
Abstract
Background:
Hallux metatarsophalangeal (MP) joint arthrodesis for hallux varus is generally reserved for severe deformity, failed surgery or the development of osteoarthritis. The purpose of this study was to determine the radiologic results of arthrodesis of the hallux MP joint following treatment for hallux varus. Our hypothesis was that in the process of correcting the hallux valgus angle, the 1-2 intermetatarsal angle (1-2 IMA) and hallux valgus angle (HVA) will be improved due to correction of the deforming forces.
Methods:
A retrospective review was performed on 26 patients with 29 feet that had symptomatic hallux varus deformities treated with arthrodesis of the hallux MP joint between September 1, 2002, and December 31, 2012. The 1-2 IMA and HVA were measured on the preoperative and most recent postoperative films and compared. Twenty-nine patients were followed with postoperative weight-bearing radiographs. Two were men and 24 were women. Twelve were performed on the right foot, 17 on the left, including 3 bilateral cases. Fourteen patients had concomitant procedures on the ipsilateral forefoot.
Results:
The average 1-2 IMA changed from 4.8 degrees to 8.4 degrees, a difference of 3.6 degrees (P < .05), and the average HVA changed from −20.7 degrees to 8.1 degrees (P < .05).
Conclusion:
Our study showed that a hallux MP joint arthrodesis in patients with hallux varus resulted in a predictable increase in the 1-2 IMA.
Level of Evidence:
Level IV, case series.
Hallux varus may be idiopathic or can occur as a sequela following overcorrected hallux valgus. Untreated, it may lead to pain and difficulty with shoe wear. The deformity at the hallux metatarsophalangeal (MP) joint can be caused by disruption of the lateral stabilizing structures or in overtightening of the medial structures during previous hallux valgus surgery.3,13 Dynamic muscular imbalance of the abductor hallucis and medial head of the flexor digitorum brevis may also contribute to hallux varus. 3 Operative treatment options include extensor hallucis longus or extensor hallucis brevis tendon transfer, a suture button technique, or hallux MP arthrodesis.10,14,15 The latter is generally reserved for severe deformity, failed surgery, or the development of osteoarthritis.
The technique of MP arthrodesis was described by McKeever in 1952, 9 and early reports were mostly restricted to those performed for a diagnosis of hallux valgus or hallux rigidus.5,7,8,16 There are more recent studies that have reported radiographic results after hallux MTP joint arthrodesis specifically performed for correction of hallux valgus deformity.2,4,6,11 They noted a change in the 1-2 intermetatarsal angle (1-2 IMA). To our knowledge, there are no studies specifically evaluating the radiographic results after MP arthrodesis for the diagnosis of hallux varus.
The purpose of this present study was to determine the radiologic results of arthrodesis of the hallux MP joint following treatment for hallux varus of any etiology. Our hypothesis was that in the process of correcting the hallux valgus angle, the deforming forces would be rebalanced and the relationship between the hallux and second metatarsals would be restored as measured by the IMA and HVA.
Methods
Following institutional review board approval, a retrospective review was performed to identify patients who had symptomatic hallux varus deformities refractory to conservative treatment and were treated with arthrodesis of the hallux MP joint. A search of the database between 2002 and 2012 identified 26 patients with 29 surgeries who had hallux MP arthrodesis for a diagnosis of hallux varus. Patients without postoperative weight-bearing radiographs and those with hallux MP arthrodesis for any diagnosis other than hallux varus were excluded. Demographic variables including concomitant procedures, the etiology of hallux varus, and the fixation construct were also identified.
Twenty-nine patients were included for study, consisting of 2 men and 24 women. Nine surgeries were performed on the right foot, 14 on the left, and 3 were bilateral. Hallux varus was idiopathic (in the absence of any prior forefoot surgery) in 9, iatrogenic in 18, and due to rheumatoid arthritis in 2. Sixteen patients had concomitant procedures on the ipsilateral forefoot—14 had distal metatarsal shortening osteotomies, 1 had a metatarsal head resection, 2 had hammertoe corrections, 1 had a bunionette procedure, and 1 had interposition arthroplasties of the second and third MP joints. Nine patients had a crossed screw construct, 7 had a dorsal plate alone, and 13 had a crossing screw with a dorsal plate. The 9 patients with the crossed screw configuration were the first patients in the series after which the author’s technique progressed to a dorsal plate to allow for immediate weight-bearing postoperatively. At this time, the surgeon’s preference is to place a single crossed compression screw with a dorsal plate. Occasionally the anatomy of the patient and the deformity did not allow for a crossed screw and in that case a dorsal compression plate was placed in isolation.
Operative Technique
All patients were treated with a similar approach. A dorsal incision was made centered over the hallux MP joint. Preparation of the joint was performed by fashioning the surfaces into a cup and cone either with a reamer system or with a burr depending on the quality of the bone. Fixation progressed from a crossed screw configuration to dorsal plate fixation with time.
The position of the fusion was ideally placed in neutral to slight valgus depending on the position of the lesser toes and patient preference. Attention was made to ensure that the fusion was not placed into varus since it is common to underestimate the corrected position of the MP joint and place it in too much varus (Figure 1).
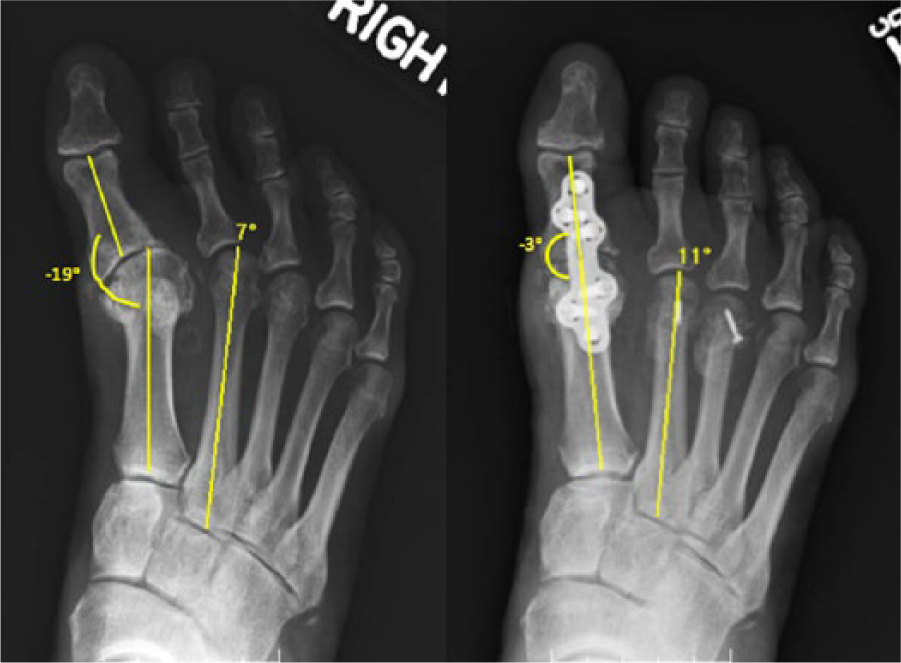
Preoperative and postoperative AP radiographs of a patient with an undercorrected HVA—a common error following fusion for hallux varus.
The postoperative protocol was surgeon and surgery dependent. In general, patients treated with a dorsal plate were made non-weight-bearing initially in a postoperative shoe with a heel wedge to allow heel weight-bearing for a total of 12 weeks. They were then transitioned to full weight-bearing in a comfortable shoe.
Outcomes
Weight-bearing AP radiographs of the foot were performed and the 1-2 IMA and hallux valgus angle (HVA) were measured on the most recent preoperative and postoperative films as described by the Ad Hoc Committee of the American Orthopedic Foot and Ankle Society on Angular Measurements. 1 All the measurements were made by a foot and ankle fellow using the measuring tools with the AMICAS PACS Light View Clinical Viewer v.6 (Merge Healthcare, Hartland, WI) used for our digital radiographs (Figures 1 and 2). Radiographs were obtained at an average of 13.3 months after surgery and there were no nonunions noted on final postoperative radiographs.
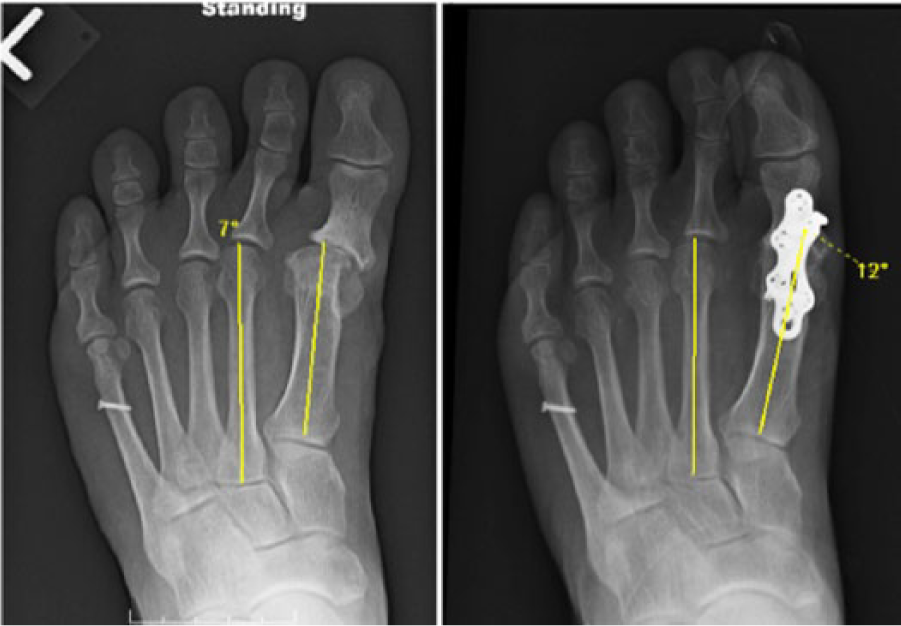
Preoperative and postoperative AP radiographs of a patient with iatrogenic hallux varus demonstrating an increase in the measured 1-2 IMA.
Data were analyzed with a 2-tailed paired Student’s t test comparing preoperative and postoperative measurements. A subgroup analysis was performed using an unpaired Student’s t test to evaluate whether the etiology of hallux varus, the presence of concomitant procedures, or the type of fixation had any effect. Significance was set at P < .05.
Results
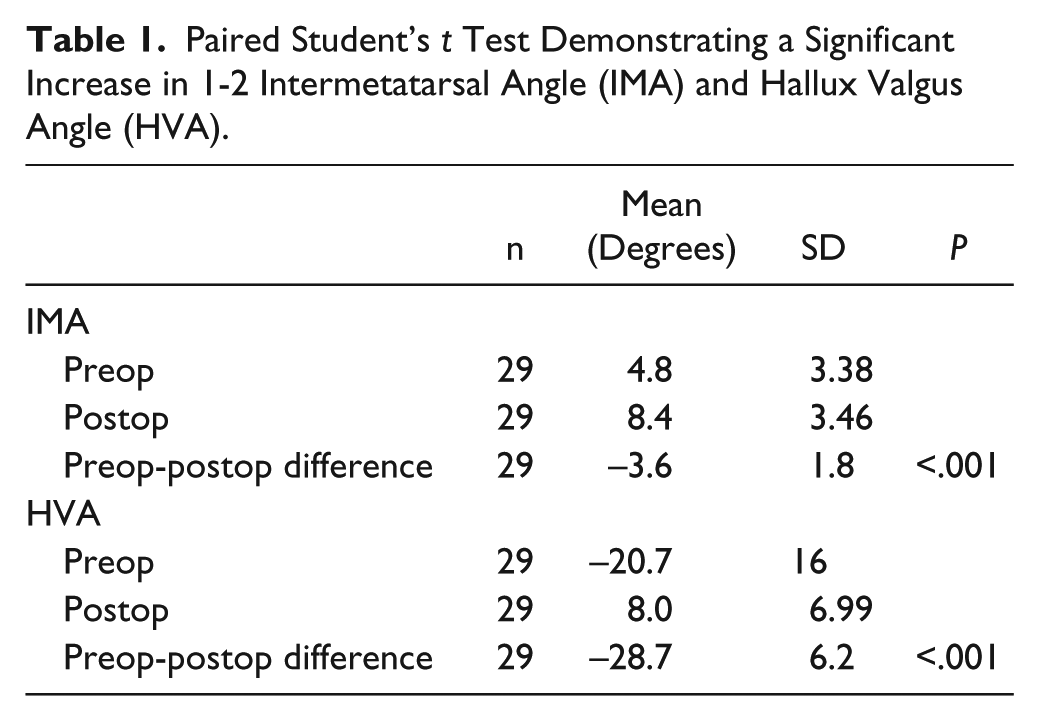
Average 1-2 IMA improved from 4.8 degrees to 8.4 degrees, a difference of 3.6 degrees (P < .05). Average HVA improved from −20.7 degrees to 8.1 degrees (P < .05) (Table 1). Subgroup analysis comparing iatrogenic versus idiopathic hallux varus, the presence of concomitant procedures, and plate versus screw fixation showed no significant difference (Table 2, Figures 2 and 3).
Paired Student’s t Test Demonstrating a Significant Increase in 1-2 Intermetatarsal Angle (IMA) and Hallux Valgus Angle (HVA).
Unpaired Student’s t Test Showed No Significant Difference When Comparing Etiology, Type of Fixation, or Presence of Concomitant Procedures.
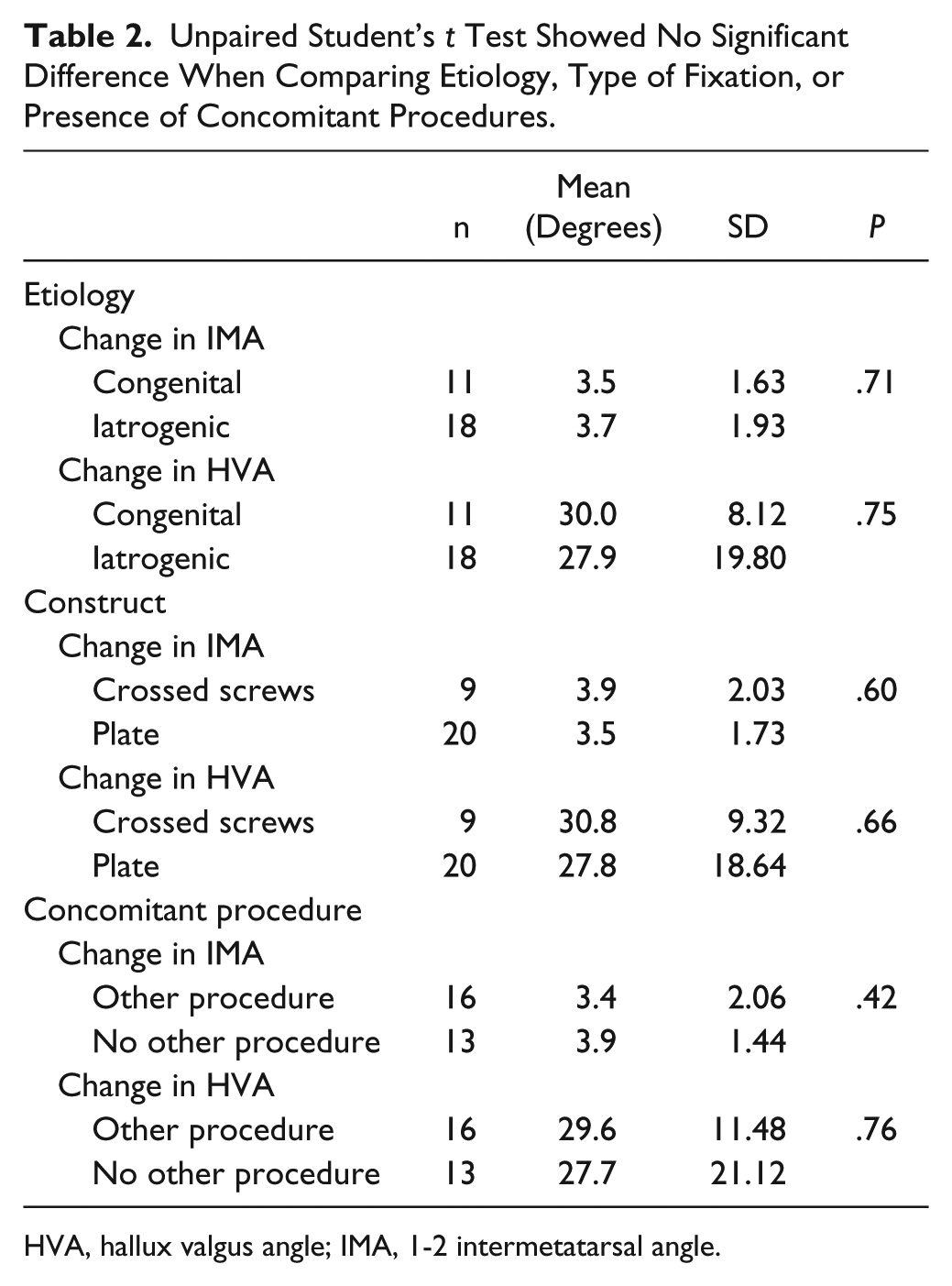
HVA, hallux valgus angle; IMA, 1-2 intermetatarsal angle.
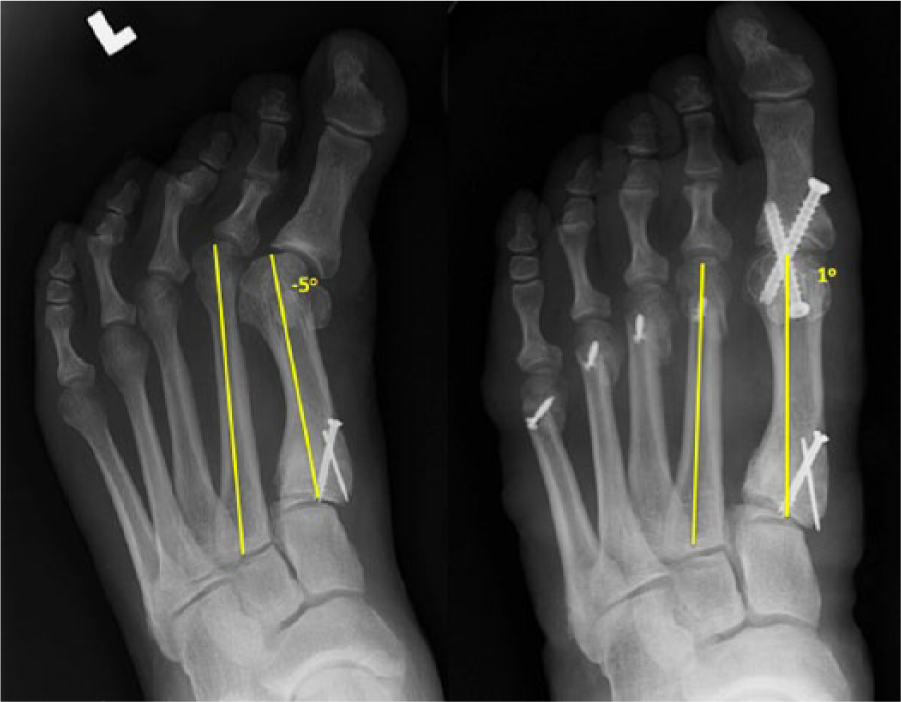
Preoperative and postoperative AP radiographs of a patient with iatrogenic hallux varus demonstrating an increase in the measured 1-2 IMA.
Discussion
The purpose of this study was to determine the radiologic results of arthrodesis of the hallux MP joint as treatment of hallux varus. Our study has shown that arthrodesis in this setting predictably increased the 1-2 IMA. This suggests that during the procedure as the HVA was corrected, the deforming forces, including the abductor hallucis and flexor digitorum brevis, were realigned and subsequently the 1-2 IMA was corrected to its normal position.
The treatment for hallux varus is vast and can include soft tissue procedures, the use of suture button constructs, or arthrodesis. One of the largest studies to date on the treatment of hallux varus was published by Skalley and Myerson, 14 in which they evaluated 45 feet with multiple causes of hallux varus treated with soft tissue procedures and tendon transfers. They recommended tendon transfer in the young, active patient without arthritis with maintained range of motion. The use of a hallux MP arthrodesis for the treatment of hallux varus was discussed as early as 1989 when Mills and Menelaus 10 reviewed their results of 12 patients with hallux varus after an average follow-up of 12.7 years. Included in this evaluation was arthrodesis performed in 3 patients with satisfactory outcomes. Arthrodesis is generally reserved for severe deformity, failed surgery or the development of osteoarthritis.
Most early reports of hallux MP arthrodesis are restricted to those performed for a diagnosis of hallux valgus or hallux rigidus.5,7,8,16 There are also more recent studies that have reported radiographic results after hallux MTP joint arthrodesis,2,4,6,11 specifically the change in the 1-2 IMA. Mann et al evaluated the results of MP arthrodesis for any indication including hallux valgus, hallux rigidus, rheumatoid arthritis. In their study, they only included 1 patient with a diagnosis of hallux varus. 6 Cronin et al 2 evaluated the radiographic results after MP arthrodesis in 20 patients, all of which had a diagnosis of hallux valgus. Results of this study showed a mean change of 8.22 degrees in the IMA. Similarly, Pydah et al 11 evaluated 69 feet following MP arthrodesis for hallux valgus deformity showing an average improvement of 4.4 degrees in the 1-2 IMA. Riggs and Johnson 12 followed 206 patients treated with hallux MP arthrodesis for hallux valgus and showed a 4 degree correction on postoperative radiographs.
To our knowledge, there are no studies specifically evaluating the radiographic results after MP arthrodesis for the diagnosis of hallux varus. Those that include hallux varus in their evaluation have very few patients making it difficult to draw any conclusions. Our study presents the radiographic outcomes of 29 patients treated with hallux MP arthrodesis for hallux varus, revealing an increase in 1-2 IMA by 3.6 degrees. This is fairly similar to the change reported by the above studies in correction of the 1-2 IMA for hallux valgus.
One limitation of our study includes the fact that it was retrospective in nature. We also included patients who had concomitant procedures, but our analysis did not suggest that this should have altered our results. Hypothetically, patients with a distal metatarsal osteotomy may have a change in the 1-2 IMA due to a shift of the second metatarsal rather than correction of the hallux. However, our measurements were made per the Ad Hoc Committee of the AOFAS recommendations. They state that the second metatarsal reference points should be metaphyseal/diaphyseal and 1-2 cm proximal to the distal articular surface to avoid any effect of a distal metatarsal head excision or osteotomy. 1 We feel that the inclusion of these cases had a negligible effect on our results, particularly since subgroup analysis showed no difference between those with and without concomitant procedures.
In conclusion, our study showed that a hallux MP joint arthrodesis in patients with hallux varus resulted in a predictable increase in the 1-2 IMA. We believe that this was due to a correction of the deforming forces after realignment of the hallux MP joint.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mark S. Myerson, MD, reports grants and personal fees from Tornier, personal fees from BME, personal fees from Orthohelix, personal fees from Biomet, outside the submitted work.