. With eyes open, significantly greater postural sway was found in the anterior direction. In the FAI group, no difference was found in postural sway compared with those in the control group. The MAI group showed significantly greater postural sway in the anterior direction compared with the FAI group with eyes closed and open. No significant difference in postural sway was found between the unstable and stable ankles in the MAI or FAI groups, with or without vision.
Conclusions:
Patients with MAI have deficits in postural control, especially in anterior-posterior directions. However, no difference was found in postural sway in patients with FAI compared with healthy people.
Clinical Relevance:
As MAI patients suffer from deficits in postural control, balance training should be applied in those patients. In addition, special training should also include the contralateral side after a unilateral ankle ligament injured.
Acute lateral ankle sprain is one of the most common injuries, and more than 20% of such patients have persistent symptoms and chronic instability of the ankle,36,37 which may lead to repetitive ankle sprains. Chronic ankle instability (CAI) may be caused by mechanical ankle instability (MAI), functional ankle instability (FAI), or a combination of the two. Mechanical ankle instability is defined as laxity and excessive joint motion of the ankle joints caused by structural damage of the supporting ligamentous tissues, which may need operative treatment. Besides the pathologic laxity, arthrokinematic restrictions, synovial irritation, or degenerative changes to the ankle joint also may be found in patients with MAI. 21 In contrast, FAI does not exhibit any physical laxity of the ankle joints. 21 In 1965, Freeman et al 13 first described the concept of FAI, which has the tendency for the foot to “give way” after an ankle sprain. 13 The instability may be caused by specific insufficiencies in proprioception, neuromuscular control, postural control, or muscle strength, 21 which were mainly treated by physiotherapeutic rehabilitation. 25
Functional ankle instability has been associated with several functional insufficiencies around the ankle. The most common balance parameter detected in patients with FAI is an increased area of postural sway in the injured ankle during a single-limb standing test. 20 Freeman et al 13 believed that poor postural control performance has been associated with lateral ankle instability. Moreover, deficit in postural sway indicated the risk of ankle reinjury was increased. 33 However, in previous studies, contradicting evidence exists for the changes in postural stability deficits in the single-leg stance following FAI.1,2,9,12,34,42 Inconsistent results may be partially because the authors did not divide individuals into MAI or FAI groups. Since the structural and pathological differences in MAI and FAI may not be the same, various functional insufficiencies may exist between patients with MAI and FAI. Identifying the intrinsic ankle characteristics and restoring these insufficiencies can reduce the risk of ankle reinjury, which has become an important consideration to the clinician, 45 and it may be better to treat these as separate groups. 4
In this study, our aim was to separate CAI by mechanical or functional instability and compare the difference in postural control between MAI and FAI. One of our hypotheses was that patients with MAI may have deficits in postural control. The second hypothesis was that a difference in postural control may exist between patients with MAI and FAI, which would indicate that different treatment strategies may be needed in these patients.
Methods
Participants
Forty people (14 healthy participants, 26 CAI patients) took part in the study, which was approved by the authors’ university research ethics committee. The patients with CAI were subdivided into MAI and FAI groups. Therefore, the participants were assigned to 3 groups: 11 in the FAI group, 15 in the MAI group, and 14 in the healthy control group. The 3 groups were well matched for age, sex, height, and weight (Table 1). The most common symptom in patients with FAI was the feeling of “giving way” when walking on uneven ground after ankle sprain. Moreover, other factors, including the severity of the initial ankle sprain, the frequency of ankle sprains that occurred, and the influence on daily activities and sports, should be considered when FAI is defined. 30 In previous studies, various self-reported questionnaires were frequently used to quantify these factors and objectively identify patients with ankle instability for diagnosing FAI (Table 2), and 2 were used in our study.
Participant Characteristics.
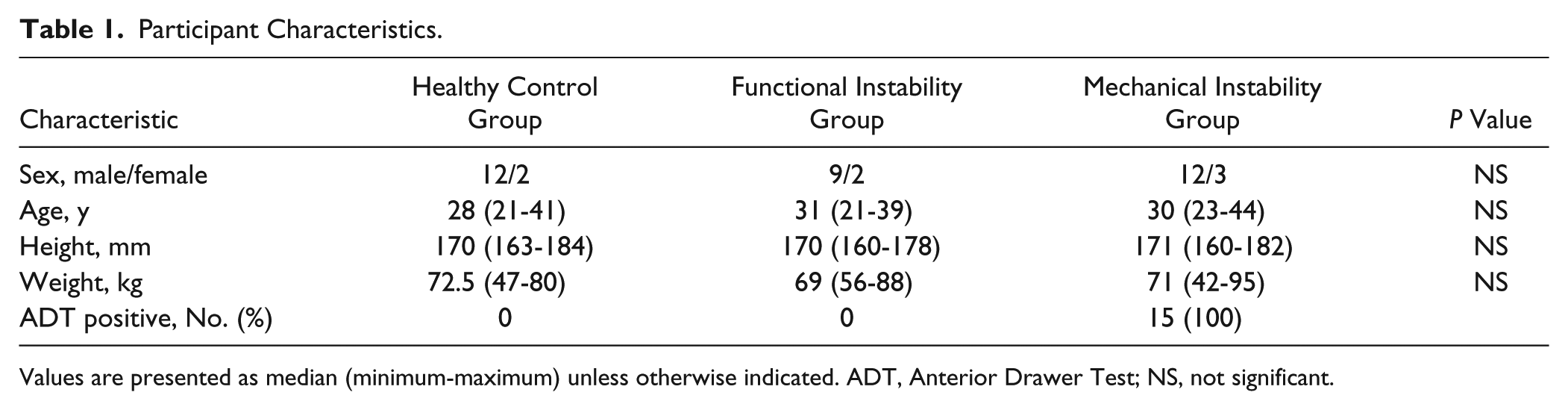
Values are presented as median (minimum-maximum) unless otherwise indicated. ADT, Anterior Drawer Test; NS, not significant.
Instruments to Determine Patients With CAI or FAI.
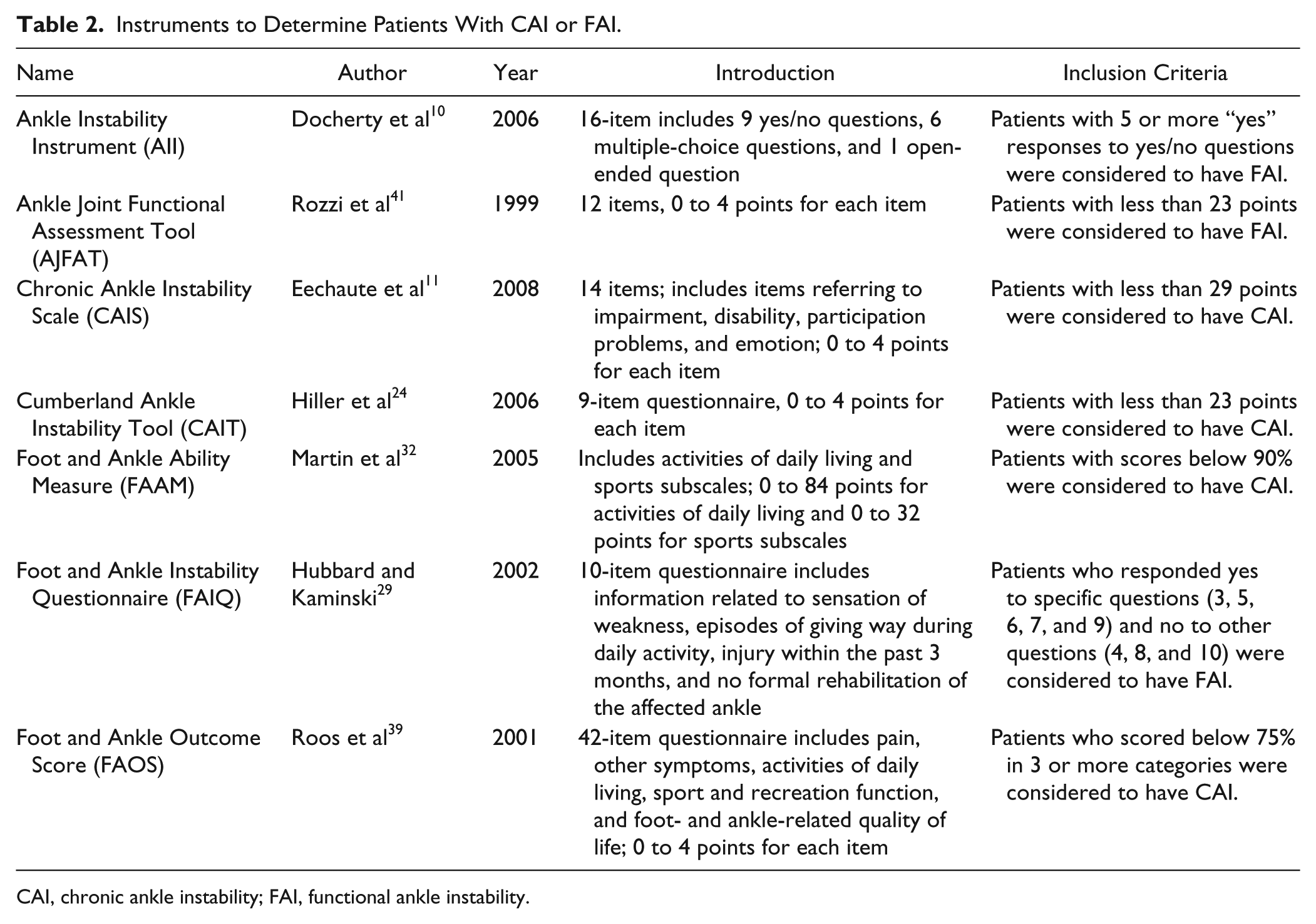
CAI, chronic ankle instability; FAI, functional ankle instability.
The patients assigned to the FAI group had a history of at least 1 unilateral ankle sprain, with the original injury occurring at least 12 months prior to the study, and met the criteria set forth by the Functional Ankle Instability Questionnaire 29 and Ankle Instability Instrument 30 (Table 2). Moreover, any patient identified with lateral ankle ligament injury by magnetic resonance imaging (MRI) or ultrasonography was excluded from the FAI group.
The patients identified with lateral ankle ligament (including anterior talofibular ligament [ATFL] and/or calcaneofibular ligament [CFL]) injuries were assigned to the MAI group. Moreover, a history of at least 1 unilateral ankle sprain, with the original injury occurring at least 12 months before the study, and physical examination of the positive anterior drawer sign were the inclusion criteria for patients with MAI.
The exclusion criteria for patients with FAI and MAI included previous injury or surgery to the lower limb, balance or motion disorder, cavus feet, tendon injury in the lower leg or ankle, required use of foot orthotics, any open wounds on the foot, and osteochondral lesions. 34 The control group was free from any history of ankle sprains and any criteria for exclusion.
Mechanical Stability Measures
Ultrasonography
The ultrasonography examination was performed by a senior radiologist using an ALT HDI 5000 US unit (Philips Medical Systems, Bothell, WA). Patients were placed in a supine position with the ankle passively placed in a maximal inversion and plantarflexion position. A wide-frequency linear array transducer with center frequencies of 5 to 17 MHz was used. The contralateral lateral ankle ligaments were also examined. The ultrasonography criteria for ligament injury were (1) ligament tear: partial or total interruption of the ligament fibers at the insertion or in the midsubstance; (2) ligament laxity: the ligament remained curved when the ankle was in maximum inversion and plantarflexion; (3) ligament thickening: the width of the ligament was 2.4 mm or >20% of the contralateral normal ligament; (4) ligament absorption: no ligament fibers were seen; and (5) nonunion of avulsion fracture of the lateral malleolus. 26
MRI
Magnetic resonance imaging was performed with a 1.5-T HD twin-speed magnetic resonance scanner (Signa; GE Medical Systems, Milwaukee, WI) using a 20-cm extremity coil. The feet of the participants were placed in the neutral position. The axial, sagittal, and coronal planes were obtained. A section thickness of 3 mm was used. The examination protocol consisted of transverse T2-weighted (repetition time/echo time: 4000/96; matrix: 256 × 256; echo train length: 8) fast-spin-echo sequences. The field of view was 10 cm in all examinations. The diagnostic criteria for determining a ligament injury were as follows: (1) discontinuity, (2) wavy or curved contour, and (3) increased signal intensity within the ligament. The diagnosis of ligament injuries was made upon fulfillment of any one of these criteria. 35
Instrumentation
All participants were assessed for postural sway on a Kistler force plate (Model 9284; Kistler Instruments AG, Winterthur, Switzerland). Postural sway was defined as the deviation from the mean center of pressure (COP) of the foot for a given trial. 18 During a single-leg standing test, the deviation from the mean COP was calculated as the most frequently detected parameter during postural control assessments in sports medicine settings. 38 The average distances from the mean COP position in the mediolateral (x) and anteroposterior (y) directions were recorded during quiet standing on the force plate for 10 seconds. 30 Each participant performed 3 tests on each leg with and without vision, with a 2-minute rest between the tests. Under the 2 conditions, the participants were asked to stand with 1 leg as still as possible, the arms were held loosely by the sides, and the contralateral knees were in flexion at a 45-degree angle. Shoes were not worn. The standing foot was placed on a longitudinal reference line on the platform extending from the first space between the big and second toes and the center of the heel. During the tests with vision, the participants were asked to focus on a point at eye level on the opposite wall. During the tests without vision, the participants were asked to close their eyes when ready. 34 This method used in the single-limb standing test has been judged to be reliable. 34 Moreover, the advantage of the static balance test is that it is easier to perform and safer than dynamic tests, and some tests can be performed outside a laboratory. 25
If the participant touched down with the opposite limb, made contact with the stance limb, or was unable to maintain the standing posture during the 10-second trial, the trial was terminated and repeated. 30
Mediolateral and anteroposterior postural sways were calculated by summing the 2 sway components on a particular axis. The absolute +x and −x components were added to provide the mediolateral total, while the absolute +y and −y components formed the anteroposterior total. 34
Statistical Analysis
An a priori power analysis was used to calculate the sample sizes. An accepted effect size of 0.5, α of 0.05, and 1 – β of 0.95 required a minimum sample size of 9 participants in each group. 8 In the control group, the left and right sides were randomly assigned as “affected” and “unaffected.” Due to the skewed distributions and the heterogeneity of variance among the 3 groups, data were presented as median and range and analyzed using nonparametric tests. Comparisons among the 3 groups were performed by the Kruskal-Wallis test, except for the comparison regarding sex distribution, which was analyzed with the Pearson χ2 test. Post hoc analyses between groups were carried out with the Mann-Whitney U test. A matched pair design using the Wilcoxon signed-rank test (with a median of 0) was used to detect the differences in balance measures between the affected and unaffected ankles within groups. Differences were considered statistically significant for values of P < .05. All statistical analyses were conducted using SPSS 19.0 (SPSS, Inc, an IBM Company, Chicago, IL).
Results
Fifteen patients in the MAI group were diagnosed with lateral ankle ligament injury by MRI and ultrasonography. Ultrasonography revealed the following: 6 cases of tear of the ligaments (Figure 1), 2 cases of relaxation of the ligaments, 2 cases of thickening of the ligaments, 3 cases of absorption of the ligaments, and 2 cases of avulsion fracture. Magnetic resonance imaging revealed the following: 9 cases of discontinuity of the ligaments (Figure 2), 4 cases of wavy or curved contour, and 2 cases of increased signal intensity within the ligaments.
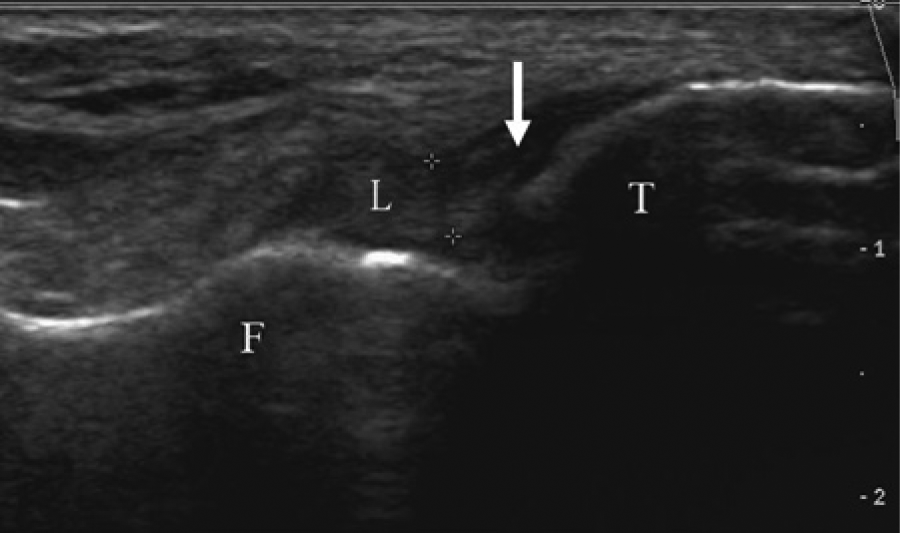
Ultrasonography examination for the lateral ankle ligaments. Sonogram shows a ligament tear at the insertion on the talus. The ligament is curved and the insertion on the talus is interrupted (white arrow). The upper and lower boundary of the ligament is marked by the 2 crosshairs. 1 and −2 on the right-hand side describe the distance of the tissue relative to the probe. 1 and 2 mean the distance of the tissue relative to the probe is 1 and 2 cm, respectively. F, fibula; L, anterior talofibular ligament; S, skin surface; T, talus.
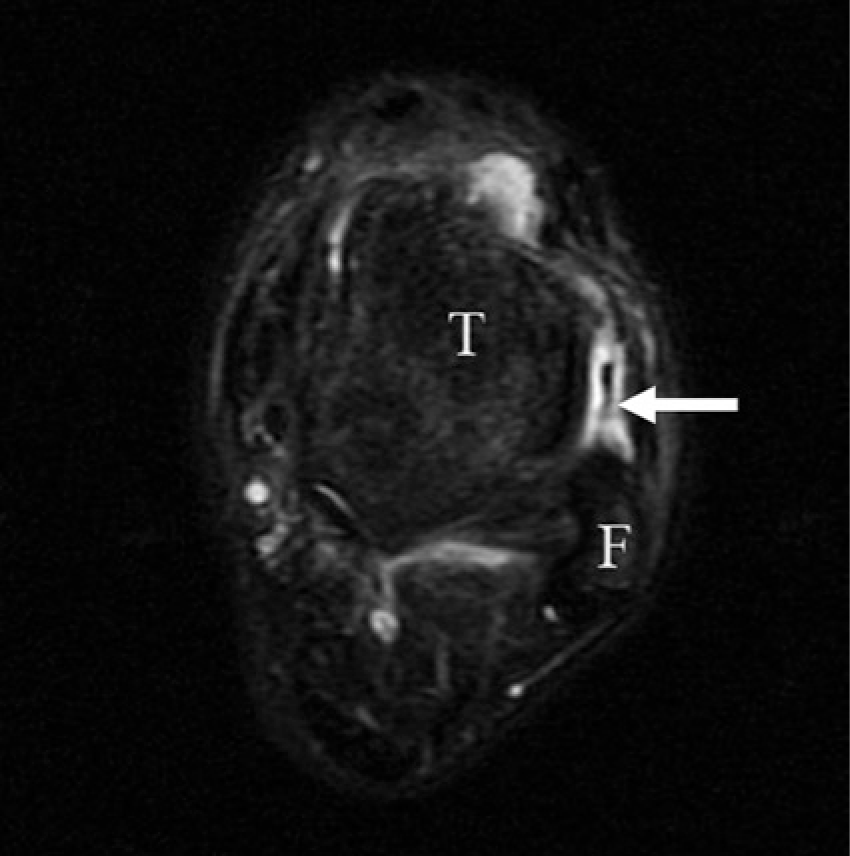
Magnetic resonance imaging examination for the lateral ankle ligaments. Complete tear of the anterior tibiofibular ligament on an axial T2-weighted image is seen as a discontinuous ligament (white arrow). F, fibula; T, talus.
In the MAI group, several significant differences were found in postural sway. The unstable ankles in the MAI group had significantly greater postural sway compared with those in the control group in the anterior, posterior, and medial directions with eyes closed (Table 3). With eyes open, significantly greater postural sway was found in the anterior direction (Table 4). Moreover, the stable ankles in the MAI group had significantly greater anterior postural sway with eyes closed (Table 3) and increased medial postural sway with eyes open (Table 4). In addition, the MAI group demonstrated significantly greater postural sway in the anterior direction compared with the FAI group with eyes closed (Table 3). With eyes open, significantly greater postural sway was found in the medial direction compared with the FAI group (Table 4). No significant difference in postural sway was found between the unstable and stable ankles (Tables 3 and 4).
Results of the Postural Sway Test (Without Vision).
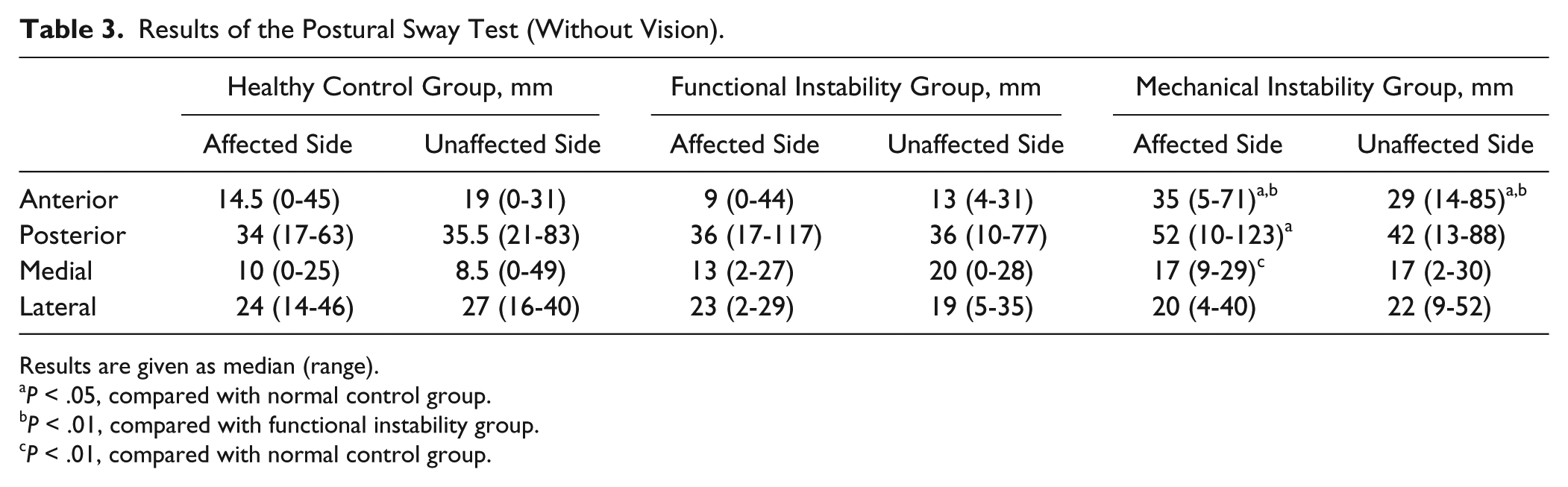
Results are given as median (range).
P < .05, compared with normal control group.
P < .01, compared with functional instability group.
P < .01, compared with normal control group.
Results of the Postural Sway Test (With Vision).
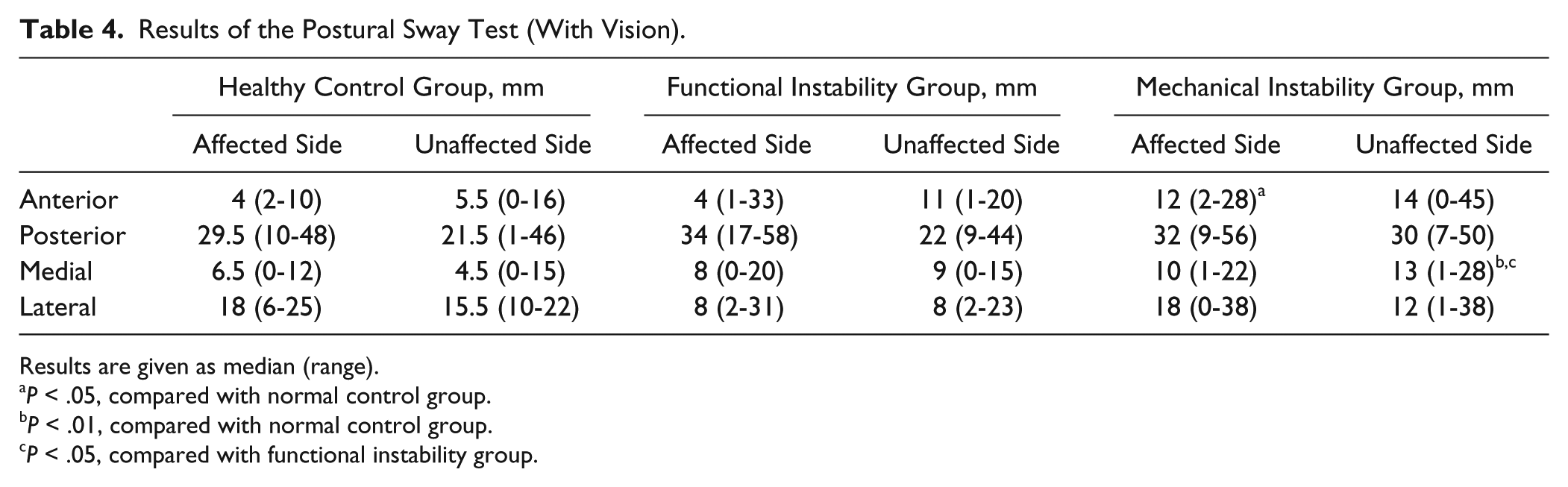
Results are given as median (range).
P < .05, compared with normal control group.
P < .01, compared with normal control group.
P < .05, compared with functional instability group.
In the FAI group, no significant difference in postural sway was found in either the anteroposterior or mediolateral plane compared with those in the control group (Tables 3 and 4).
Discussion
A previous study indicated that several individual components contribute to postural control, including proprioception, postural reflexes, muscle strength, nerve conduction velocity, and joint range of motion. 38 Although FAI was thought to be caused by specific insufficiencies in postural control in Freeman’s option, contradicting evidence exists for changes in postural stability deficits.1,2,9,12,34,42 In our study, no difference was found in the FAI group in postural control compared with those in the health control group. The reasons for these discrepancies in postural stability studies are unclear. One potential reason could be the variation in functional performance tests chosen to elicit functional performance deficits. 42 Another reason may be that the inclusion criteria for FAI were inconsistent in previous studies, and most have not separated chronically unstable patients by mechanical or functional instability. Moreover, mechanical instability was identified by manual stress tests and stress radiography.2,43 However, the reliability and validity of manual stress tests and stress radiography in diagnosing lateral ankle ligament injury have been questioned.14,15 In this study, the patients with CAI were subdivided into FAI and MAI groups by ultrasonography and MRI, which demonstrated satisfactory diagnostic accuracy for lateral ankle ligament rupture.26,35 Any patient diagnosed with lateral ankle ligament injury was excluded from the FAI group, thereby meeting the definition that FAI does not exhibit any laxity of the talocrural, subtalar, and/or inferior tibiofibular joints. 21
In patients with MAI, the most common mechanical change is hypermobility after ankle sprains, which refers to laxity of the ankle joint.23,28 Increased postural sway was found in patients with MAI, indicating that the deficit in postural control was related to the laxity of the ankle. The possible reasons include the following: first, an increase in the accessory motion of an ankle joint indicates enlargement of the neutral zone of the joint, which will increase the area of postural sway. 28 Previous studies demonstrated improvement of postural control following use of ankle supports,1,19 which can significantly decrease the mechanical laxity in patients with CAI. 27 Second, the presence of decreased mechanical ankle-joint stability might require higher levels of ankle-muscle coactivation to maintain the joint in optimal alignment and may therefore influence the execution of motor strategies concerned with maintaining balance. 38 Finally, the role of ligamentous mechanoreceptors in balance control and joint position sense has been questioned. In the study by Hertel et al, 22 anesthesia of the lateral ankle ligaments failed to result in significant alterations in postural control, suggesting that an adaptive mechanism occurred after anesthesia to compensate for the loss of mechanoreceptor input from the lateral ankle. As a result, intact lateral ankle ligaments could be more important than mechanoreceptors in postural control. Our results showed that the unstable ankles in the MAI group had greater postural sway in the anterior-posterior directions. The reason may be that the injured ATFL could not limit anterior and posterior movement of the tibia on the talus, which may increase the anterior-posterior movement 4 ; therefore, greater postural sway may be detected.
In this study, we did not find any significant differences in balance performance in the FAI group. The reason may be that, since the joint mechanoreceptors are only active near the end range of motion, 44 a single-leg standing test as used in our study is not sensitive enough to find any postural deficit in patients with FAI because it is a relatively static task. Thus, a more dynamic method may be necessary for neural discharge of joint mechanoreceptors to diagnose these patients. 44
In this study, no significant difference in postural sway was found between unstable and stable ankles in patients with MAI. These results are consistent with previous studies.2,12,34,40 One of the reasons may be that the stable and unstable ankles were using the same processes to maintain postural sway or that the unstable ankles compensated for any existing deficits with either increased reliance on other sensory systems or increased reliance on muscles for postural control. 34 Another reason may be that some insufficiency problem may be appearing in the contralateral ankle after the occurrence of unilateral CAI. In a 7-year follow-up study, problems such as pain, swelling, and ankle sprain were reported in the contralateral ankle of 85% of people who developed CAI after a unilateral sprain. 31 A third reason may be the presence of alterations in hip extensor activity in both the injured and uninjured limbs after severe unilateral ankle sprains. 3 These proximal alterations may be related to increased stress on the ankle joint during jump landing 5 and insufficient postural control. 17
Previous research indicated that poor postural control was associated with increased risk of ankle sprain. 33 Because our study found that MAI and FAI had different findings in balance control, it may be important to separate these subtypes in future research studies. In addition, clinicians may need to develop alternate rehabilitation parameters to address these differences. For example, we found that patients with MAI had greater postural sway, especially in anterior-posterior directions. Since the use of balance and coordination training can prevent ankle instability, especially in those with a history of ankle sprains,25,33 it is reasonable to suggest that balance training should be applied regardless of whether a patient with MAI undergoes operative treatment. In addition, because of the insufficient postural control in the contralateral ankle, special training after an ankle ligament lesion should also include the contralateral side.
In recent years, there has been increasing attention to the difference of functional insufficiency between MAI and FAI.6,7,16,18 However, to our knowledge, our study is the first to specifically examine the difference of MAI and FAI in postural sway. The limitation of this study was that as a retrospective, cross-sectional study, episodes of instability were self-reported and may not have been accurate. Therefore, to compensate for this, we used MRI and ultrasonography to reveal ankle lateral ligament injury in the MAI group.
Conclusion
Our results revealed that patients with MAI had increased postural sway compared with that of patients with FAI and healthy people, especially in the anterior-posterior direction. However, no difference was found in postural control in patients with FAI compared with that of healthy volunteers. As MAI patients suffer from deficits in postural control, balance training should be applied in those patients. In addition, special training should also include the contralateral side after a unilateral ankle ligament injured.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant awarded to Ying-Hui Hua from the National Natural Science Foundation of China (NSFC81101391).