
Abstract

Keywords
Several percutaneous lateral ankle ligament reconstruction techniques have been introduced for the treatment of chronic lateral ankle instability with local ligamentous tissue so severely attenuated or deficient that direct repair would be expected to have a poor outcome.4,7,11,12 Percutaneous Chrisman-Snook lateral ankle ligament reconstruction using half of the peroneus brevis tendon has been introduced. 7 However, disturbing the peroneus brevis, the primary evertor and dynamic lateral ankle stabilizer, can be a drawback.1,5,6 An allograft tendon can be used in percutaneous reconstruction. 12 However, the associated high cost and possibility of an immunogenic response is a concern. 3 A minimally invasive lateral ankle ligament reconstruction technique using a semitendinosus autograft was recently introduced. 11 However, harvesting the semitendinosus tendon may not be easy for foot and ankle surgeons who are not familiar with the knee anatomy. Precutting of the tendon can occur because of the juncturae connected to the tendon. Inadvertent saphenous nerve injury during the harvesting procedures may result in numbness around the harvest site. 9 We developed a technique using a split half of the peroneus longus tendon as a free autograft for the percutaneous lateral ankle ligament reconstruction. The free graft can be easily harvested from 1 of the percutaneous incisions for reconstruction in the same position as that of the ligament reconstruction. The percutaneous technique offers better cosmesis with less scarring than a standard open procedure.
Operative Technique
The patient is placed in a semilateral or lateral position that is usually used for lateral ankle ligament reconstruction. To harvest a split half of the peroneus longus tendon, a 1-cm longitudinal incision is created on the posterior margin of the lateral malleolus 2 cm proximal to the distal tip. The peroneus longus tendon, which can easily be identified superficial to the peroneus brevis tendon, is then carefully pulled out of the incision (Figure 1A). Since the peroneus longus tendon inserts into the base of the first metatarsal, it plantarflexes the first metatarsal when tension is applied. After cutting and splitting the anterior half of the tendon, the distal end is sutured with a Krackow whip-stitch (Figure 1B). The route of the tendon can be distinguished over the skin by pulling the tendon through the incision. A 1.5-cm transverse incision is created over the peroneus longus tendon 10 cm proximal to the initial incision. The proximal portion of the peroneus longus tendon is pulled out from the second incision with a mosquito clamp to keep it under tension. A 5-mm tendon stripper (Arthrex Inc, Naples, FL) is then introduced over the anterior portion of the peroneus longus tendon through the initial incision and pushed proximally (Figure 1C). When the tendon stripper reaches the second incision, the anterior split of the peroneus longus tendon is pulled out of the incision and the tendon stripper is retrieved (Figure 1D) yielding a 10-cm free tendon graft.
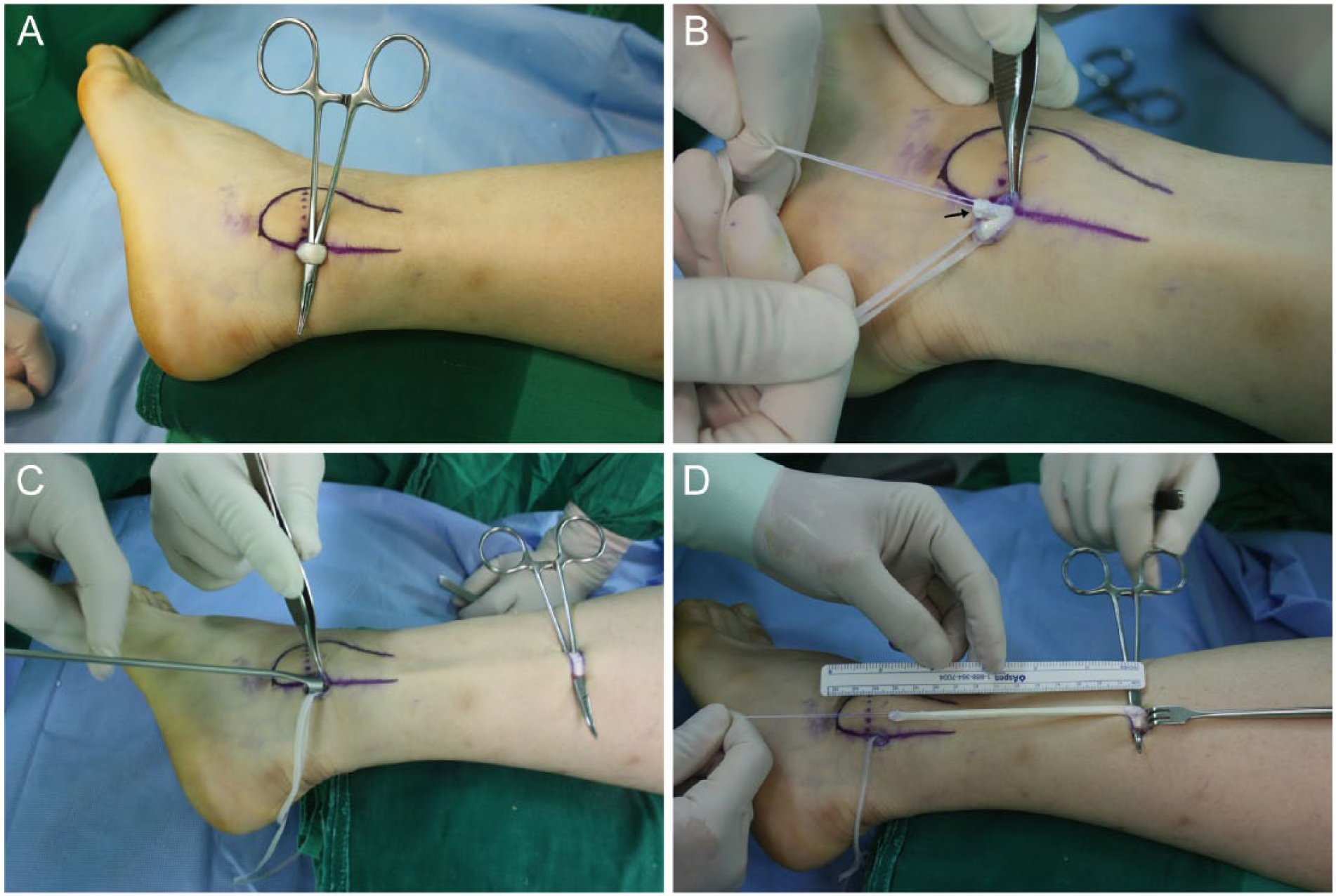
(A) Peroneus longus tendon is pulled out of an incision created on the posterior margin of the lateral malleolus 2 cm proximal to the distal tip. (B) The peroneus longus tendon is split in half and a Krachow whip-stitch is woven into the end of the anteriorly split tendon (indicated with an arrow). (C) A tendon stripper is pushed proximally over the anterior split of the tendon while the distal end of the tendon is pulled to keep the tendon under tension. (D) The anterior split of the tendon is pulled out of the second incision that was created 10-12 cm proximal to the initial incision. A 10-cm free tendon can be harvested for the lateral ankle ligament reconstruction.
Without changing the patient’s position, a fibular bone tunnel is made using a 4-mm drill bit in a posterior-to-anterior direction through the incision made for the tendon harvest under fluoroscopic guidance. A percutaneous small incision is made just anterior to the fibular bone tunnel. Under fluoroscopic guidance, a guide wire is inserted at the anterior margin of the talar body, at the attachment of the anterior talofibular ligament (ATFL). A percutaneous small incision is made and a talar bone tunnel 5 mm in diameter and 20 mm deep is made over the guide wire. The harvested tendon is then passed through the fibular bone tunnel in a posterior-to-anterior direction using the posterior incision created for the tendon harvest and is pulled out through the percutaneous incision just anterior to the fibular bone tunnel. An eyelet needle or a loop wire is then used to guide the tendon to the percutaneous incision at the talar bone tunnel and the tendon is fixed into the talar tunnel at the ATFL attachment area using a 4.75-mm bioabsorbable interference screw (Arthrex Inc, Naples, FL) to reconstruct the ATFL (Figure 2, 3A). A 10-mm incision is made over the lateral calcaneal wall where the calcaneofibular ligament (CFL) attaches, and a 5.0-mm calcaneal tunnel is created. The posterior end of the autograft tendon is then passed downward over the peroneal tendons. The autograft tendon is inserted into the calcaneal tunnel from lateral to medial and is tensioned with the ankle in the plantigrade position and the subtalar joint in a neutral position. A 6.25-mm bioabsorbable interference screw (Arthrex) is inserted to reconstruct the CFL (Figure 2, 3B).
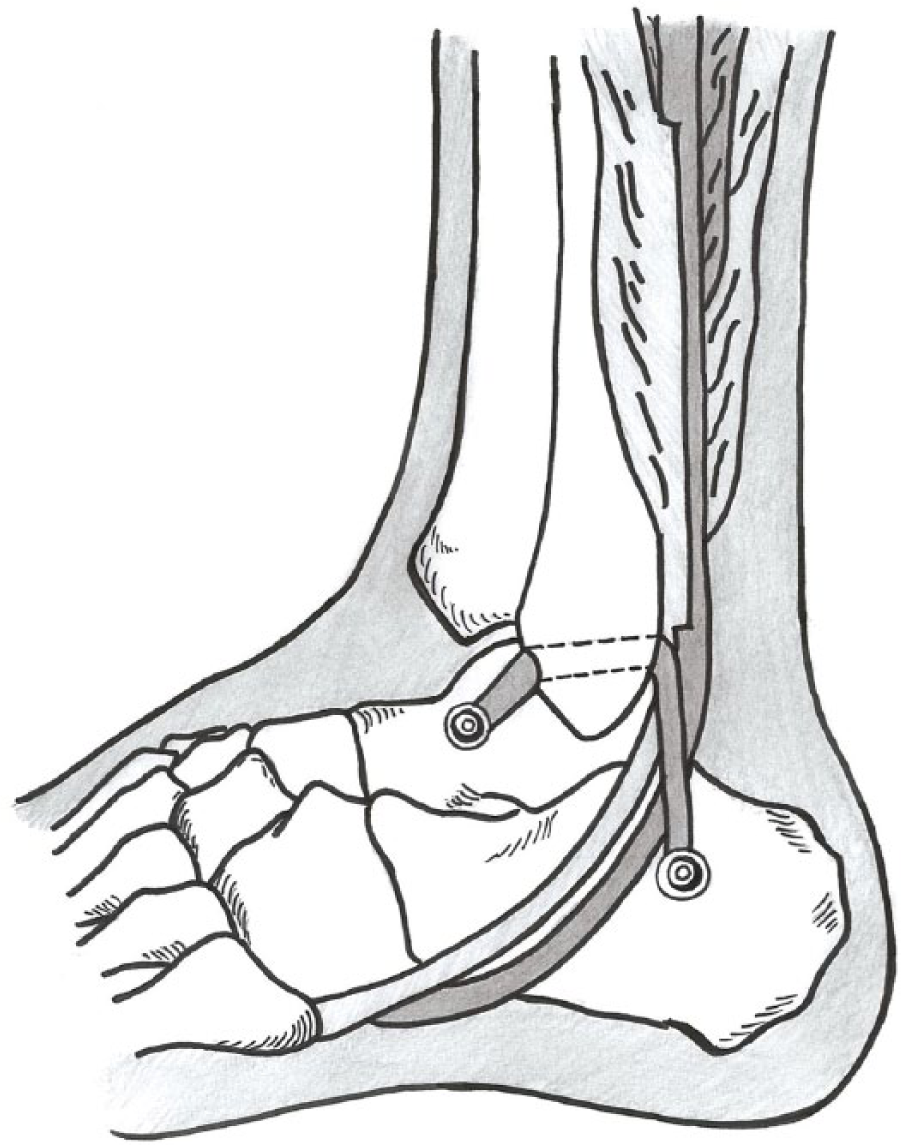
Diagram showing percutaneous lateral ankle ligament reconstruction using a split half of the peroneus longus tendon.
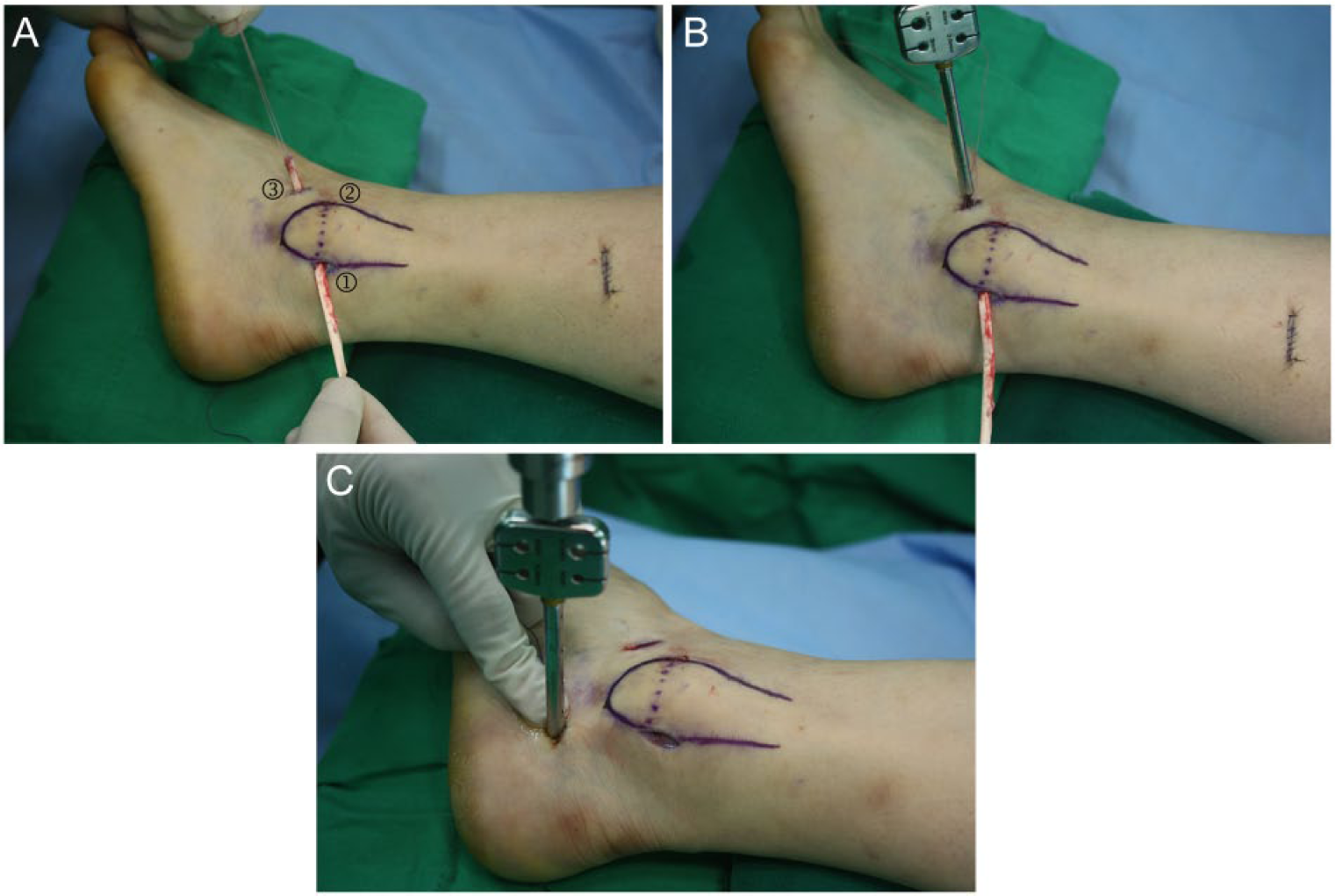
(A) A fibular bone tunnel is made in a posterior to anterior direction through the (1) incision made for the tendon harvest. A percutaneous (2) incision is made just anterior to the fibular bone tunnel. A percutaneous (3) incision is made over the anterior margin of the talar body where the anterior talofibular ligament attaches. A talar bone tunnel is made through the (3) incision. The harvested tendon is then passed through the fibular bone tunnel in a posterior to anterior direction and is pulled out through the (2) incision and then through the (3) incision using an eyelet needle or loop wire. (B) The tendon is fixed into the talar tunnel using a bioabsorbable interference screw. (C) The posterior end of the tendon is then passed downward over the peroneal tendons and fixed into the calcaneal wall using a bioabsorbable interference screw.
Postoperatively, the ankle is immobilized in a short leg cast in a neutral position. Active range of motion and protected weight-bearing is allowed 4 weeks after the operation. A soft ankle orthosis is used for another 4 weeks and balance training and proprioceptive exercises are encouraged.
Discussion
In the literature, the peroneus longus tendon has been successfully used for lateral ankle ligament reconstruction for the treatment of chronic lateral ankle instability.2,6,10 There are several advantages to using a split half of the peroneus longus tendon for percutaneous lateral ankle ligament reconstruction. Since the peroneus longus tendon is superficial in the distal leg and has no juncturae or adherence to the surrounding soft tissue, it is easily harvested using a tendon stripper. 13 Moreover, it can be harvested with the patient in the same position as that used for lateral ankle ligament reconstruction and does not require repositioning. Furthermore, the tendon harvest can be achieved through 1 of the percutaneous incisions created for the reconstruction.
A split half of the peroneus longus tendon has been reported to be an acceptable autogenous graft source with respect to its safety, strength, and donor site morbidity. 13
However, the peroneus longus is a dynamic lateral ankle stabilizer, therefore, disturbing it can have drawbacks. However, we believe that using the peroneus longus tendon for percutaneous lateral ankle ligament reconstruction is a better option than using the peroneus brevis tendon for percutaneous Chrisman-Snook lateral ankle ligament reconstruction since the peroneus brevis is the primary dynamic stabilizer and a more effective evertor than the peroneus longus. 8 The peroneus longus tendon may not be adequate to use when there are splits or tears in the tendon. Careful physical examination should be performed and MRI should be considered before surgery when these pathologies are suspected.
Another disadvantage of this technique is that the percutaneous technique does not restore the CFL anatomically, since the reconstructed autograft tendon passes over the peroneal tendons from the posterior aspect of the distal fibula but not from the distal tip where the CFL originally attaches. However, anatomic reconstruction using a graft tendon is difficult in cases after failed prior surgeries where anchors were used in the original surgery inside the fibula where the ligaments attach. Creating fibular bone tunnels at the ligament attachment sites for anatomic reconstruction is difficult unless the anchors are removed. However, it is difficult to remove the anchors, and although doing may be possible, the possibility of bone breakage exists when fibular bone tunnels are created at sites where anchors have been removed. In this case, a fibular bone tunnel can be made in a posterior-to-anterior direction proximal from the distal tip of the fibula toward the ATFL attachment area without disturbing the anchor (Figure 4). This fibular bone tunnel can be used for the percutaneous lateral ankle ligament reconstruction using a split half of the peroneus longus tendon. We performed this technique in 5 patients with failed Broström procedure using the anchors. None of the cases had bone breakage nor recurrent ankle instability at a median of 13 months follow-up.

Lateral view of an ankle after a failed Broström procedure showing 2 anchors in the fibular. A fibular bone tunnel (dotted line) made without disturbing the anchors can be used in percutaneous lateral ankle ligament reconstruction.
Although there is no evidence that the percutaneous lateral ankle ligament reconstruction technique results in better outcome over an open procedure, when lateral ankle ligament reconstruction requires combination with other procedures that carry more extensive approach, such as total ankle replacement, use of the percutaneous approach can eliminate the need to make a large incision close to those incisions used in other procedures.
In conclusion, percutaneous lateral ankle ligament reconstruction using a split half of the peroneus longus tendon as a free autograft can be an operative option for chronic ankle instability with attenuated or deficient ligaments, especially for cases after a failed Broström procedure with the anchors inside the fibula. The split half of the peroneus longus tendon can be easily harvested using a tendon stripper through the incision created for percutaneous lateral ligament reconstruction without the need for patient repositioning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.