
Abstract
Background:
Lateral column lengthening (LCL) has been used for correction of flatfoot deformity. The purpose of this study was to determine the effect of LCL graft shape on tarsal bone position and talonavicular and subtalar joint pressure.
Methods:
A flatfoot model was created in 6 cadaveric specimens. Corrective LCL was performed using a rectangular graft or a trapezoidal graft with the broad surface oriented dorsally, laterally, or plantarly. Bony surface markers were digitized to calculate angular parameters used in the evaluation of flatfoot deformity. Contact pressure and area in the subtalar and talonavicular joints were also recorded. All measurements were carried out under multiple axial loads in the intact and flatfoot conditions, and following LCL with each graft shape.
Results:
Flatfoot creation resulted in significant changes in arch collapse and forefoot abduction. LCL with a rectangular graft best corrected these parameters, while a laterally oriented trapezoidal graft provided some correction. Talonavicular contact pressure was unchanged after flatfoot creation, and was significantly less than intact after LCL. Subtalar contact pressure decreased in some conditions after flatfoot creation, and decreased further after LCL.
Conclusion:
LCL with a rectangular graft best restored tarsal bone orientation in a cadaveric flatfoot model. The decreases in talonavicular pressure likely represent redistribution of force from the medial to lateral foot.
Clinical Relevance:
When performing LCL for flatfoot deformity, increased bone graft volume medially better restores tarsal bone position. One way of achieving this is through the use of a rectangular graft as opposed to a trapezoidal graft.
Keywords
Acquired flatfoot deformity is caused most often by insufficiency of the tibialis posterior tendon.21,22,29 This leads to the characteristic findings of medial arch collapse, forefoot abduction, and hindfoot valgus.18,29 Radiographic evaluation is usually performed and allows for determination of the degree of arch collapse (lateral talo-first metatarsal angle 29 and calcaneal pitch),25,31 forefoot abduction (anterior-posterior [AP] talo-first metatarsal angle), 31 and hindfoot valgus (AP talo-calcaneal and lateral calo-calcaneal angles).2,7,25 There has been extensive literature to suggest that the initial treatment for acquired flatfoot should consist of conservative management;1,6,13,15,19 if operative intervention is required, a number of techniques have been reported based on the severity of the pathology.11,17,20,26,29
In cases of more mild, flexible flatfoot deformities, operative intervention is controversial. Lateral column lengthening (LCL) with a calcaneal osteotomy, as originally described by Evans, 10 has been demonstrated to restore medial arch height, forefoot abduction, and hindfoot valgus on imaging.4,9,12,27 There has been a variety of biomechanical work published on LCL. In 1 cadaveric study, DuMontier et al 8 used CT to quantify bony position shifts after LCL. The authors reported relative adduction and plantarflexion of the midfoot following the procedure, and noted linked motion of the navicular and cuboid. 8 Despite studies showing restoration of bony position with LCL, clinical outcomes have been mixed.4,9,12 Other work has focused on pressure redistribution about the foot. Tien et al 28 have demonstrated increased lateral plantar (foot-floor interface) pressures following LCL, which led these authors to suggest that a simultaneous procedure to redistribute forces medially be performed. 28 This concept was then studied by Benthien et al, 5 who performed sequential LCL and medial cuneiform osteotomy in a cadaveric flatfoot model. They reported improvement of the flatfoot deformity following LCL, as well as increased lateral forefoot plantar pressures which were relieved by medial cuneiform osteotomy. 5 Most recently, Xia et al 30 investigated the effect of LCL graft size on intra-articular calcaneocuboid pressure. The authors noted increased calcaneocuboid pressure with flatfoot creation, and demonstrated restoration of this pressure following LCL with smaller trapezoidal grafts. Larger trapezoidal grafts, however, resulted in calcaneocuboid pressures that were significantly greater than those recorded in normal feet. 30 One possibility is that abnormal redistribution of pressures following LCL may be causing mediocre clinical outcomes despite evident improvement in bony realignment following the procedure; a better understanding of these changes is an important factor to consider when attempting to improve outcomes.
Despite the extensive literature on LCL and some biomechanical work focusing on optimal graft size, there have been no biomechanical studies evaluating graft shape. This is important since there is no gold standard graft, and much of the current work has been performed using trapezoidal or “wedge” grafts.5,8,28,30 It is unknown if the conclusions drawn from the available literature regarding graft size would apply if a rectangular graft were used for the lengthening procedure. In addition, little data exist regarding subtalar or talonavicular joint pressures following such a procedure. The purpose of this study was to determine the effects of graft shape for LCL on foot and ankle biomechanics, including relative tarsal bone positions and contact pressure/area of the subtalar and talonavicular joints. We hypothesized that a rectangular graft would better restore bony realignment compared to a trapezoidal graft by increasing the volume of graft at the medial aspect of the osteotomy site, and that intra-articular pressures would not vary based on graft shape.
Materials And Methods
Specimen Preparation
Six fresh-frozen cadaveric below-knee specimens (5 males and 1 female; mean age at death, 83 years; standard deviation, 8 years) with no evidence of musculoskeletal pathology were used; institutional review board approval was not required since this was a basic science study. Specimens were dissected free of overlying skin and soft tissue while preserving the distal tibialis posterior (PT) tendon and its sheath as well as the plantar fascia and ligaments of the foot. Each tibia was placed in a section of PVC pipe, with care taken to ensure the tibial shaft was parallel to the long axis of the pipe. The tibia was then secured within the section of pipe using plaster of Paris reinforced with wood screws. The fibula was left attached distally and cut as high as possible to maintain length; it was not incorporated into the PVC pipe-plaster of Paris structure. Specimens were kept moist with 0.9% normal saline during all phases of testing.
Biomechanical Testing
After preparation, specimen-PVC pipe constructs were affixed to an MTS machine capable of applying a downward force through the section of PVC pipe, and a 5 Newton load was applied to the PT tendon using an in-line pulley (Figure 1). This loading scheme was chosen based on preliminary testing for its ability to maintain tension on the tendon and improve reproducibility while also minimizing the effect of PT load on flatfoot correction. Three constant, reproducible landmarks were identified and marked on the tibia, first metatarsal, navicular, talus, calcaneus, and cuboid; the origin and insertion of the long/short plantar and spring ligaments were also identified. The positions of these reproducible landmarks were measured using a Microscribe 3DLX system (Immersion Corp, San Jose, CA) by digitizing each set of points (Figure 2). This device is a mechanical-linkage system with a long arm attached to a stylus, which is placed on the point to be recorded. It is accurate to 0.30 mm and has a repeatability of 0.13 mm. 24 These positional data were recorded twice to ensure they were reproducible within 1 mm, and used to calculate positional parameters used in the evaluation of flatfoot deformity, including lateral talo-first metatarsal angle and calcaneal pitch (for evaluation of longitudinal arch collapse), AP talo-first metatarsal angle (for forefoot abduction), AP talo-calcaneal angle and lateral talo-calcaneal angle (for hindfoot valgus), and the length of the spring ligament. These angles were chosen since their radiographic counterparts are useful for characterizing the pes planus deformity in the clinical setting. It should be noted, however, that in this study these angles were calculated based on the relative positions of superficial bony landmarks in 3-dimensional space; similar methods have been shown to be accurate in previous literature.3,14
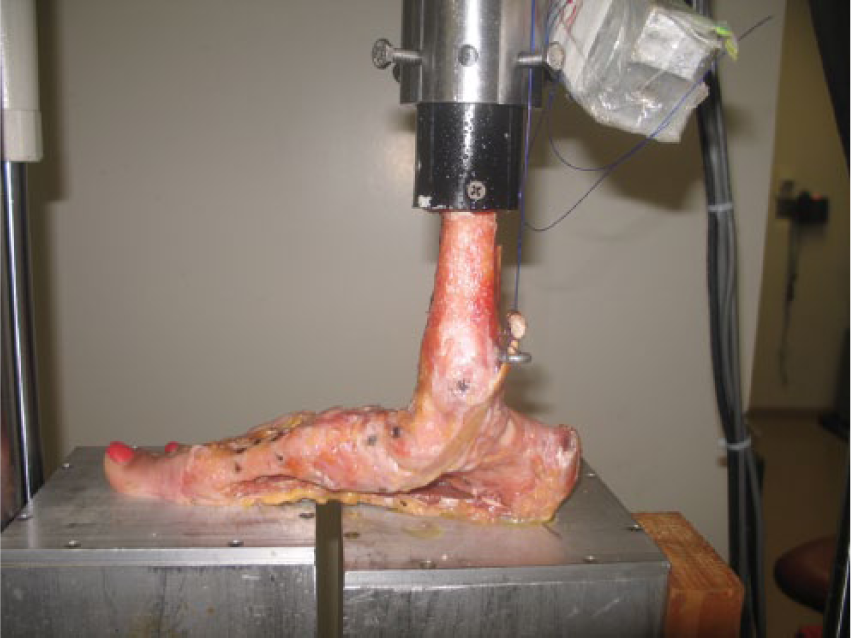
Photograph demonstrating specimen mounted to MTS machine, which applied a downward force through the tibia.

Photograph showing the Microscribe device (left-hand side) and Tekscan sensor (seen in the subtalar joint).
A Tekscan Model 4201 pressure sensor (Tekscan Inc, South Boston, MA) was calibrated using 2-point calibration at 200 and 1000 N, and then used to record contact area and pressure in both the subtalar and talonavicular joints (Figure 2). This device has 264 total sensor elements and a resolution of 27.6 sensels per square centimeter. Both positional and joint pressure testing described above was carried out for each combination of specimen condition (intact, flatfoot deformity, and after LCL with each graft shape) and axial load (200, 400, 600, 800, and 1000 N applied through the MTS system). Specimens were brought to a given load and data were recorded immediately; no creep was noted. Data were recorded at sequentially increasing loads, and the sequence was then repeated to ensure reproducibility within 0.5 MPa.
Flatfoot Model
A flatfoot model was created using a method described previously.8,16 This included spring ligament attenuation, which was achieved by (1) transection of approximately 50% of the superomedial spring ligament, (2) transection of the medial capsule of the talonavicular joint, and (3) transection of approximately 50% of the talocalcaneal ligament. Specimens were then loaded axially and cycled between 700 and 1200 N for 10,000 cycles at 0.5 Hz based on previous work showing adequate flatfoot creation using this methodology.8,16 Flatfoot was defined as a 10-degree change in the lateral talo-first metatarsal angle.
Lateral Column Lengthening
A vertical calcaneal osteotomy was performed 1 cm proximal to the calcaneocuboid joint with a thin oscillating saw as described by Raines et al (Figure 3). 23 Two different foam bone graft shapes were used to perform lengthening. The first was a rectangular graft (1 cm [AP] × 2 cm [dorsal-plantar] × 2 cm [medial-lateral]); the second was a wedge-shaped trapezoidal graft (0.5 cm × 1 cm × 2 cm × 2 cm). Each specimen underwent 4 different lengthening procedures with (1) the rectangular graft, followed by the trapezoidal wedge-shaped graft, which was tested with the 1 cm side of the wedge oriented (2) laterally, (3) dorsally, and (4) plantarly. A small plate and 3 screws were used for fixation of the graft during testing. No additional laxity or graft slippage was noted to develop from condition to condition.
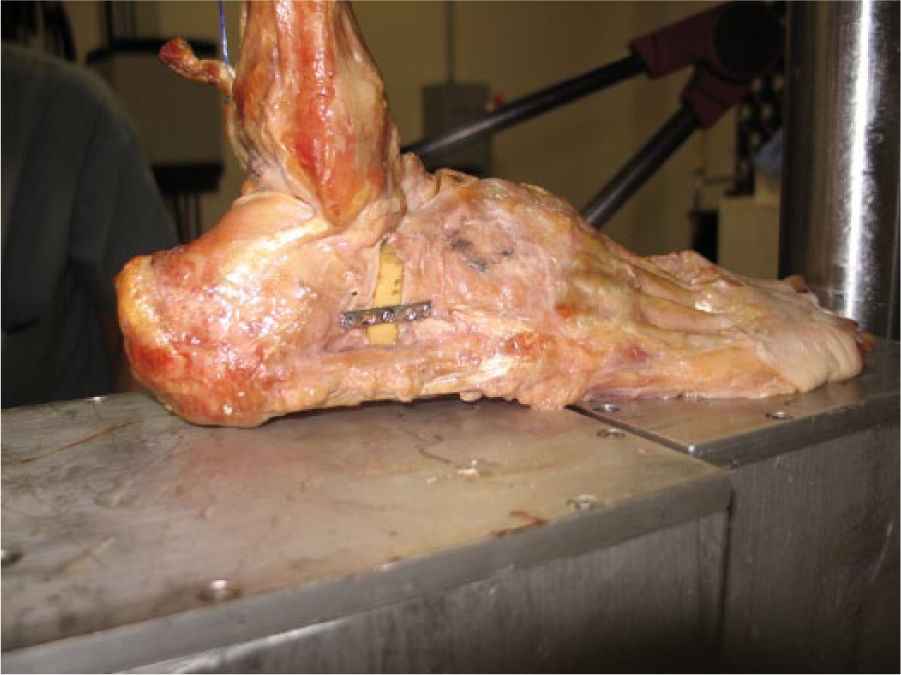
Photograph showing specimen after undergoing lateral column lengthening with a laterally oriented trapezoidal wedge graft.
Data Analysis
Based on pilot data, sample size calculation was performed using alpha of 5% and power of 80%. Four specimens were found to be required to show a difference between conditions for various positional parameters, while 6 were necessary to elucidate differences for some pressure/area measurements. A 2-way repeated measures analysis of variance was used to examine the effect of load and condition. Interaction effects were identified first. A post hoc Tukey test was performed to determine the simple effect of condition if interaction was present, or the main effect of condition if interaction did not occur.
Results
There was no interaction effect between load and condition for any of the parameters measured except for subtalar contact pressure, as described below.
Longitudinal Arch Collapse
Flatfoot creation resulted in plantar rotation of the long axis of the talus, such that the lateral talo-first metatarsal angle decreased significantly from intact. After LCL, this angle was no different from intact with the rectangular and lateral grafts. The specimens remained significantly different from intact with the plantar and dorsal grafts (Figure 4a). LCL resulted in a significantly improved angle when compared to the flatfoot model only when the rectangular graft was used (Figure 4a).
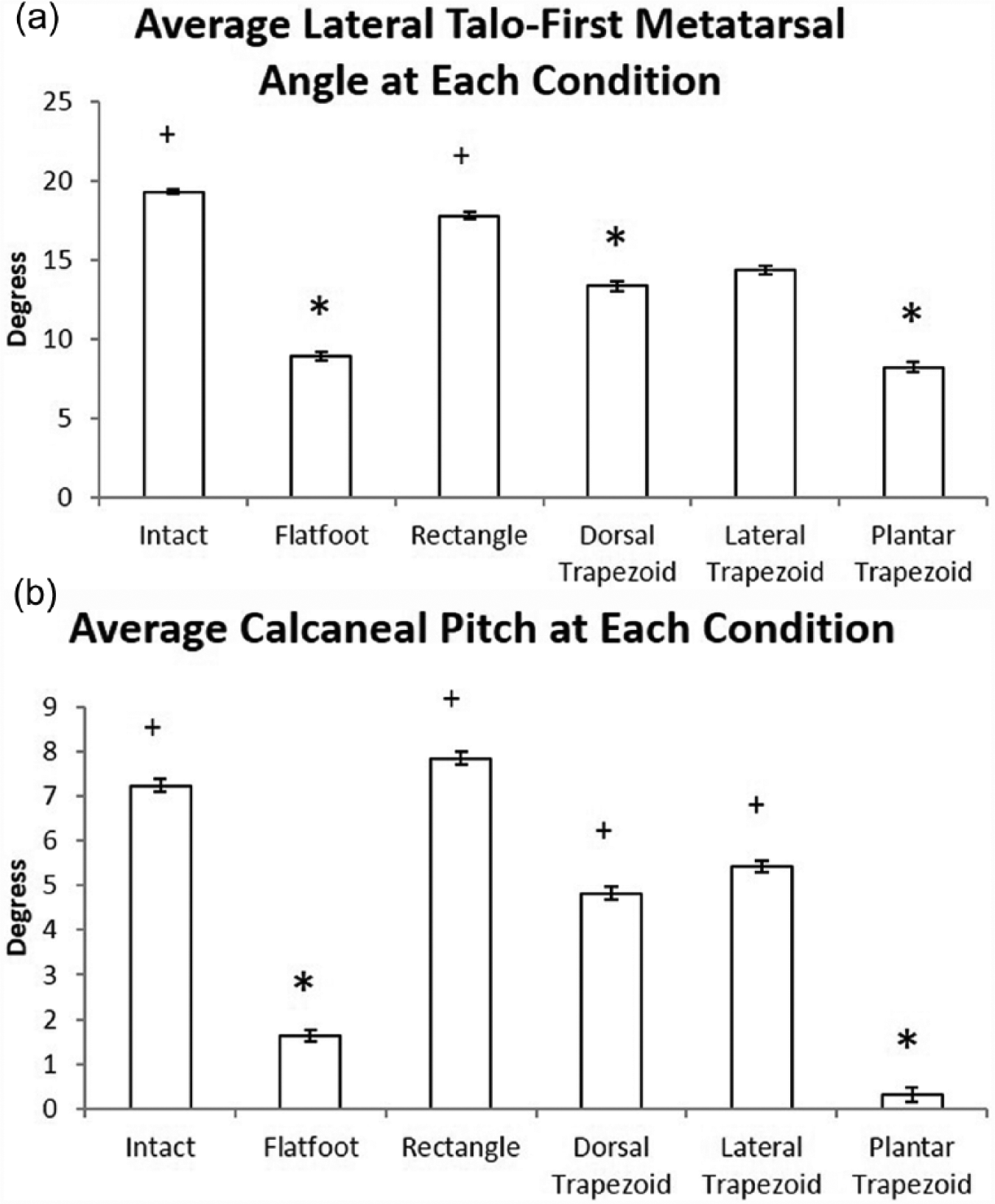
Histograms showing (a) average lateral talo-first metatarsal angle and (b) average calcaneal pitch for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Calcaneal pitch decreased significantly after creation of the flatfoot model. The rectangular, lateral, and dorsal trapezoidal grafts restored calcaneal pitch to the intact condition. Grafting with the plantarly angled trapezoidal graft resulted in angles significantly less than intact specimens and no greater than the flatfoot condition (Figure 4b).
Forefoot Abduction
The AP talo-first metatarsal angle increased significantly from intact after flatfoot creation. After LCL with the rectangular, dorsal, and lateral grafts, there was no significant difference in this angle from intact specimens; however, only the rectangular graft resulted in an angle statistically different from the flatfoot condition. The plantar trapezoidal wedge did not restore the AP talo-first metatarsal angle to the intact condition, and resulted in an angle that was not significantly different from the flatfoot condition (Figure 5).
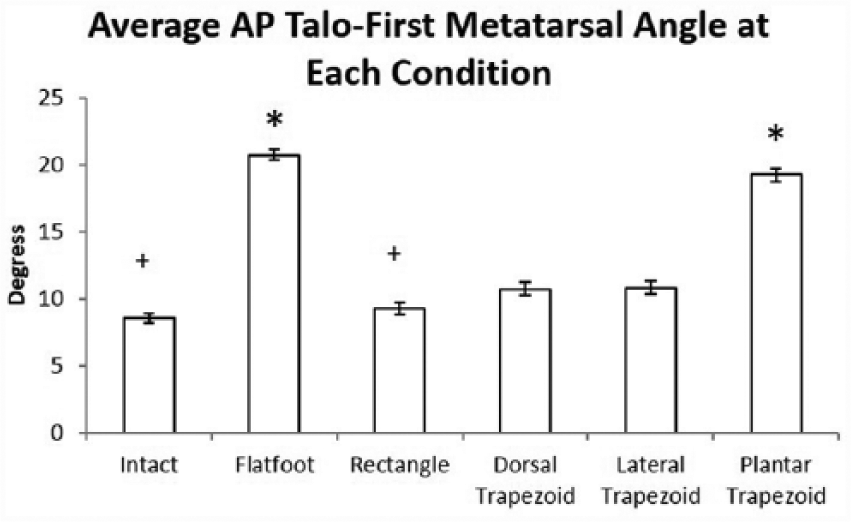
Histogram showing average anterior-posterior (AP) talo-first metatarsal angle for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Hindfoot Valgus
The AP talo-calcaneal angle did not change significantly after creation of the flatfoot model. It did increase significantly from the intact condition after rectangular, lateral, and plantar grafting, and from the flatfoot condition with lateral grafting (Figure 6). The lateral talo-calcaneal angle did not change significantly during any phase of testing (P > 0.05).
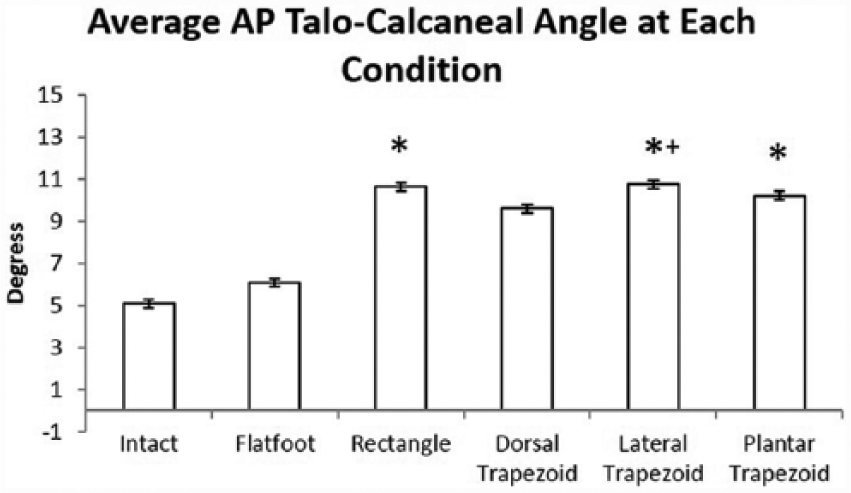
Histogram showing average anterior-posterior (AP) talo-calcaneal angle for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Spring Ligament Length
The length of the spring ligament increased significantly from intact after flatfoot creation. After LCL, it was significantly longer than intact with all graft types. The plantar and lateral grafts significantly increased the spring ligament length when compared to the flatfoot state (Figure 7).
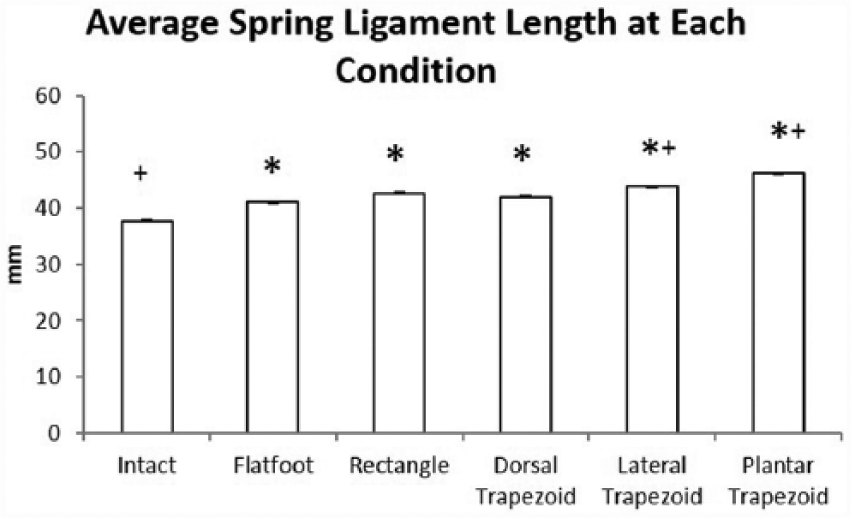
Histogram showing average spring ligament length for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Average Contact Pressure and Area
Average contact pressure across the subtalar joint decreased significantly after creation of the flatfoot at 600, 800, and 1000 N loads. After LCL, contact pressure was significantly less than the intact and the flatfoot conditions for all graft shapes at all loads tested except for the rectangular graft at 200 N (Table 1). For the talonavicular joint, flatfoot creation did not significantly change contact pressure. After LCL, contact pressure across the talonavicular joint decreased significantly compared to the intact and flatfoot conditions with all grafts (Figure 8).
Subtalar Joint Average Contact Pressure.
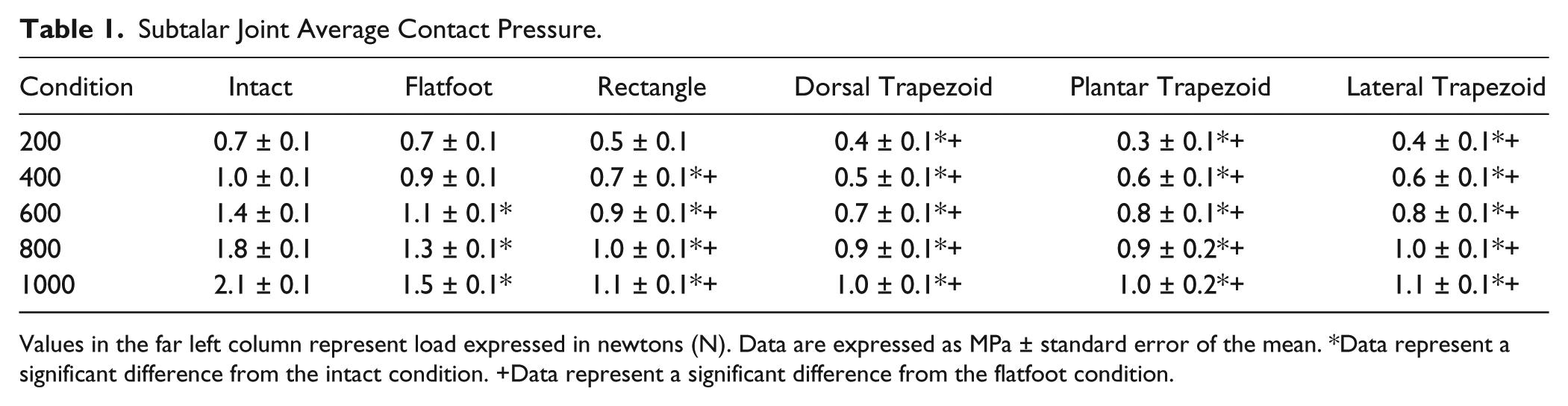
Values in the far left column represent load expressed in newtons (N). Data are expressed as MPa ± standard error of the mean. *Data represent a significant difference from the intact condition. +Data represent a significant difference from the flatfoot condition.
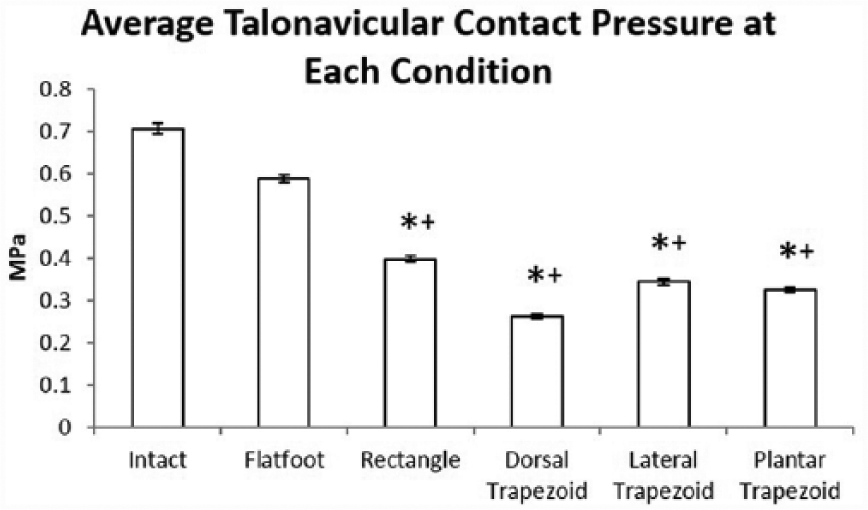
Histogram showing average talonavicular contact pressure for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Average contact area across the subtalar joint decreased significantly from the intact condition only with the dorsal trapezoidal graft (Figure 9a). For the talonavicular joint, all grafts decreased contact area significantly from intact. The rectangular, dorsal, and plantar grafts decreased contact area from the flatfoot condition. (Figure 9b).
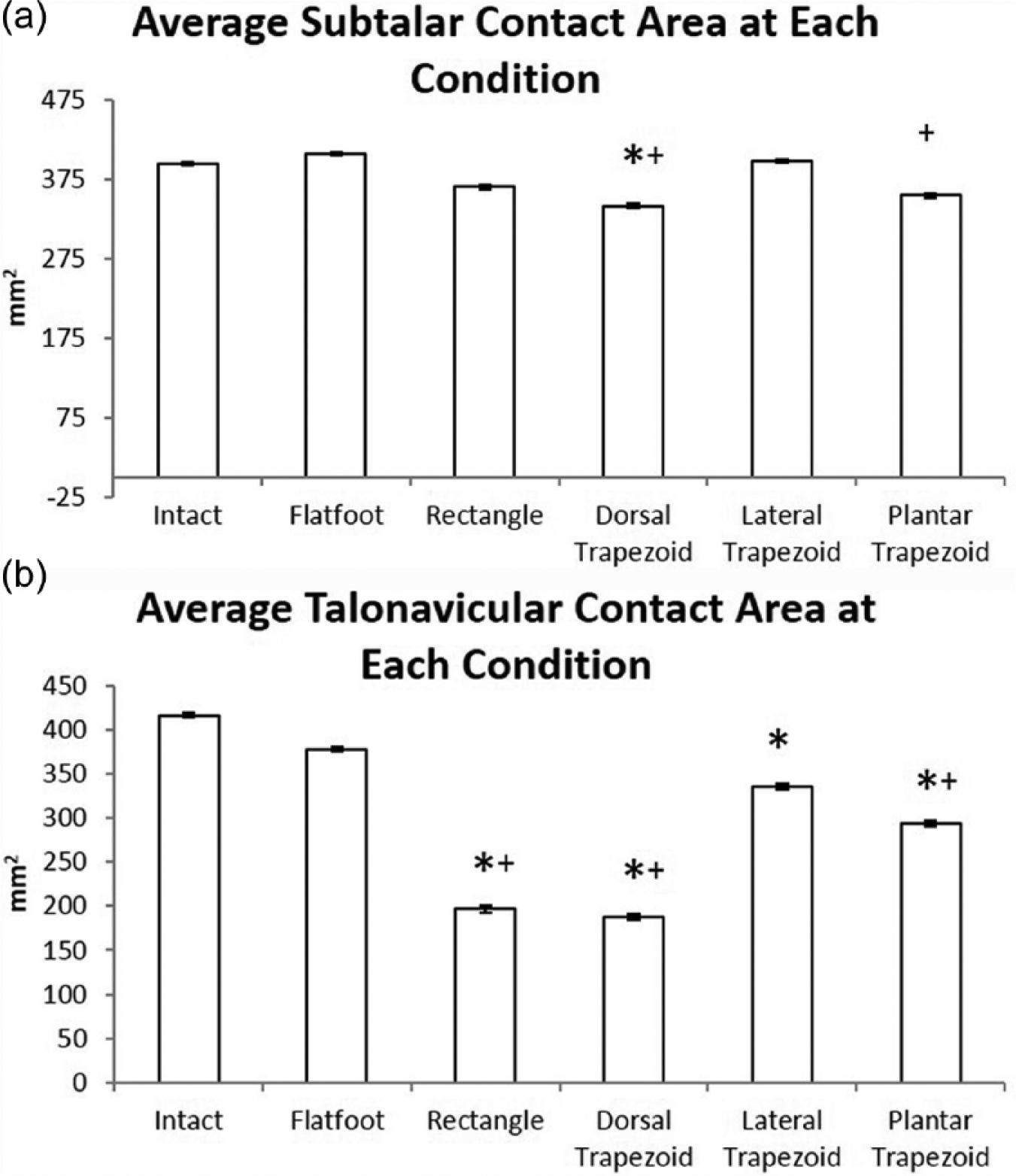
Histogram showing average (a) subtalar joint and (b) talonavicular joint contact area for each condition. Error bars represent standard error of the mean. *Data are significantly different from the intact condition. +Data are significantly different from the flatfoot condition.
Discussion
In this study, creation of the flatfoot model resulted in a significant deformity as measured by the lateral talo-first metatarsal angle, calcaneal pitch, and AP talo-first metatarsal angle. The lateral talo-first metatarsal and AP talo-first metatarsal angles were restored best by the rectangular graft. Calcaneal pitch was restored by the rectangular, dorsal, and lateral trapezoidal grafts. The trapezoidal graft oriented plantarly did not restore these angles. In the talonavicular joint, flatfoot creation did not significantly alter contact pressure or area, however pressure did decrease significantly after LCL. Contact area in the talonavicular joint also decreased after LCL. In the subtalar joint, contact pressure decreased in many testing conditions after flatfoot creation, and decreased even further after LCL; contact area was not affected by flatfoot creation and minimally affected by LCL.
In a study by DuMontier et al, 8 a flatfoot model was created in 3 cadaveric specimens which then underwent operative LCL via Evans procedure using a trapezoidal graft. Computed tomography was then used to determine the position of each bone in 3-dimensional space and assessed the relative changes throughout testing. The authors reported restoration of arch height, forefoot abduction, and heel valgus in all cases after LCL. 8 This is in agreement with the present study, in which we noted correction of many of the parameters used to evaluate tarsal bone position in our flatfoot model after LCL with similar methodology (our laterally oriented trapezoidal graft condition). We did find, however, that the rectangular graft was more effective at flatfoot correction than the trapezoidal, likely due to the increased distraction provided by the larger bone graft volume medially.
In another recent study, Tien et al 28 used 12 matched cadaveric feet to evaluate the changes in plantar pressures following either the Evans procedure or calcaneocuboid distraction arthrodesis for LCL. The authors noted increased lateral and decreased medial plantar pressures following both procedures, and noted that the lateral pressure produced by the Evans procedure was significantly less than calcaneocuboid distraction arthrodesis. 28 This was confirmed in a study by Benthien et al, 5 who determined that in 12 cadaveric feet, LCL increased lateral plantar pressure significantly. Their work also included evaluation of the effects of subsequent medial cuneiform osteotomy, which reduced lateral plantar pressure so that it was not significantly different from normal feet. 5 In other work, Xia et al 30 found additional evidence supporting lateral column overload following LCL by measuring calcaneocuboid pressures. They found significantly increased calcaneocuboid pressures in 6 cadaveric specimens following creation of a flatfoot model, which remained elevated in many of the authors’ testing conditions after LCL with a laterally oriented trapezoidal graft. 30 The authors also evaluated the effects of graft size by progressively increasing the width of the lateral side of the graft during testing. This resulted in peak calcaneocuboid pressures most similar to the intact state with an 8 mm graft, but the authors did not quantitatively evaluate restoration of bony position. 30 In the current study, we identified decreased talonavicular contact pressure following LCL. Although this has not been measured in previous literature, it is consistent in the sense that the redistribution of forces which overloads the lateral calcaneocuboid joint also decreases pressure across the medial talonavicular joint, as the navicular and cuboid have been shown to move in unison. 8 If this decrease in contact pressure is related to the redistribution of forces, future studies could better definitively outline this relationship. We also compared a 10 mm (maximum thickness) trapezoidal graft to a 10 mm rectangular graft and demonstrated better bony realignment with the latter, which has not described previously.
There are several limitations of this study. As with all cadaveric studies, specimens were tested in the time-zero state, and it was not possible to study the contribution of soft-tissue or bony healing. In addition, our flatfoot model is a simplification of the in vivo state: only the PT tendon was loaded, and much of the soft tissue about the ankle was removed to identify bony landmarks. We did not attempt to dynamically load musculature spanning the ankle, nor did we attempt to elucidate variations in our measured parameters during a simulated gait cycle. While our method for flatfoot creation was effective at producing longitudinal arch collapse and forefoot abduction, only 1 of 2 the parameters used to evaluate hindfoot valgus (lateral talo-calcaneal angle) increased significantly from the intact state, and talonavicular contact pressure did not change from the intact state; this may limit the conclusions that can be drawn regarding the effect of graft shape on these parameters. In addition, it should be noted that the parameters used to evaluate bony position in this study were named after their radiographic equivalents; however, as these data were recorded based on superficial bony landmarks, the absolute value of the various parameters cannot be directly compared to radiographic data. Another limitation is the fact that each cadaver was subjected to LCL with 4 different grafts, and no radiographs were obtained to confirm construct integrity. While this could have affected fixation strength, we did not notice any graft slippage during testing. In addition, our goal was not to provide the stability that would be required in a clinical situation, but rather to assess the secondary parameters of bony position and intra-articular pressure based on graft shape. Finally, the sequence of axially loading specimens from 200 to 1000 N was performed sequentially instead of randomly, although measurements were obtained twice to ensure reproducibility.
In conclusion, this study showed correction of tarsal bone position and decreased talonavicular pressure following LCL in a flatfoot model. We demonstrated a rectangular graft better restored bony alignment than a trapezoidal graft of similar maximum width. In a clinical situation, increasing graft volume medially may lead to better correction of a flatfoot deformity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study provided by a grant from the Veterans Affairs Rehabilitation Research and Development Merit Review. The funding source did not play a role in the investigation.