
Abstract
Background:
Reduction and stabilization of the syndesmosis in unstable ankle fractures is important for ankle mortise congruity and restoration of normal tibiotalar contact forces. Of the syndesmotic ligaments, the posterior inferior tibiofibular ligament (PITFL) provides the most strength for maintaining syndesmotic stability, and previous work has demonstrated the significance of restoring PITFL function when it remains attached to a posterior malleolus fracture fragment. However, little is known regarding the nature of a PITFL injury in the absence of a posterior malleolus fracture. The goal of this study was to describe the PITFL injury pattern based on magnetic resonance imaging (MRI) and intraoperative observation.
Methods:
A prospective database of all operatively treated ankle fractures by a single surgeon was used to identify all supination-external rotation (SER) types III and IV ankle fracture patients with complete preoperative orthogonal ankle radiographs and MRI. All patients with a posterior malleolus fracture were excluded. Using a combination of preoperative imaging and intraoperative findings, we analyzed the nature of injuries to the PITFL. In total, 185 SER III and IV operatively treated ankle fractures with complete imaging were initially identified.
Results:
Analysis of the preoperative imaging and operative reports revealed 34% (63/185) had a posterior malleolus fracture and were excluded. From the remaining 122 ankle fractures, the PITFL was delaminated from the posterior malleolus in 97% (119/122) of cases. A smaller proportion (3%; 3/122) had an intrasubstance PITFL rupture.
Conclusions:
Accurate and stable syndesmotic reduction is a significant component of restoring the ankle mortise after unstable ankle fractures. In our large cohort of rotationally unstable ankle fractures without posterior malleolus fractures, we found that most PITFL injuries occur as a delamination off the posterior malleolus. This predictable PITFL injury pattern may be used to guide new methods for stabilizing the syndesmosis in these patients.
Level of Evidence:
Level IV, case series.
Ankle fractures are common lower extremity injuries.1,10,15,29,31,38 Twenty-three percent of all ankle fractures involve disruption to the syndesmosis,11,30 and 39% of supination-external rotation (SER) type IV ankle fractures demonstrate syndesmotic instability. 35 Disruption of the syndesmosis can lead to diastasis of the distal tibiofibular joint and an asymmetric ankle mortise.3,26 Restoring the proper tibiofibular spatial relationship is critical to avoid the subsequent development of posttraumatic arthritis and long-term complications.17,28,33
Despite the frequency of syndesmotic instability, its treatment has been challenging. Several studies have been performed to determine effective methods for reduction and fixation of the syndesmosis.* Trans-syndesmotic screw fixation has been recommended and is currently the gold-standard technique.2,24,34 However, trans-syndesmotic screw fixation has been associated with fibular malreduction in up to 52% of patients and abnormal fibular motion during the gait cycle, both of which may lead to an increased rate of posttraumatic arthritis.8,11,14,19,21,33 In addition, trans-syndesmotic screws are frequently removed prior to weight bearing, which requires an additional surgical procedure.18,22 The technique of trans-syndesmotic fixation using suture endobutton devices attempts to improve on the shortcomings of trans-syndesmotic screw fixation.23,32 However, issues with malreduction and nonanatomic biomechanics may persist, and further studies are needed regarding this technique. Because of the increased morbidity associated with the use of trans-syndesmotic screws, determining more anatomic methods of syndesmosis reduction and stabilization may improve patient outcomes.
Of the ligamentous components comprising the syndesmosis, the posteroinferior tibiofibular ligament (PITFL) has been shown to be the most important by providing the greatest strength and stability to the syndesmosis. 26 Previous studies have examined syndesmotic stabilization in rotationally unstable ankle fractures through fixation of the posterior malleolus fracture fragment with its intact PITFL. This technique was demonstrated to have superior construct stiffness over syndesmotic screws in a cadaveric model. 7 Also, clinical outcomes were similar between posterior malleolus fixation and trans-syndesmotic screw fixation without the need for an additional procedure often required for removal of syndesmotic screws. 20 These results highlight the importance of the PITFL for the biomechanical function of the syndesmosis and suggest that restoration of the PITFL in rotationally unstable ankle fractures is an acceptable alternative for syndesmotic stabilization.
Although previous work has focused on the importance of the PITFL in unstable ankle fractures when an intact PITFL was attached to a posterior malleolus fracture,7,20 little is known regarding the nature of a PITFL injury in the absence of a posterior malleolus fracture. The purpose of our study was to describe the PITFL injury pattern using magnetic resonance imaging (MRI) and intraoperative observations.
Methods
After approval by the institutional review board, a prospective database of all operatively treated ankle fractures by a single surgeon from 2010 through 2013 was reviewed. Skeletally mature patients who underwent internal fixation of supination external rotation (SER) III and IV ankle fractures according to the Lauge-Hansen classification 16 were selected for further evaluation. All patients included in the study had complete preoperative imaging, which included orthogonal ankle radiographs and MRI. We initially identified 185 SER III and IV ankle fractures with complete preoperative imaging. Of these, 63 patients (34%) had posterior malleolus fractures. In all cases of posterior malleolus fractures, the PITFL was noted to be intact and attached to the fracture fragment at the time of surgery, consistent with previous results. 20 The remaining 122 patients with PITFL injuries were used for further analysis. The average patient age was 47 years (range, 15-87 years), with 68 females (56%) and 54 males (44%). Twenty patients (16%) had tibiotalar dislocations at presentation.
A fellowship-trained musculoskeletal radiologist retrospectively evaluated all MRIs for the presence of a PITFL injury and describe its injury characteristics, being blinded to the operative notes. If a PITFL rupture was observed, the location of the rupture was recorded as an intrasubstance tear or a tear from the tibia or fibula.
Analysis of the PITFL injury was also performed intraoperatively during surgical fixation of the ankle fracture. Our preferred technique for open reduction and internal fixation of SER ankle fractures included a posterolateral approach to the ankle. The fibula was reduced and typically fixed with a 2.7-mm reconstruction plate placed posteriorly in an antiglide fashion. Following fibula fixation, the posterolateral dissection was taken medially to the PITFL. In the absence of a posterior malleolus fracture, the competence of the PITFL was assessed by direct visualization. When the PITFL was found to be incompetent due to disruption from its broad tibial attachment (Figure 1), a 3.5-mm cortical screw with a spiked polyetheretherketone (PEEK) soft tissue washer was used to restore the PITFL attachment to the posterior malleolus (Figures 2 and 3). In cases where the PITFL sustained an intrasubstance rupture, syndesmotic screws were used to provide syndesmotic stability if the syndesmosis was determined to be unstable with manual stress maneuvers. The status of the PITFL and location of the injury based on intraoperative findings were recorded by the attending surgeon immediately after the case.
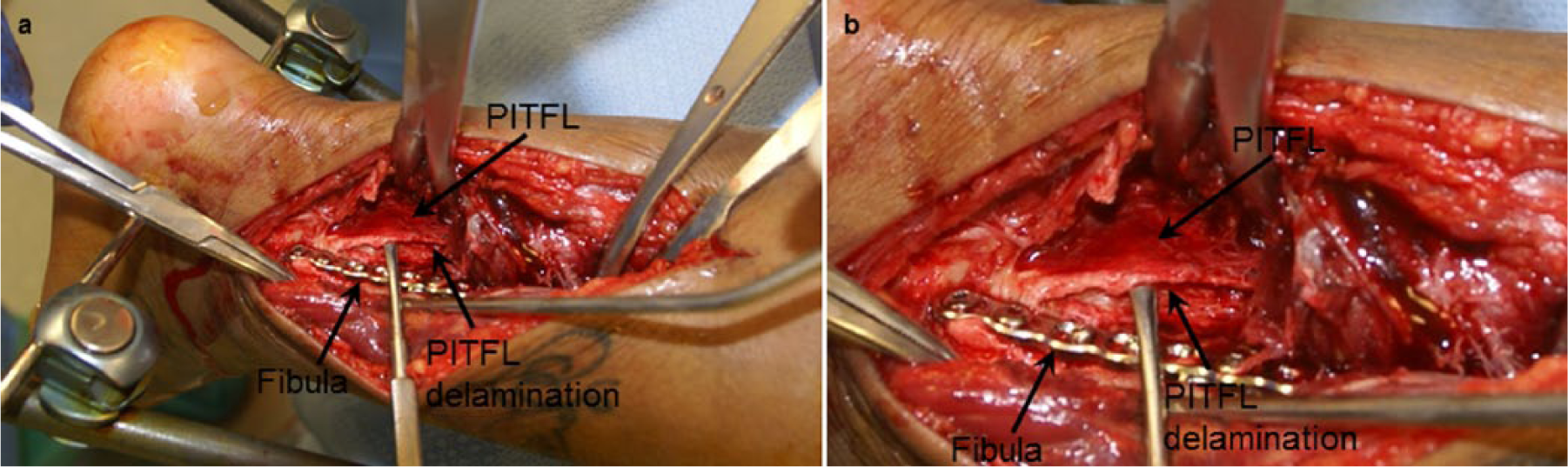
Intraoperative images of posterior inferior tibiofibular ligament (PITFL) delamination from the posterior malleolus.

Case example of a posterior inferior tibiofibular ligament (PITFL) repair. Anteroposterior (a), mortise (b), and lateral (c) injury radiographs of an ankle fracture-dislocation with a PITFL rupture. Intraoperative fluoroscopy demonstrating residual syndesmotic widening after fixation of the lateral and medial malleoli (d), followed by syndesmotic reduction (e) and maintenance of syndesmotic reduction after PITFL repair (f, g).
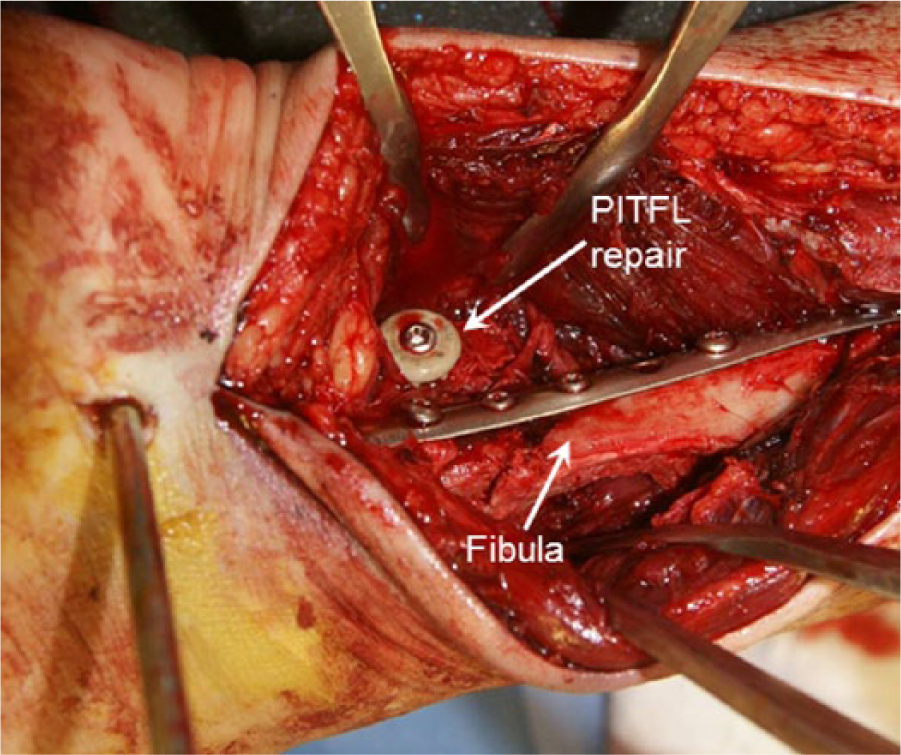
Intraoperative photograph of a posterior inferior tibiofibular ligament (PITFL) from a posterior-lateral approach.
To evaluate the native anatomy of the PITFL as well confirm our intraoperative observations and preoperative imaging findings, we dissected 8 human cadaver lower extremity specimens disarticulated through the knee. The posterior soft tissues of the ankle were removed to reveal the PITFL, taking care not to disrupt its attachments. The orientation and characteristics of the ligament’s tibial insertion were recorded and photographed.
Results
Based on prospective intraoperative assessments by direct visualization, 97% (119/122) of PITFL injuries were due to a broad delamination of the ligament from its attachment to the posterior malleolus (Figure 1). The remaining 3% (3/122) of PITFL injuries demonstrated intrasubstance ruptures.
Analysis of preoperative MRI was performed to assess the ability of this modality to diagnose PITFL injuries compared with intraoperative assessment. Of the 122 patients with PITFL ruptures based on intraoperative assessments, 86 (70%) of these injuries were also detected by MRI, whereas 36 (30%) were not. An additional 10 patients were thought to have a PITFL injury based on MRI but intraoperatively were determined to have a small posterior malleolus fracture with an intact PITFL attached to the fracture fragment. With regard to the location of the PITFL injury based on MRI, 91 of 96 (95%) PITFL tears seen on MRI were interpreted as disruptions from the posterior malleolus (Figure 4), 3 (3%) were intrasubstance ruptures (Figure 5), and 2 (2%) were disruptions from the fibula. Using intraoperative evaluation as the gold standard, MRI was 70% sensitive and 84% specific for detection of a PITFL injury, with a positive predictive value of 90% and negative predictive value of 60%.
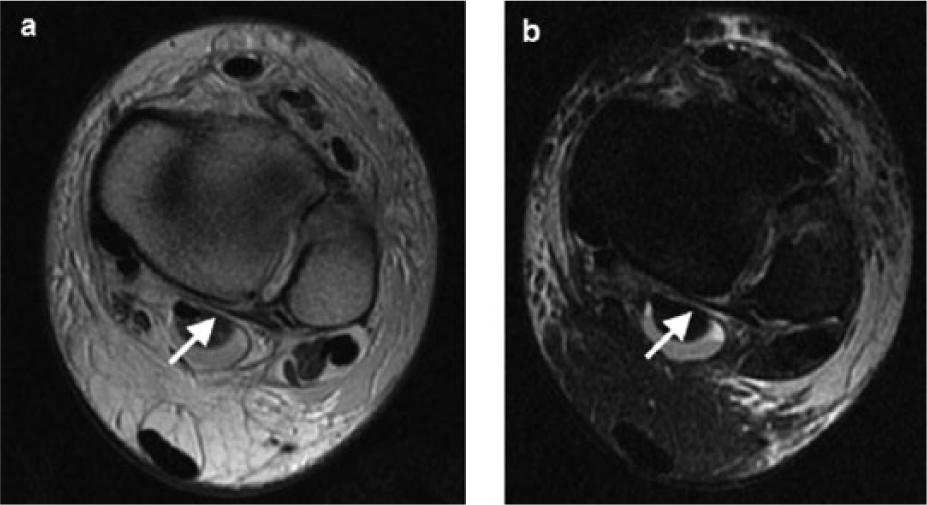
Axial proton density (a) and short tau inversion recovery (b) magnetic resonance images of posterior inferior tibiofibular ligament (arrow) delamination from the posterior malleolus.
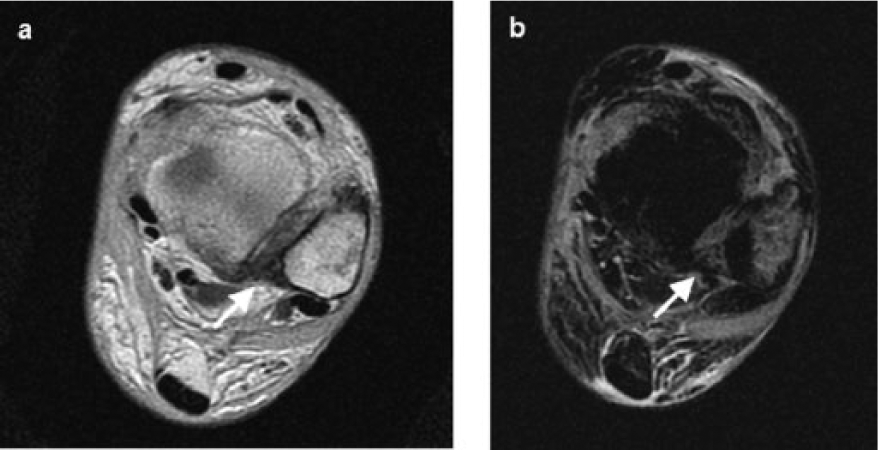
Axial proton density (a) and short tau inversion recovery (b) magnetic resonance images of an intrasubstance rupture of the posterior inferior tibiofibular ligament (arrow).
Dissections of cadaveric leg specimens were performed to qualitatively analyze the anatomy of the PITFL. In all of these specimens, the PITFL had a broad attachment extending from the posterior aspect of the fibula to the posterior malleolus (Figure 6). The fibers of the PITFL fanned out as a sleeve of tissue medially across a broad surface on the posterior malleolus and blended into the periosteum at its periphery (Figure 6).
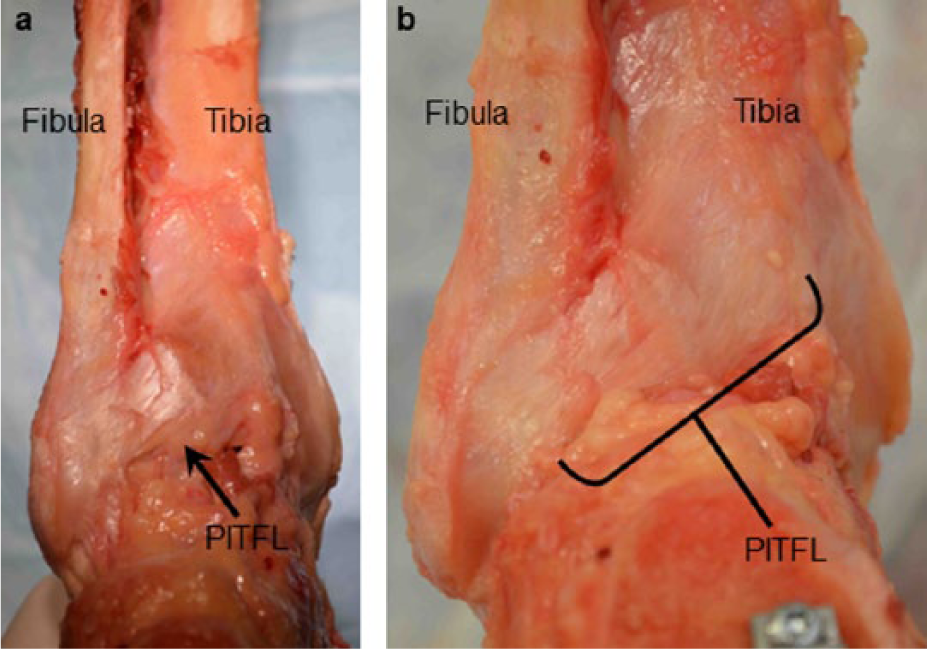
Photographs of the posterior ankle in cadaveric specimens with soft tissue removed to highlight the posterior inferior tibiofibular ligament (PITFL).
Discussion
Syndesmotic disruptions are a common component of unstable ankle fractures, and restoration of syndesmotic stability is critical for establishing proper ankle biomechanics.17,28,33 The importance of the PITFL in syndesmosis function has previously been demonstrated in biomechanical and clinical studies,7,20,26 yet little is known regarding PITFL injuries. In this study, we analyzed the nature of PITFL injuries using MRI and intraoperative observation in a large cohort of SER III and IV ankle fractures. Our results suggest a predictable PITFL injury pattern in rotationally unstable ankle fractures, with the vast majority of PITFL injuries occurring as a delamination of the ligament from its attachment to the posterior malleolus. As opposed to an intrasubstance tear, we found delamination of the essentially intact PITFL permitted its reapproximation and functional repair to the posterior malleolus.
MRI has previously been shown to be an effective means to evaluate PITFL injuries.25,37,39 Compared with direct visualization during ankle arthroscopy, MRI has been found to be 100% sensitive and 94% specific in diagnosing PITFL tears that were visualized using arthroscopy. 37 Therefore, because of its diagnostic ability, we used MRI to confirm the PITFL injury characteristics of our intraoperative findings. Intraoperative observation found 97% of PITFL injuries were delaminations off the posterior malleolus, compared with 95% by MRI analysis. However, 30% of PITFL disruptions that were seen intraoperatively were not seen with MRI. These results may reflect an increased sensitivity for detecting ligament incompetence with direct visualization and awareness of this common injury pattern. In addition, the oblique orientation of the PITFL relative to the orthogonal MRI planes may contribute to inconsistencies in diagnosing PITFL ruptures using MRI.12,13
Nevertheless, these similar findings of PITFL disruption patterns using 2 different modalities confirm the fact that in patients with unstable ankle injuries without evidence of a posterior malleolus fracture, the PITFL avulses from its posterior malleolus attachment in nearly every case. In addition, from our cadaveric dissections, the PITFL was found to have a broad insertion onto the posterior malleolus. This unique PITFL insertion morphology is consistent with the delamination injury pattern most commonly seen clinically in these patients.
In unstable ankle fractures without a posterior malleolus fracture, this study demonstrated a common injury pattern to the PITFL that was amenable to repair. We believe that repair techniques to fix the PITFL back to its footprint on the posterior malleolus may provide an effective and reproducible means to stabilize the syndesmosis. In these cases, this approach potentially could obviate the need for trans-syndesmotic screws. We believe the inferior outcomes after fixation of unstable ankle fractures and use of trans-syndesmotic fixation, either with screws or endobuttons, is in part due to a nonanatomic method of fixation. Specifically, we believe that during initiation of early range of motion without the posterior checkrein of the PITFL, ankle dorsiflexion can result in excessive rotation of the fibula within the incisura. This increased ankle instability may result in abundant disorganized scar formation, ankle joint stiffness, and reduced ankle function often seen after injury. We predict that restoring the anatomic orientation of the PITFL and reducing potential pathologic instability could improve functional outcomes in these patients.
This study has several limitations. The MRIs were analyzed retrospectively by only 1 attending musculoskeletal radiologist. However, given the fact that the MRI results were similar to our operative observations in that nearly all PITFL avulsions were from the posterior malleolus, we do not believe this is a significant limitation. Another limitation of this study is that the biomechanical and clinical relevance of this PITFL injury was not assessed, although this is a topic of current investigation. Despite these limitations, our results suggest a clearly reproducible injury pattern not yet appreciated.
In conclusion, despite recent advances in technique, imaging, and devices for reduction and stabilization of the ankle syndesmosis, consistent and favorable results are lacking. In rotationally unstable ankle injuries without a posterior malleolus fracture, the PITFL is destabilized as a delamination from its insertion on the posterior malleolus in the vast majority of cases, as determined by intraoperative observation and MRI analysis. This suggests the possibility of an alternative technique for restoring syndesmotic integrity by reapproximating the intact but delaminated ligament and reattaching it to its bony bed, thereby functionally restoring one of the major syndesmotic stabilizers. Ultimately, this more anatomic reconstruction of the syndesmotic stabilizers may provide for improved syndesmosis reduction and obviate the need for trans-syndesmotic screws.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.