
Abstract
Background:
Adult acquired flatfoot deformity is characterized by midfoot abduction and collapse of the medial longitudinal arch. Lateral column lengthening osteotomies primarily correct the abduction deformity, but the effects of graft shape on deformity correction and forefoot loading are unclear. Therefore, the purpose of this study was to demonstrate the effect of graft shape and taper on deformity correction and forefoot loading mechanics in a cadaveric flatfoot model.
Methods:
Flatfoot deformity was simulated in 18 cadaveric specimens. A lateral column lengthening osteotomy was performed using a triangular, trapezoidal, and rectangular graft for each specimen. During each testing condition, talonavicular joint angles and forefoot plantar pressures were measured.
Results:
Each graft shape corrected abduction and dorsiflexion deformity at the talonavicular joint. Coronal plane correction was affected by graft shape, and the less tapered trapezoidal and rectangular grafts overloaded the lateral forefoot compared to the intact condition. The more tapered triangular graft did not cause a lateral shift in forefoot pressures. Forefoot plantar pressures were strongly correlated with talonavicular abduction correction (R2 = .473, P < .001).
Conclusion:
Graft shape had no effect on the correction of talonavicular abduction or dorsiflexion but did influence coronal plane motion and forefoot loading mechanics. Also, overcorrecting the abduction deformity was predictive of increased lateral plantar pressures.
Clinical Relevance:
Although overcorrection of the abduction deformity at the midfoot remains the primary determinant of lateral forefoot overload, utilizing a graft with a larger taper may lower the incidence of lateralized forefoot pressure following correction.
Lateral column lengthening (LCL) osteotomies have proved effective in the treatment of adult acquired flatfoot deformity. Elongation of the calcaneus adducts the forefoot while also restoring the medial longitudinal arch.15,21 Although the LCL procedure corrects flatfoot deformity, plantar pain secondary to the procedure has been reported in as many as half of patients. 10 Lateral forefoot pain after LCL has been linked to elevated plantar loading of the lateral forefoot but does not appear to be associated with overcorrection. 12
Cadaveric studies have also demonstrated that isolated LCL osteotomies tend to overload the lateral portion of the forefoot.4,18,21,25 The size of the graft has a graded effect on both the amount of deformity correction and forefoot loading, 21 but the influence of graft shape on these mechanics is less clear. The LCL procedure was first described by Evans 14 as an opening wedge osteotomy to increase the length of the lateral column of the foot. Mosca 20 modified this technique by using a trapezoidal graft to alter the center of rotation of the osteotomy to approximate the center of the head of the talus. While each of these grafts adducts the forefoot, the graft shape and taper determines the amount of anterior calcaneal rotation and distraction. The effect of graft shape on the amount of deformity correction and forefoot load transfer remains unclear.
Therefore, we performed this study to determine whether graft shape and taper are an important factor when planning a LCL osteotomy for the treatment of adult acquired flatfoot deformity. Specifically, this study was performed to answer 3 research questions: (1) Does graft shape have an effect on correction of the talonavicular deformity when the width of the graft is held constant? (2) Can graft shape mitigate overload on the lateral portion of the forefoot during simulated standing? and (3) Is the amount of deformity correction predictive of lateralization of forefoot pressures? We hypothesized that grafts with a smaller taper, such as a rectangular graft, would result in greater talonavicular correction but also increase lateral loading of the forefoot compared to grafts with a larger taper such as a triangular or trapezoidal graft. In addition, we hypothesized that the amount of abduction correction would be positively correlated with a lateral shift in forefoot loading.
Materials and Methods
Eighteen fresh-frozen midtibia cadaveric lower limbs (13 male) of a mean age of 59 years (36 to 71 years) were used in this study. Specimens had no history of lower extremity injuries, and visual inspection revealed no musculoskeletal deformities. Soft tissues proximal to the ankle joint were removed and the proximal tibia was secured in epoxy bonding cement (Bondo/3M, Atlanta, GA). The distal fibula was held fixed to the tibia with the syndesmosis reduced using a single wood screw and a thin canvas strap was sutured to the Achilles tendon. Skin, tendons, and fat were removed around the joints of the midfoot and hindfoot to allow for clean access to these joints for flatfoot creation and the LCL osteotomy.
Standing was simulated during 5 test conditions for each specimen: intact, flatfoot, triangular LCL graft, trapezoidal LCL graft, and rectangular LCL graft. Specimens were loaded using a hydraulic loading frame (Bionix 858, MTS Systems, Eden Prairie, MN) and a pneumatic cylinder (Minimatic, Clippard, Cincinnati, OH) attached to the Achilles tendon strap (Figure 1). Standing was simulated by applying a 750 N compressive load on the tibia and a 350 N Achilles load. These values approximated the ground reaction force of 400 N that is equivalent to one-half body weight. The Achilles tension transferred load through the midfoot that resulted in plantar loading on the forefoot and represented the estimated tendon load during standing. 7 A thin plastic sheet was placed between the foot and testing setup to reduce friction at the plantar surface and to allow for unconstrained motion of the foot. 17 Each loading trial lasted 5 seconds, and motion capture data confirmed that equilibrium of the bones was satisfied. One loading trial was performed for each test condition.
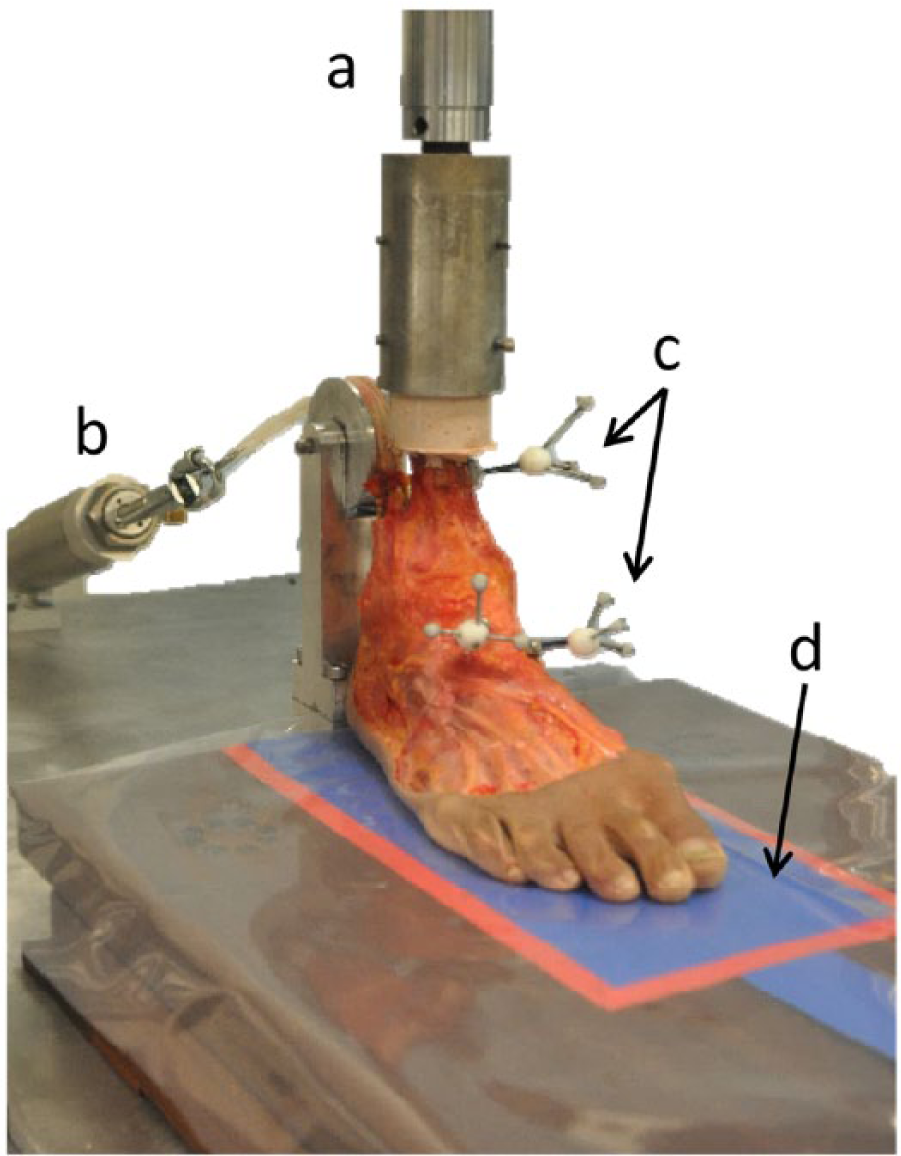
Experimental setup utilized a hydraulic testing frame (a) to load the tibia while a pneumatic cylinder (b) applied constant tension to the Achilles tendon. Reflective markers (c) were rigidly attached to the tibia, talus, and navicular for the purpose of calculating talonavicular joint angles throughout the experiment. A pressure sensitive mat (d) was placed to the ground surface to measure plantar pressures during each trial.
Flatfoot deformity was created by sectioning the spring ligament, the medial capsule of the talonavicular joint, and the interosseous talocalcaneal ligament. These ligaments have been identified as commonly damaged tissues in patients with adult acquired flatfoot deformity 9 and have been sectioned in a previous cadaveric model to create a deformity. 21 Then, the foot was axially loaded to 1150 N for 400 cycles while the Achilles tendon was under 350 N of tension, which resulted in an 800 N ground reaction force. To confirm that a deformity of sufficient magnitude was created, a custom written MATLAB routine (The Mathworks, Natick, MA) calculated talonavicular abduction. Because we wanted a mild to moderate abduction deformity, cyclic loading was applied until talonavicular abduction was between 5 and 15 degrees compared to the intact condition. If this deformity magnitude did not result after 400 cycles, up to 400 additional loading cycles were performed until the desired deformity was achieved.
To determine the effect of graft taper on talonavicular deformity correction and forefoot loading, each specimen was tested using 3 graft shapes: a triangle, trapezoid, and rectangle (Figure 2). These grafts had a base width of 10 mm, were 8 mm in height, and 23 mm in length; the base width of 10 mm has been used in previous cadaveric investigations of LCL osteotomies,1,4,21,25 and the height and length of the grafts were determined from measurements of the osteotomy site collected during pilot testing. These custom made grafts were built from aluminum and the same set was used for each specimen. The triangular graft provided 10 mm of lateral side distraction and no medial side distraction, the trapezoidal graft provided 10 mm of lateral side distraction and approximately 5 mm of medial side distraction, and the rectangular graft distracted by the lateral and medial sides of the calcaneus 10 mm. These geometries demonstrate that the triangular graft had the largest taper angle while the rectangular graft had the smallest taper angle. These 3 graft shapes were tested to better understand the effects of graft taper on forefoot correction and load transfer, not necessarily which specific graft geometry was best for correcting flatfoot deformity. LCL osteotomies were performed by creating a “Z” cut through the body of the calcaneus (Figure 3A) as described by Vander Griend. 26 This osteotomy has been shown to be biomechanically similar to an Evans LCL osteotomy 22 but may have provided a more stable platform for fixation in our cadaveric model and greater potential for osseous healing in vivo. Each graft was placed in the superior space of the osteotomy site with the base of the implant flush with the lateral border of the anterior calcaneal segment (Figure 3B). To achieve stability of the osteotomies, we used external fixators (Hoffmann II Micro External Fixation System, Stryker Corporation, Kalamazoo, MI) on both the medial and lateral aspects of the calcaneus (Figure 3B). Self-drilling 2.0 mm pins were placed through both cortices close to the osteotomy site, and 5.0 mm stainless steel rods were used to achieve rigid fixation of the osteotomy. During testing we did not observe any motion of the grafts; and during pilot testing, motion between the segments of the calcaneus was detected to be less than 1.0 mm. The external fixator pins also provided leverage to ensure that the sides of the grafts were fully in contact with the calcaneal segments.
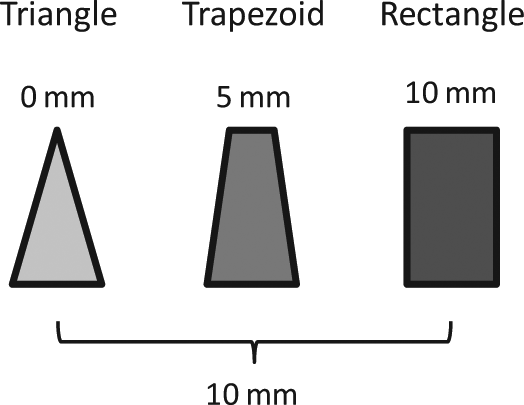
Schematic of the 3 graft geometries tested. All grafts had a constant base width (bottom) of 10 mm. Each taper angle was a function of the width of the opposing base (top), where the triangular graft had the largest taper angle because its opposing base width was 0 mm and the rectangular graft had the smallest taper angle because its opposing base width was 10 mm. The opposing base width affected the amount of distraction of the medial cortex of the calcaneus.
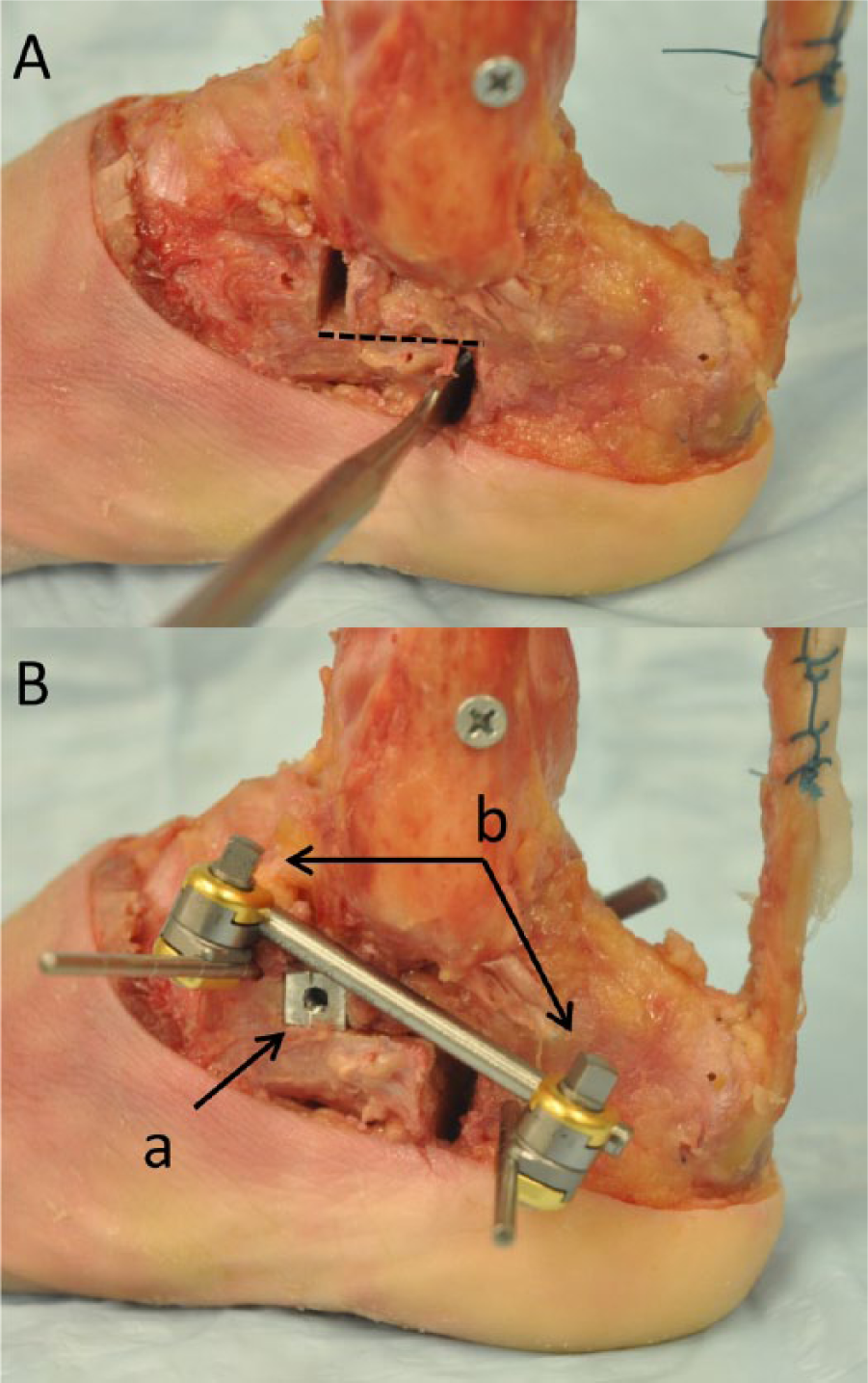
(A) Photograph of the Z-cut osteotomy (dashed line identifies horizontal cut) near the anterior body of the calcaneus. (B) A triangular graft (a) was inserted into the superior space created from distracting the 2 calcaneal segments. An external fixator (b) was placed on the lateral side to prevent motion between the 2 calcaneal segments, and a second external fixator was placed on the medial side of the calcaneus.
To quantify talonavicular motion, reflective markers that were rigidly attached to the talus and navicular bones (Figure 1) were tracked using a 4 camera motion capture system (Eagle-4, Motion Analysis Corp, Santa Rosa, CA). Joint angles were considered zero when the intact foot was loaded and were based on recommendations made by the International Society of Biomechanics. 27 Briefly, talonavicular adduction occurred in the axial plane defined by the long axis of the tibia and transmalleolar axis, dorsiflexion occurred in the sagittal plane that was perpendicular to the transmalleolar axis, and inversion occurred in the plane that was perpendicular to the previous planes of motion. Although inversion was expressed about an axis that changed as a function of dorsiflexion and internal rotation, this motion occurred in a plane similar to the coronal plane when the other rotations of the foot were small. Unlike clinical imaging of the talonavicular joint that commonly describes the amount of uncoverage of the joint,13,28 our measurements only describe the angular relation between talus and navicular. Talonavicular adduction, dorsiflexion, and inversion were calculated as positive values for all feet.
Plantar pressure measurements were acquired using a pressure sensitive mat (Pliance 32, Novel, Munich, Germany). During testing, the toes pointed anteriorly and the medial aspect of the foot was parallel with the length of the mat. Because the automated masking software provided by the vendor required complete plantar pressure information to generate the mask (which was not available from our simulated standing data), a single investigator identified the forefoot region that has previously been described in the literature.12,21 A custom written MATLAB routine calculated the weighted center of plantar pressure in the mediolateral direction (Figure 4); a plantar pressure map for each condition was displayed on a computer monitor and the same investigator placed a bounding box around the forefoot region. The weighted center of plantar pressure (Equation 1) was calculated for each loading condition. Next, center of plantar pressure data were normalized to the intact condition for each specimen, where a positive value indicated a lateral shift in forefoot pressures. In several specimens, the LCL conditions resulted in undetectable amounts of medial forefoot pressures. To account for this, forefoot width for each test condition was set to be equivalent to the intact condition (this was accomplished by adding columns of zeroes to act as place holders in the data arrays). Forefoot width was calculated as the width of the bounding box for the intact condition. Repeated measurements were performed on a specimen and the coefficient of variation of the center of plantar pressure calculation was 1%.

where pi denotes the summed plantar pressures for the ith column of data from the medial boundary of the forefoot, and xi denotes the location of the plantar pressure data in the forefoot region.
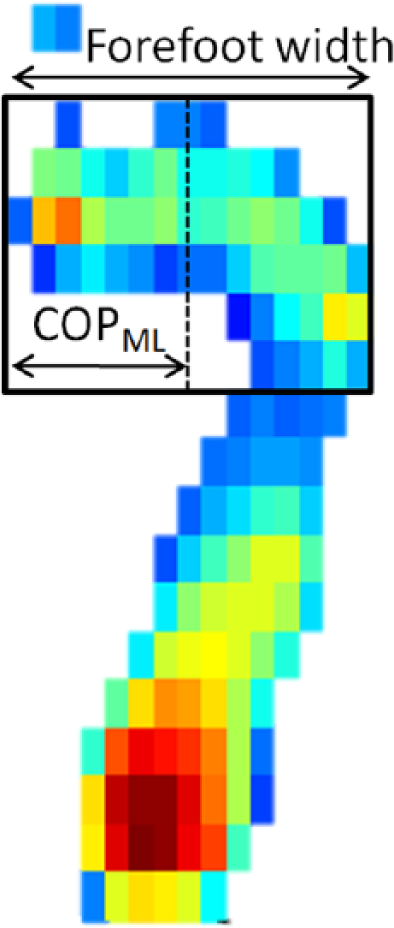
Plantar pressure map of intact specimen with forefoot bounding box (rectangle) and calculated center of mediolateral pressure (COPML) represented by a dashed line. The width of the forefoot was defined as the width of the bounding box, and toes were not included in the calculation. The forefoot included the region that is normally occupied by the base of the fifth metatarsal, which was often pronounced in the LCL conditions.
To test that our flatfoot model provided significant talonavicular deformity, 1-sample t tests were performed to compare the joint angles of the flatfoot condition to the intact condition (joint angles for intact condition are considered zero degrees). To test our first hypothesis that graft taper would have an effect on the amount of deformity correction, 1-way repeated-measures analyses of variance were performed for talonavicular abduction, dorsiflexion, and inversion. Due to the close proximity of the motion capture markers to the bones, markers were inadvertently moved on 6 specimens and further analysis of the motion capture data confirmed that these data were affected. We analyzed 12 specimens that had unaffected motion capture data. To test our second hypothesis that graft shape would affect forefoot loading, a 1-way repeated-measures analysis of variance model was used to compare the mediolateral shift in the center of plantar pressure between the intact, flatfoot and 3 LCL conditions. Plantar pressure data for 1 specimen were not complete (motion data from this specimen was complete); therefore data from 17 specimens were analyzed. To test our third hypothesis that the amount of correction of the talonavicular deformity would be predictive of lateralization of forefoot loading, we performed simple linear regressions using the amount of correction as the explanatory variables and the change in forefoot loading as the response variable. All analyses were performed in SigmaPlot software (Version 12.3, Systat Software Inc, Chicago, IL), and analysis of variance models used a Tukey post hoc test to control for multiple comparisons. Statistical significance was set at α = .05.
Results
The flatfoot model was confirmed with both talonavicular deformity and a medial shift in forefoot plantar pressures (Figures 4 and 5). Talonavicular abduction and dorsiflexion were both significantly increased compared to the intact condition (P < .001), but the amount of eversion at the talonavicular joint created in the flatfoot condition was small and not significantly different than the intact condition (P = .074). Forefoot pressures shifted medially an average of 9% of the forefoot width following the creation of the flatfoot deformity (P < .001).
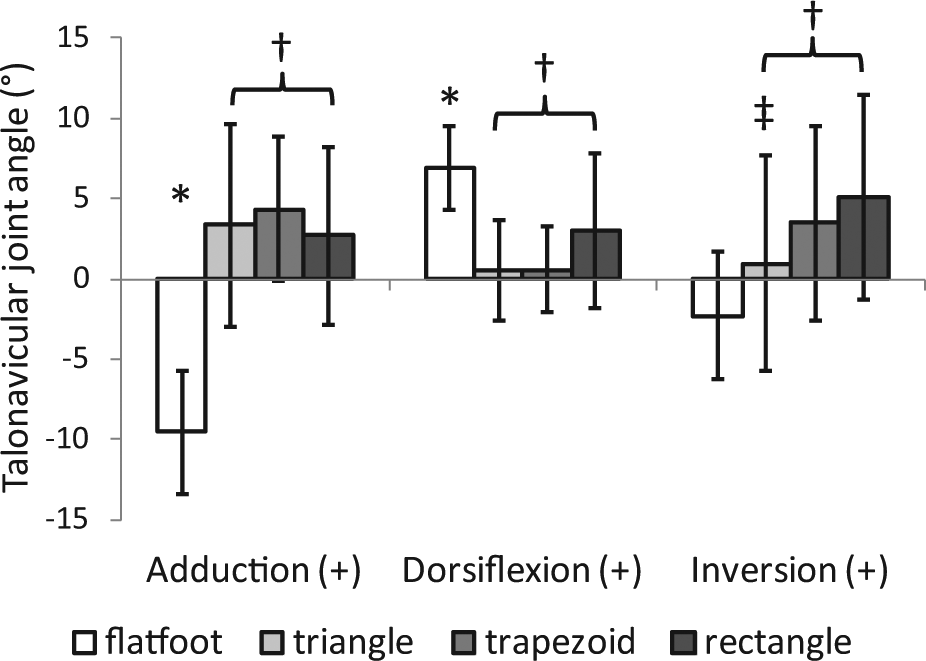
Talonavicular joint angles shown for the flatfoot and 3 LCL graft shapes and were offsets from the intact loading condition. The flatfoot deformity resulted in increased amounts of abduction and dorsiflexion compared to the intact condition (*P < .001). Following each of the LCL conditions, talonavicular abduction and dorsiflexion deformities were reduced compared to the flatfoot condition (†P ≤ .012). Each graft shape also inverted the talonavicular joint compared to the flatfoot condition (†P ≤ .012) while the triangular graft resulted in less inversion compared to the rectangular graft (‡P = .014).
The 3 LCL grafts provided significant correction of the talonavicular abduction and dorsiflexion deformity compared to the flatfoot condition (P ≤ .012, Figure 5); however, the amount of correction in the coronal plane differed with graft taper angle. While all 3 graft shapes inverted the talonavicular joint compared to the flatfoot condition (P ≤ .012), the rectangular graft resulted in greater talonavicular inversion than the triangular graft (P = .014, Figure 5).
Forefoot loading shifted laterally following each of the 3 grafts compared to the flatfoot conditions (P < .001; Figure 6); however, the triangular graft did not result in elevated lateral loading compared to the intact condition while the other 2 grafts did (P ≤ .002). In the intact condition, the center of forefoot pressure was located 54% of the forefoot width from the medial border of the first ray. The trapezoidal and rectangular grafts both caused an average lateral shift of 7%.
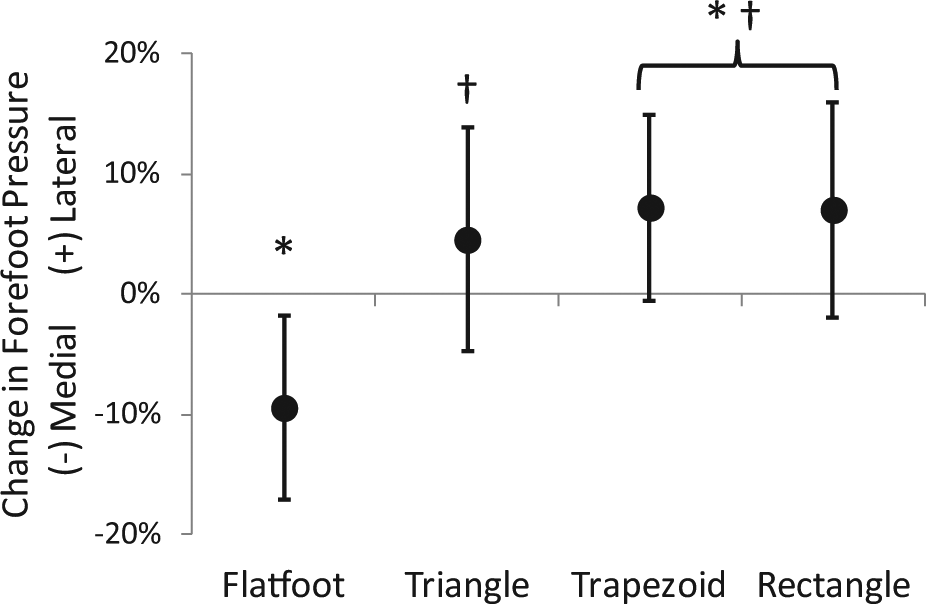
Mediolateral shift in forefoot center of contact pressure compared to the intact condition reported as a percentage change normalized by the width of the foot. The flatfoot condition demonstrated a medial shift compared to the intact condition, while all 3 LCL graft conditions showed a lateral shift of forefoot contact pressure compared to the flatfoot condition. The triangular graft did not overload the lateral forefoot compared to the intact condition. *P ≤ .002 compared to intact condition; †P < .001 compared to flatfoot condition.
Lateralization of the forefoot pressures was positively and moderately correlated with the correction of the talonavicular abduction deformity (Figure 7). While the 3 LCL grafts consistently corrected the abduction deformity, 47% of the variation in forefoot pressures was explained by the abduction correction (P < .001). No correlations were found between the lateral shift in forefoot pressures and the amount of correction of the talonavicular dorsiflexion and eversion (R2 ≤ .052, P ≥ .233).
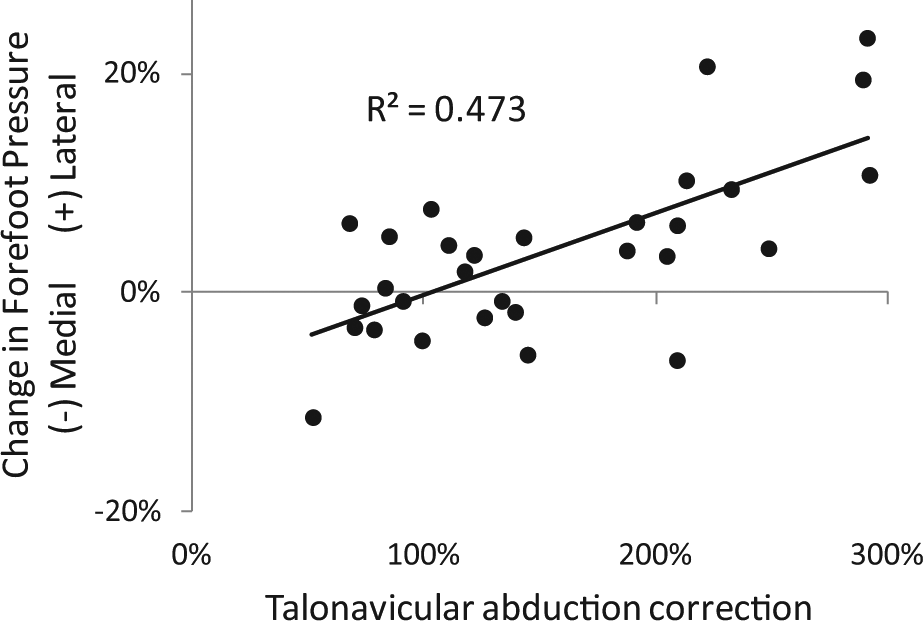
Lateralization of forefoot center of pressures following LCL osteotomies compared to the amount of talonavicular deformity correction, where 100% of abduction correction represents restored intact talonavicular alignment compared to the intact condition and greater than 100% demonstrates over correction. A significant correlation was found between forefoot pressure lateralization and talonavicular abduction correction (R2 = .473, P < .001).
Discussion
The results from this study supported our hypotheses that LCL graft shape and amount of taper influences the amount of deformity correction (Figure 5) and forefoot loading mechanics (Figure 6). Each graft, regardless of taper angle, provided significant correction of talonavicular abduction and dorsiflexion deformity. However, the triangular graft inverted the talonavicular joint less than the rectangular graft and did not overload of the lateral forefoot like the trapezoidal and rectangular grafts. We also found that nearly one-half of lateralization of forefoot pressures was explained by the amount of talonavicular abduction correction (Figure 7). To our knowledge, this is the first report on the effects of LCL shape and taper on deformity correction and forefoot load transfer.
There are several reported methods for creating flatfoot deformity in cadaveric specimens that compare favorably to our model. Previous models report a range of 4-14 degrees of talonavicular abduction deformity and 3-11 degrees talonavicular dorsiflexion,4,17,21,29 which are similar to our deformity amounts of 10 and 7 degrees, respectively. However, our model resulted in an average of 3 degrees of talonavicular eversion, which was less than half the reported value of eversion in flatfoot models that created similar amounts of talonavicular abduction and dorsiflexion.17,29 In addition, our observations of a medial shift in forefoot pressure following the creation of the flatfoot deformity is similar to previous reports in cadaveric studies.4,16,21
Correction of the talonavicular deformity in this study was comparable to previous reports. In a prior study that used a similar loading model, an Evans osteotomy with a 10 mm trapezoidal graft resulted in 14 degrees of adduction and 6 degrees of plantarflexion that was the same amount of correction found in the current study when the trapezoidal graft was used. 21 Other cadaver experiments with slightly different loading schemes and LCL techniques demonstrated similar amounts of correction of talonavicular deformity. A calcaneocuboid distraction LCL resulted in an average of 11 and 8 degrees of abduction and dorsiflexion correction, respectively; 18 while an Evans LCL with a 10 mm graft in conjunction with an FDL tendon transfer produced 20 degrees of adduction and 10 degrees of plantarflexion compared to the flatfoot deformity. 4 The use of a 10 mm trapezoidal graft in our study inverted the talonavicular joint an average of 6 degrees while a recent study performed by Zanolli and colleagues 29 found that an 8 mm trapezoidal graft resulted in 7 degrees of correction in the coronal plane.
The characteristic lateral shift of forefoot pressures following LCL has been well documented in both cadaveric and clinical studies. Cadaveric models that investigated the effects of several different LCL techniques demonstrated consistent lateralization of the forefoot loads compared to both the intact and flatfoot conditions.4,16,18,21,25 Patients that report lateral foot pain after flatfoot reconstruction also demonstrate elevated pressures under the lateral forefoot. 12 Surprisingly, these patients do not appear to have differences in talonavicular alignment compared to asymptomatic flatfoot patients, although it should be noted that talonavicular inversion is typically not measured in clinical populations and may be an important parameter to consider in future studies, as it may relate to residual forefoot supination following flatfoot correction. We found a strong and positive correlation between forefoot loading and the amount of talonavicular abduction correction. However, this relationship between talonavicular alignment and forefoot loading may weaken in the presence of concomitant corrective procedures commonly performed on flatfoot patients. 12
Our findings suggest that graft shape and taper has an effect on forefoot loading mechanics (Figure 6) and talonavicular inversion but not on radiographic parameters like talonavicular abduction or dorsiflexion (Figure 5). Midfoot motion in the coronal plane is difficult to measure using planar imaging, but several cadaveric studies report talonavicular eversion as a component of flatfoot deformity.17,29 The amount of graft taper appeared to have a graded effect on talonavicular inversion (Figure 5), suggesting that a graft with a smaller taper may result in greater midfoot inversion that may manifest as residual forefoot supination following flatfoot correction. In addition, excessive inversion of the midfoot and forefoot might lead to stiffness and reduced mobility of the midfoot joints, which are essential for walking and running in healthy populations.2,19 Although our findings were significant, additional variability is likely to occur in vivo, and the effects of graft taper on midfoot inversion may be less pronounced in a clinical population.
In addition to the increased talonavicular inversion caused by the rectangular graft, the graft was sometimes difficult to fully insert into the osteotomy. Smaller specimens tended to demonstrate some amount of talonavicular distraction when the rectangular graft was used. This was likely a result of excessive distraction of the calcaneocuboid joint and a likely artifact resulting from the graft being too large for these small feet, since this type of talonavicular distraction did not occur in larger feet. Although we did not measure midfoot joint pressure, a previous investigation found a strong link between graft size and calcaneocuboid contact pressure. 8 While each of the grafts tested were 10 mm wide, the rectangular graft resulted in a markedly stiffer hindfoot than the other grafts, which may have increased contact pressure in neighboring joints. We observed this foot stiffness as resistance to manual pronation-supination of the midfoot; and although foot stiffness is a difficult measure to quantify, it has been reported as a symptom in LCL patients and may be predictor of patient reported pain secondary to surgery. 10
Approximately 50% of lateral foot overload variability was explained by talonavicular correction (Figure 7), suggesting that other properties of the foot are equally responsible for the manifestation of elevated plantar pressure and pain.6,10 These results also suggest that lateral overload does not occur when perfect correction is achieved and overcorrection is avoided. However, assessing deformity correction in the operating room is difficult, and it may be prudent to mitigate the risk of lateral overload of the forefoot by judiciously lengthening the lateral column without creating stiffness and limiting eversion motion. 11
This study was affected by several limitations. The flatfoot deformity was created by sectioning several ligaments commonly deficient in patients with flatfoot deformity 9 and loading the foot cyclically several hundred times. Although other flatfoot models utilize a greater number of loading cycles and ligament attenuation, 5 our flatfoot deformity model was confirmed with both talonavicular joint angles and forefoot plantar pressures. We also simulated standing by applying an axial load along the tibia and a tensile load on the Achilles tendon, instead of using other simulation techniques that involve additional muscles and dynamic simulation;3,23,24 our results should be interpreted as measurements similar to those made using standing fluoroscopy. We decided to not include tibialis posterior tendon actuation during the intact condition; while this may have manifest in an intact foot that was slightly planus, 16 the goal of this study was to understand the effects of LCL graft shape and taper on foot mechanics and including posterior tibialis tension during the intact condition would have been a confounding variable. In addition, we did not attempt to provide perfect correction for each specimen, but rather we compared 3 graft shapes of constant width to understand the mechanics of graft taper angle. Although increased loading of the fifth metatarsal may be responsible for plantar pain, 12 we did not track the position of the fifth metatarsal with respect to the plantar pressure mat and decided to use mediolateral forefoot loading as a surrogate for lateral overload of the forefoot. Although the ISB definition of the lower extremity describes foot inversion as motion about a common axis, we described this motion as coronal plane motion, which may become less appropriate as joint motion in other planes becomes large.
In conclusion, our results suggest that graft shapes used in LCL osteotomies do not affect correction of the talonavicular abduction or dorsiflexion deformities, but grafts with a larger taper, such as a triangular graft, result in less talonavicular inversion and do not overload the lateral forefoot compared to grafts with no taper, such as a rectangular graft. Although the effect sizes of graft taper on midfoot kinematics and forefoot loading mechanics were small, our results suggest that graft taper may be worth considering when planning surgery. In addition, the amount of abduction deformity correction appeared to be a strong predictor of lateral forefoot pressures, which likely manifests as pain. These results are representative of deformity correction in a simulated standing task. Further study is needed to understand the effect of graft shape and taper on more functional tasks like walking that are likely more reliant on preserving the mobility of the foot.
Footnotes
Authors’ Note
The use of cadaveric specimens for this study was approved by our institute’s ethical review board. The investigation was performed at the Hospital for Special Surgery.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Herbert Black Fund for Foot and Ankle Research and the Joseph M. Lane Research Grant.