
Abstract
Background:
Preoperative computer navigation and patient-specific instrumentation have had promising results in total knee arthroplasty and in a previous cadaveric total ankle arthroplasty (TAA) study. Potential benefits of patient-specific guides include improved implant alignment and decreased surgical time. The purpose of this retrospective case series was to evaluate the accuracy, reproducibility, and limitations of TAA tibia and talar implant placement and radiographic alignment using preoperative computed tomography (CT) scan–derived instrumentation in a clinical setting.
Methods:
Between 2012 and 2014, 42 consecutive TAA cases in 42 patients using preoperative CT scan–derived patient-specific plans and guides (PROPHECY, Wright Medical Technology, Memphis TN) were reviewed from a single center of foot and ankle fellowship–trained orthopaedic surgeons. TAA implants used included 29 intramedullary referencing implants (INBONE II, Wright Medical Technology) and 13 low-profile tibia and talar resurfacing implants (Infinity, Wright Medical Technology). All patients had standardized preoperative CT scans before surgery that were used to create custom surgical plans and 3-dimensional solid cutting guides and models. All patients had a minimum 3-month follow-up with weightbearing postoperative radiographs. Patient demographics were recorded, and coronal and sagittal alignments were compared among weightbearing preoperative radiographs, CT scan–derived surgical plans, and weightbearing postoperative radiographs using a digital picture archiving and communication system.
Results:
Average age for all patients was 63 ± 9 years, with a body mass index of 29.8 ± 5.9. Average total surgical time for all TAAs was 100 ± 11 minutes, with Infinity TAAs taking less time than INBONE II TAAs (92 vs 104 minutes; P < .05). Average preoperative coronal alignment was 1.9 degrees varus ± 6.4 (range, 14 degrees valgus to 10 degrees varus). Postoperative weightbearing alignments for all TAA cases were within ±3° of the predicted coronal and sagittal alignments from the CT scan–derived surgical plans. There were no significant differences in pre- or postoperative weightbearing alignments between INBONE II and Infinity TAA cases. Neutral coronal and sagittal alignments were obtained for all TAA cases regardless of preoperative deformity. Patient-specific surgical plans were accurate to within 1 size for tibia and talar implants used. Surgical plans predicted the actual tibia implant size used in 100% of INBONE II cases and 92% of Infinity cases. Plans were less accurate for talar implants and predicted the actual talar implant size used in 76% of INBONE II cases and 46% of Infinity cases. In all cases of predicted tibia or talar size mismatch, surgical plans predicted 1 implant size larger than actually used.
Conclusions:
Results from this study provide early clinical evidence that preoperative CT scan–derived patient-specific surgical plans and guides can help provide accurate and reproducible TAA radiographic alignments. Talar implant sizing was not as accurate due to individual surgeon preference regarding the extent of gutter debridement. Similar to other modern computer navigation and patient-specific instrumentation systems, final coronal and sagittal alignments were within 3 degrees of the predicted surgical plans, and sizing was accurate within 1 implant size. Future studies are warranted to investigate the clinical and functional implications of patient-specific TAA and the overall cost-effectiveness of this technique.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Preoperative computer navigation, templating, and patient-specific instrumentation have all shown promising results in total knee and hip arthroplasty with accurate and reproducible radiographic outcomes.2,4,10,13,16-19 A standard of ±3 degrees has been established as the maximum amount of allowable implant alignment and positional error.2,4,10,13,16-19 The goal of patient-specific instrumentation is to restore mechanical and kinematic joint axes. 19 Proposed benefits include improved implant alignment, decreased operative time, more efficient surgical planning, and lower cost. 18
In recent years, preoperative computed tomography (CT) scan–derived patient-specific plans and guides (PROPHECY, Wright Medical Technology, Memphis, TN) have been developed for total ankle arthroplasty (TAA) and approved by the Food and Drug Administration. Cadaveric study results have shown that these patient-specific guides can provide reliable and reproducible placement of TAA implants to within 2 degrees of preoperative plans. 3 However, no studies have evaluated the outcomes of TAA patient-specific guides in a clinical setting. This purpose of this retrospective case series was to evaluate the accuracy, reproducibility, and limitations of preoperative CT scan–derived instrumentation for TAA using 2 implant systems in patients with end-stage ankle arthritis.
Methods
This study was approved by the Institutional Review Board prior to initiation. Between 2012 and 2014, 42 consecutive TAA cases in 42 patients (22 female, 20 male) were reviewed from a single center of foot and ankle fellowship–trained orthopaedic surgeons. All patients had standardized preoperative CT scans before surgery that were used to create custom surgical plans and 3-dimensional solid cutting guides and models (PROPHECY). All CT scans followed a detailed protocol developed by the device manufacturer that included 2.5-mm slice increments at the knee 5 cm proximal and distal to the knee joint line, in addition to 1.25-mm slice increments from 10 cm above the ankle joint through the ball of the foot, including the toes.
For each scan, the foot was positioned in a holder in neutral position 90 degrees relative to the leg. Magnification was standardized to a known marker size to reduce size discrepancy and obtain accurate measurements of native bony anatomy. Individual patient CT data were converted into 3-dimensional computer models to create a virtual operative procedure with implant sizes, positioning, and alignment based on individual surgeon preferences. Computer analysis of the CT data evaluated the tibia and talus together as well as separately to create 3-dimensional physical models. Computer-based models were then adjusted as needed by the surgeon and fabricated to create patient-specific bone models and guides for intraoperative use.
TAAs were performed using a standard anterior approach using intramedullary referencing implants (n = 29; INBONE II, Wright Medical Technology) or low-profile tibia and talar resurfacing implants (n = 13; Infinity, Wright Medical Technology). Patient-specific operative guides for the tibia and talus designed to match each patient’s tibial and talar bony anatomy were used in a standardized fashion during each case. Patient demographics and medical comorbidities were recorded, such as diabetes, coronary artery disease, hyperlipidemia, and hypertension. All patients had a minimum of 3-month follow-up with weightbearing postoperative radiographs. Standardized weightbearing anteroposterior, lateral, and mortise radiographs were taken preoperatively and at 3-month follow-up evaluation.
Average age for all patients was 63 ± 9 years, with a body mass index of 29.8 ± 5.9 (Table 1). There were no significant differences in baseline patient demographics between INBONE II and Infinity TAA groups. Average follow-up for all TAA cases at time of data analysis was 9 ± 6 months.
Surgical Data, Radiographic Outcomes, and Preoperative Surgical Plan Implant Selection Accuracy for INBONE II and Infinity TAA Groups. a
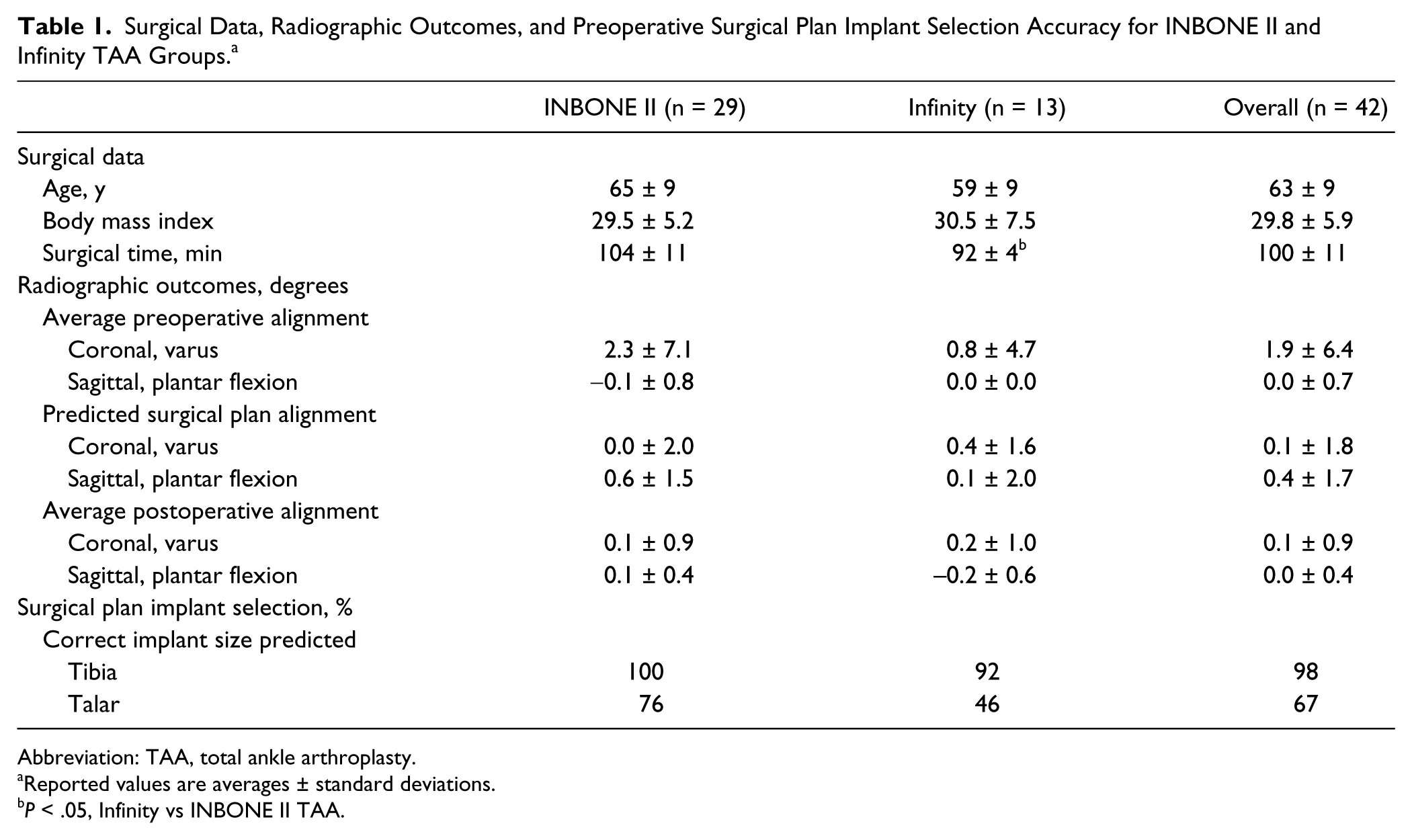
Abbreviation: TAA, total ankle arthroplasty.
Reported values are averages ± standard deviations.
P < .05, Infinity vs INBONE II TAA.
All coronal and sagittal alignment measurements followed previously published techniques.1,20 Coronal ankle alignment (varus/valgus) was determined on anteroposterior radiographs by measuring the angle between the vertical axes of the tibial shaft and talus before surgery and tibial stem and talar components after surgery. 20 Valgus alignment was defined as a negative angle on coronal images. Sagittal ankle alignment (flexion/extension) was evaluated on lateral radiographs by comparing the axes of the tibial shaft and a line perpendicular to the tibial intramedullary canal before surgery and tibial stem and talar components after surgery. 1 Dorsiflexion alignment was defined as a negative angle on sagittal images. The angle between the anatomic axis and the final implant axis was defined as the deviation between the planned and actual implant placements since each case was preoperatively aligned to the anatomic axis.
Coronal and sagittal alignments were measured and compared among weightbearing preoperative radiographs, preoperative CT scan–derived surgical plans, and postoperative weightbearing radiographs using a digital picture archiving and communication system (Stentor, Royal Philips Electronics, Amsterdam, Netherlands). All measurements were performed by a foot and ankle fellowship–trained orthopaedic surgeon with extensive experience performing radiographic analysis. Measurements were performed twice in separate sessions with a kappa coefficient of 0.92, indicating excellent intraobserver reliability. Data were found to be normally distributed using Kolmogorov-Smirnov tests, and differences between groups were evaluated using Student t tests and repeated-measures analysis of variance (SPSS, Chicago, IL). Differences in proportions between groups were evaluated with Fisher exact tests with significance set at P < .05.
Results
Average total surgical time was 100 ± 11 minutes for all TAA cases with significantly shorter operative times in the Infinity TAA group (92 ± 4 minutes) compared with the INBONE II group (104 ± 11 minutes; P < .05).
Average preoperative coronal alignment was 1.9 degrees varus ± 6.4 (range: 14 degrees valgus to 10 degrees varus), and average preoperative sagittal alignment was 0.0 degrees plantar flexion ± 0.7 (range, 2 degrees dorsiflexion to 3 degrees plantar flexion). There were 13 cases (31%) with neutral preoperative coronal alignment, 4 cases (9.5%) with less than 5 degrees varus, and 18 cases (43%) with 5 to 10 degrees of varus coronal deformity. There were 0 cases with less than 5 degrees valgus, 3 cases (7%) with 5 to 10 degrees valgus, and 4 cases (9.5%) with greater than 10 degrees valgus coronal deformity. Postoperative weightbearing alignments for all TAA cases were within ±3 degrees of the predicted coronal and sagittal alignments from the CT scan–derived surgical plans (Figures 1, 2). There were no significant differences in pre- or postoperative weightbearing alignments between INBONE II and Infinity TAA cases.
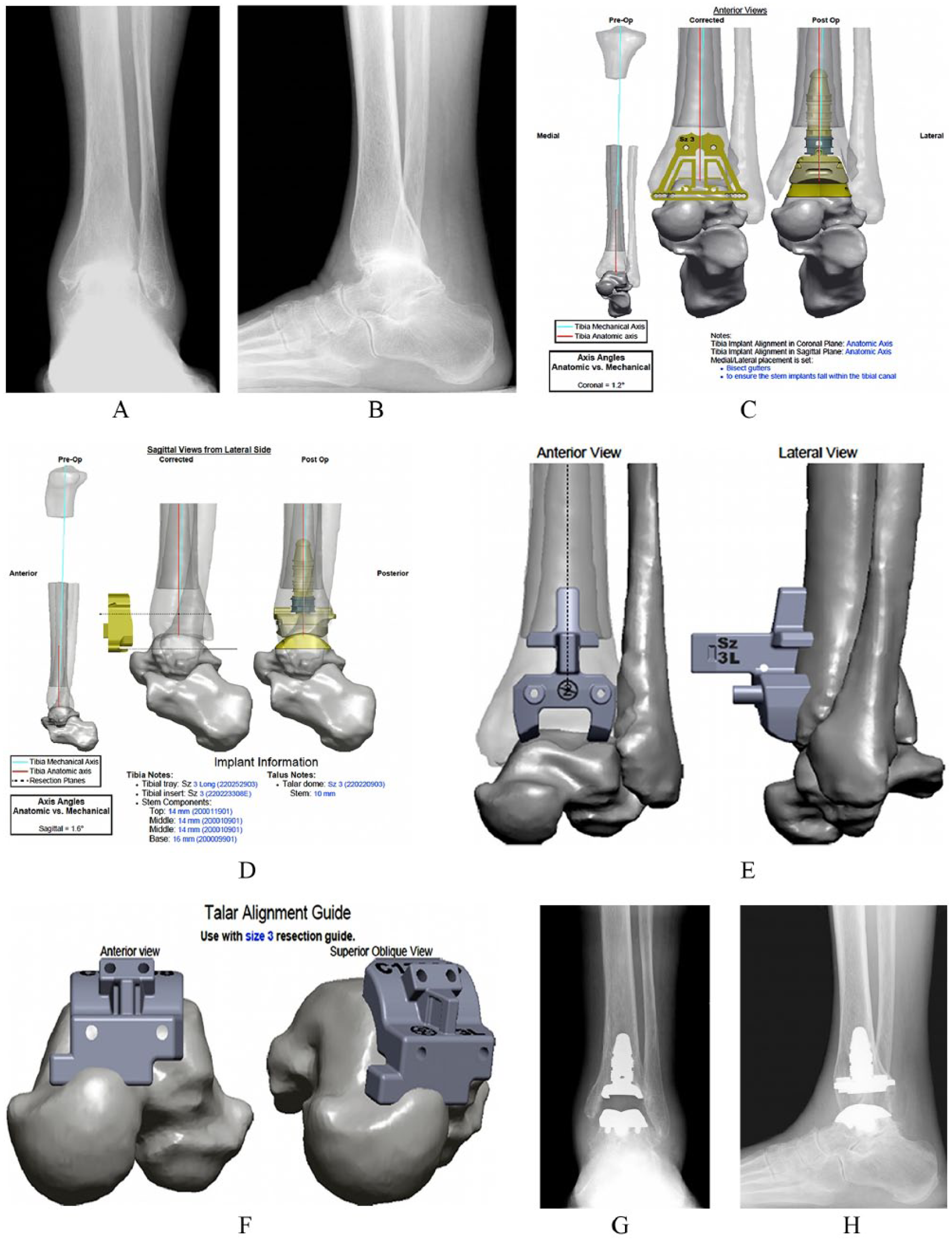
Preoperative weightbearing (A) anteroposterior and (B) lateral radiographs of a 69-year-old woman showing end-stage left ankle arthritis with 6 degrees of varus coronal deformity. (C) Anterior and (D) side views of planned distal tibia and talar bony cuts from preoperative computed tomography scan–derived patient-specific surgical plan. Patient-specific (E) distal tibia and (F) talar cutting guides showing planned guide placement on native bony anatomy. Weightbearing (G) anteroposterior and (H) lateral radiographs 3 months after intramedullary-referencing total ankle arthroplasty (INBONE II) demonstrating neutral coronal and sagittal alignment matching predicted computed tomography scan–based surgical plan and implant sizes.
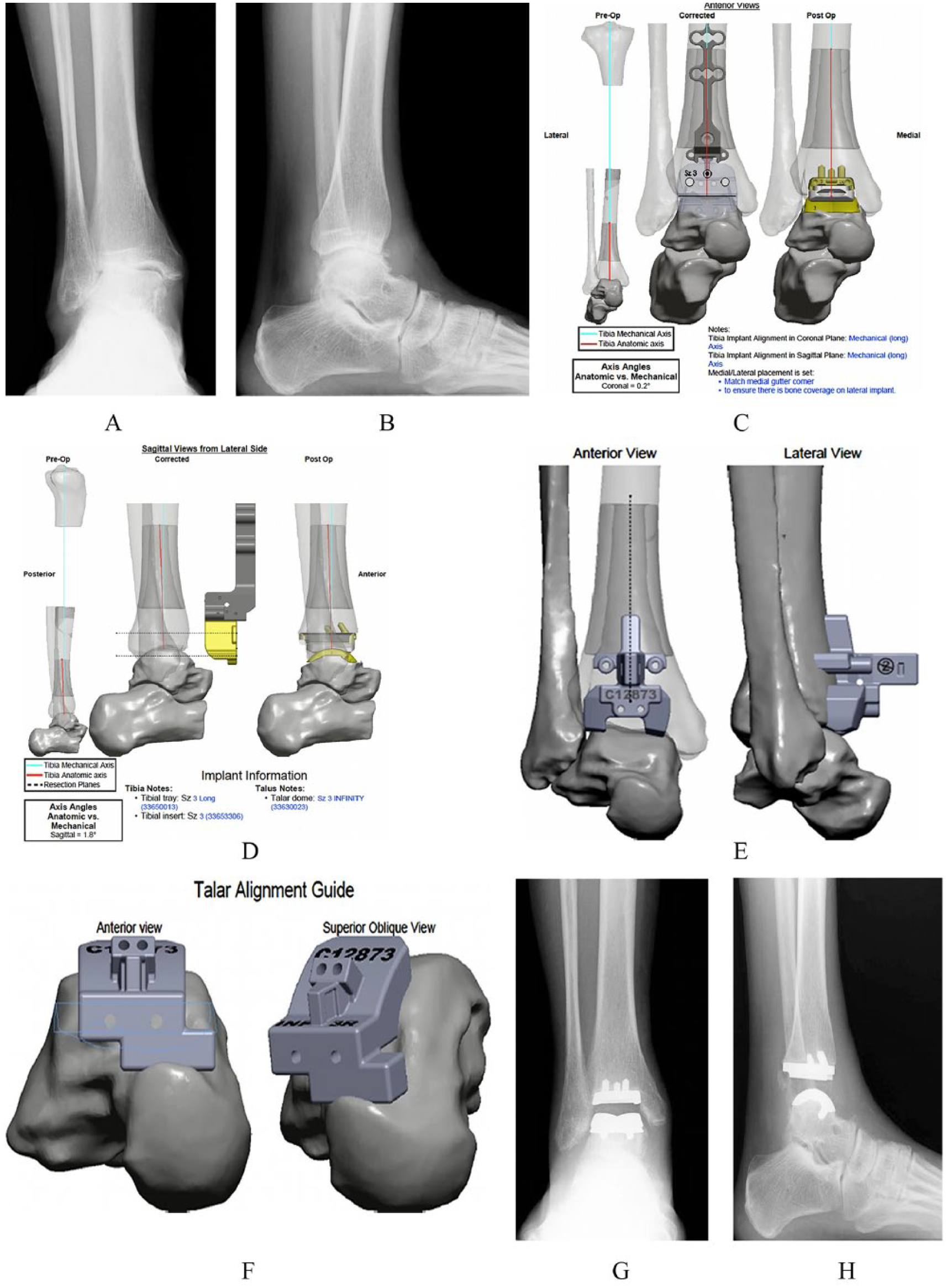
Preoperative weightbearing (A) anteroposterior and (B) lateral radiographs of a 52-year-old woman showing end-stage right ankle arthritis with 11 degrees of valgus coronal deformity. (C) Anterior and (D) lateral side views of planned distal tibia and talar resections. Patient-specific (E) distal tibia and (F) talar cutting guides showing planned guide placement. Weightbearing (G) anteroposterior and (H) lateral radiographs 3 months after low-profile tibia and talar resurfacing total ankle arthroplasty (Infinity) showing neutral coronal and sagittal alignment matching patient-specific surgical plan.
Neutral coronal (less than 1 degree varus/valgus) and sagittal (less than 1 degree plantar flexion/dorsiflexion) alignments were obtained for all TAA cases regardless of preoperative deformity. Average postoperative coronal alignment was 0.1 degrees varus ± 0.9, and average postoperative sagittal alignment was 0.0 degrees plantar flexion ± 0.4. Patient-specific surgical plans predicted all tibia and talar implants used within 1 size. Surgical plans predicted the actual tibia implant size used in 29 of 29 (100%) INBONE II cases and in 12 of 13 (92%) Infinity cases. Plans predicted the actual talar implant size used in 22 of 29 (76%) INBONE II cases and 6 of 13 (46%) Infinity cases. In all cases of predicted tibia or talar size mismatch, plans predicted 1 implant size larger than actually used.
Discussion
The main finding of this study was that preoperative CT scan–derived patient-specific plans and guides for TAA helped provide accurate and reproducible radiographic outcomes but were less accurate for talar implant sizing. Radiographic outcomes were within ±3 degrees of the predicted coronal and sagittal alignments from preoperative patient-specific surgical plans using 2 TAA implant systems. Neutral coronal and sagittal alignments were obtained for all cases regardless of the degree of preoperative deformity, and significantly shorter total operative times (12 minutes) were achieved when using patient-specific guides in combination with a low-profile tibia and talar resurfacing TAA (Infinity) compared to an intramedullary referencing TAA (INBONE II). This is the first study to report the early results of TAA patient-specific navigation in a clinical setting.
Obtaining reproducible anatomic alignment while correcting coronal plane deformity in TAA is critical to reduce the incidence of eccentric wear, component loosening, subsidence, and reoperation.12,14,15 In a systematic review of 49 studies evaluating TAA and ankle arthrodesis, Haddad et al found a 5-year TAA implant survival rate of 78% and a 10-year survival rate of 77%. 7 The overall revision rate for TAA was 7%, with the primary reason for revision being component loosening and/or subsidence (28%). Berlet et al reported on the use of patient-specific guides for TAA in a cadaveric model and found that surgical plans and guides provided reliable and reproducible placement of TAA implants. 3 Average variation between pre- and postoperative implant placement was less than 2 degrees and 1.4 mm in all specimens tested. Component placement was analyzed using multiple cameras to determine the position of infrared marker arrays on the distal tibia and talus, followed by software processing.
The present study expands on these findings and reports the early radiographic outcomes of patient-specific TAA in a clinical context. We found similar results in terms of implant alignment accuracy and reproducibility with an increase of 1 degree in coronal and sagittal plane variability. This is likely explained by the fact that implant alignment in the current study was determined using standardized measurements on a picture archiving and communication system with weightbearing radiographs rather than computer-guided measurements in more controllable cadaveric specimens. It is not standard policy for our institute to obtain postoperative CT scans after TAA due to increased radiation exposure and expense. However, postoperative CT scans would allow for improved analysis of TAA component rotation and axial alignment, both of which were not analyzed in the present study.
Patient-specific surgical plans predicted all tibia and talar implants used within 1 size, with a trend toward improved sizing accuracy with INBONE II TAA compared with Infinity TAA. In addition, there was an overall higher level of accuracy obtained for all tibia implants compared with talar implants (98% vs 67%). In all cases of predicted tibia or talar size mismatch, plans predicted 1 implant size larger than actually used. This can be partly explained by our preference to routinely downsize the talar component and increase medial and lateral gutter debridement when in between sizes to reduce the likelihood of gutter impingement that may cause postoperative pain.6,9,12 We have found gutter impingement to become symptomatic and to often require revision surgery when using larger talar sizes from older TAA systems. As a result, our current practice is to use a small reciprocating saw in combination with a medium rongeur to obtain at least 4 mm of space in the medial and lateral gutters.
It is important to note that there are multiple intraoperative checks that are available for the INBONE II and Infinity TAA systems that can and should be used by surgeons to guide final implant selection, in addition to the PROPHECY surgical plans. A unique design feature of both the INBONE II and Infinity TAA systems used in the present study was that there was a sulcus articulating geometry between the talar dome and polyethylene insert that increased coronal stability without overconstraining the ankle joint. 11 We have found that this additional stability without additional bony resection allows more aggressive medial and lateral gutter debridement that can improve ankle motion and limit residual ankle stiffness.
In analyzing the cases in the present study in which predicted implant sizes from surgical plans did not match actual sizes used, we did not find that the degree of deformity, presence of large cysts or osteophytes, retained hardware, body mass index, or other factors significantly affected implant sizing. Computer models were able to account for these factors and adjust the surgical plan for each patient’s native anatomy. However, future research is warranted to specifically evaluate the currently unknown factors that may influence implant sizing in large cohorts of TAA patients. In the present study, reproducible TAA alignments were obtained in all cases, performed by 5 foot and ankle fellowship–trained surgeons, thus increasing the generalizability of our findings. There were 22 cases (52%) with preoperative varus coronal deformity and 7 cases (17%) with valgus deformity that all achieved neutral alignment on weightbearing postoperative radiographs.
In our experience, we have found that patient-specific navigation is relatively easier and faster to use, in comparison with more traditional intramedullary and extramedullary guides. This idea is supported by the fact that total operative times were, on average, 12 minutes shorter when using navigation with Infinity TAA compared to INBONE II TAA. Infinity TAA can be performed entirely with patient-specific guides and cutting blocks, while INBONE II still requires a small external jig to guide tibial component insertion through the plantar heel. Cases of coronal or sagittal plane deformity greater than 5 degrees, significant distal tibia and/or talar bone loss, and revision TAA are well suited for CT scan–derived navigation to better define native anatomy, planned bony resection, and implant placement.5,8,12
Limitations of the present study were that it was retrospective and included a relatively small cohort of patients, thus limiting the statistical power of the study results. Average follow-up for all cases was 9 months with a wide range due to the recent application of patient-specific navigation to Infinity TAA in 2014. All patients were evaluated on standardized weightbearing radiographs at 3-month follow-up to evaluate final postoperative implant positioning. We did not evaluate clinical or functional outcomes given the radiographic focus of the present study. Long-term radiographic analysis of potential implant subsidence, osteolysis, and impingement was not conducted, but we are currently evaluating these factors in ongoing clinical studies.
Conclusion
Given our study results, we believe that CT scan–derived patient-specific TAA surgical plans and guides can be helpful in obtaining accurate and reproducible radiographic results in a clinical setting. It is important for surgeons to be aware that patient-specific surgical plans are able to predict implants used within 1 size, but accuracy is lower for talar implant sizing. Individual surgeon discretion should be used in combination with intraoperative checks when choosing final implants, as talar sizing can be significantly affected by the extent of gutter debridement. Our results may be applied to other TAA implant systems in the future and serve as the standard for the next generations of TAA. Further large-scale prospective clinical trials are warranted to evaluate TAA component positioning and alignment using patient-specific guides, the associated clinical effects in the short and long terms, and the cost-effectiveness of this technique.
Footnotes
Authors’ Notes
No part of this study has been submitted or duplicated elsewhere prior. This study has been read and approved by all authors and each author believes that the manuscript is valid and represents honest work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Robert B. Anderson, MD, W. Hodges Davis, MD, Bruce E. Cohen, MD, and Carroll P. Jones, MD, are paid consultants and receive royalties from Wright Medical Technology, Inc, the manufacturer of the PROPHECY preoperative computed tomography scan–derived patient-specific plans and guides discussed in the present study. Wright Medical Technology, Inc, is also the manufacturer of the INBONE II and Infinity total ankle replacement implants discussed in the present study. Andrew R. Hsu, MD, and J. Kent Ellington, MD, have no financial relationships with Wright Medical Technology, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.