
Abstract
Background:
We evaluated whether a history of prior infection about the native ankle joint, bone, or soft tissues was associated with a higher rate of infection following total ankle arthroplasty (TAA) when compared with that of primary TAA in the general population.
Methods:
This is a retrospective review of our institution’s TAA registry to identify all patients who reported a prior history of ankle joint sepsis or osteomyelitis and who were subsequently treated with TAA with at least 1-year follow-up. The primary outcome measure was re-infection rate. Secondary outcome measures were patient-reported outcome scores, implant survival, and complications. Twenty-two TAAs were performed in 22 patients, consisting of 9 men and 13 women, with a mean age of 58.4 years (range = 30-80 years). Patients were followed for a mean of 29.3 months (range = 11.4-83.8 months). The length of complete symptom-free interval between the index infection to time of TAA was 8.8 years (range = 0-44 years). These patients had a mean 2.7 (range = 0-13) procedures involving the ipsilateral ankle joint prior to TAA.
Results:
No deep infection was observed in this series. Eleven patients were followed for more than 2 years, with postoperative visual analog scale scores decreasing from 53.1 (range = 12-90) to 20.6 (range = 0-89) of 100. Ten of the 11 ankles also had AOFAS ankle-hindfoot and SF-36 scores. Their AOFAS ankle-hindfoot score increased from 38.9 (range = 10-61) to 70.1 (range = 29-90), and SF-36 score improved from 40.6 (range = 3.3-76.4) to 67.6 (range = 36.4-85.4).
Conclusion:
Single-stage TAA can be a viable option to treat arthritic ankle pain for those patients with resolved bone or ankle joint infection, producing improved outcomes in pain and function.
Level of Evidence:
Level IV, case series.
Introduction
End-stage ankle arthritis is a debilitating condition that has been traditionally treated with arthrodesis.1,12,24 Total ankle arthroplasty (TAA) is an effective alternative to arthrodesis for ankle arthritis in terms of pain relief, with the advantage of preserving adjacent joint function. Infection is an infrequent occurrence after TAA.1,6,11,12,27 However, when it occurs, periprosthetic infection can lead to devastating outcomes, including a source of implant failure, conversion to complex salvage arthrodesis, and limb loss.2,3,13,14,18,22 Among the risk factors for periprosthetic joint infection in other total joints is a history of prior joint infection, and as a result, prior ankle infection has often been considered an operative contraindication for TAA.4,7
In patients with prior, but resolved, native knee joint infections, total knee arthroplasty has proven successful in treating arthritic pain with variable subsequent reinfection rates.2,3,13,18,22 However, to our knowledge, no such reports exist in the total ankle literature, so the outcomes and reinfection rates in patients who undergo TAA after presumed eradication of prior ankle joint or bone sepsis remain unknown.
The objective of this study was to evaluate whether a history of prior infection about the native ankle joint, bone, or soft tissues was associated with a higher rate of infection following TAA when compared with that of primary TAA in the general population.
Methods
This study was approved by an institutional review board and informed-consent was obtained by all study participants prior to study enrollment. Using our TAA registry, we identified all patients who reported a prior history of ankle joint sepsis or periarticular osteomyelitis and who were subsequently treated with TAA (Figure 1) during the period from June 2007 to September 2014. All arthroplasties were performed by fellowship-trained orthopedic foot and ankle surgeons who were experienced in total ankle arthroplasty. The primary indication for TAA was painful end-stage ankle arthritis after failure of nonoperative treatment. All prostheses were implanted using the manufacturer’s described technique. Postoperative antibiotic prophylaxis was routinely administered for a 24-hour period in all patients after TAA.
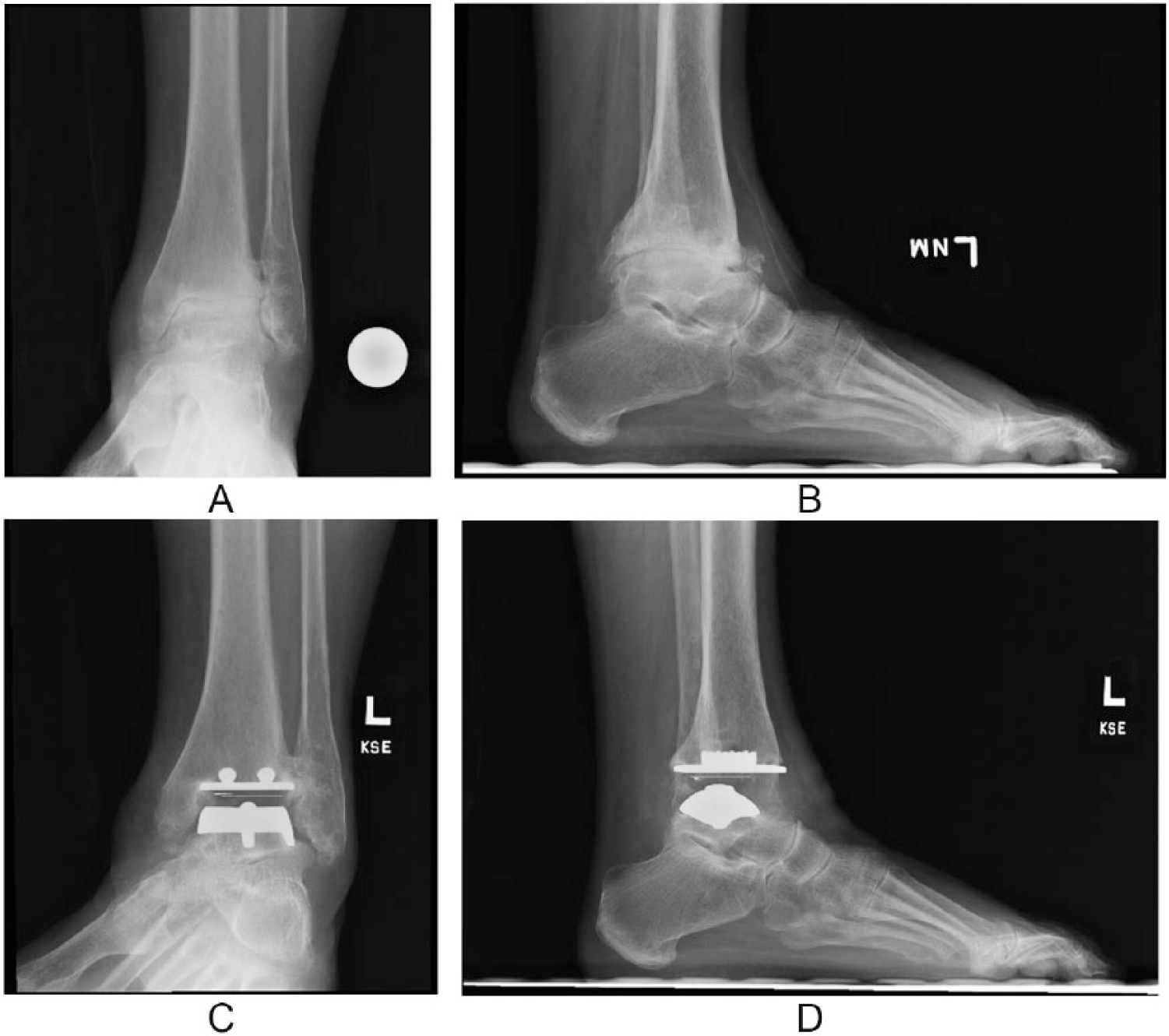
(A, B) A 65-year-old woman who had a history of left ankle fracture that required open reduction internal fixation that ultimately became infected with an open wound. She underwent wound debridement and hardware removal. Ten years later, she developed painful end-stage ankle arthritis. (C, D) Postoperative weightbearing radiographs at 22 months after total ankle arthroplasty.
All patients returned 3 weeks postoperatively for wound inspection and cast removal. Based on the condition of the soft tissue recovery, the operative extremity was again immobilized in a short leg cast for another 3 weeks of nonweightbearing or was placed into a controlled ankle movement (CAM) walker boot. Thereafter, patients participated in gradual range of motion exercises and progressive weightbearing until full weightbearing was achieved between 6 and 10 weeks postoperatively.
The etiology of the ankle arthritis, number of previous operative procedures, and medical comorbidities were recorded. Operative procedures performed concomitant with or subsequent to the TAA and postoperative complications were also reviewed. Implant failure was defined as any revision TAA or impending revision. We defined revision as the removal and reimplantation of either the tibial or the talar component and failure as conversion to tibiotalar or tibiotalocalcaneal arthrodesis.
A workup to detect the presence of quiescent infection was performed for each patient based on clinical suspicion of complete infection eradication. The preoperative workup may have included the use of laboratory testing such as white blood cell count, erythrocyte sedimentation rate, C-reactive protein, radiographs, and advanced imaging, including computed tomography or magnetic resonance imaging. The various combinations of testing and the decision to proceed with surgery were based on the discretion of the surgeon. The decision to perform routine preoperative ankle joint aspiration or obtain operative frozen section specimen or cultures was determined by clinical suspicion for active infection.
Pain and patient-reported function were assessed preoperatively, and postoperatively at 6 months, 12 months, and yearly thereafter. The 100-point visual analog scale (VAS) for pain (ranging from “no pain” to “worst pain imaginable”), the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, and the Short Form–36 (SF-36) Health Survey were used. Potential infection risk factors were reviewed including patient demographics such as age, gender, body mass index, smoking status, comorbidities, number of prior surgeries, and symptom-free interval after the index infection. The primary outcome measure was reinfection rate after TAA. Secondary outcome measures were patient-reported outcome scores, implant survival, and complications.
Twenty-two TAAs were performed in 22 patients, consisting of 9 men and 13 women, with a mean age of 58.0 years (range = 30-80 years) and mean body mass index of 28.4 (range = 21.6-35.9), who had a history of resolved native ankle joint or bone sepsis. All patients but 1 had a single-stage arthroplasty procedure. One patient had a 2-stage procedure, with the first surgery being irrigation and debridement. Potential host-related risk factors for infection included 9 previous smokers (40%), 1 current smoker (4.5%), 3 patients with diabetes mellitus (14%), and 1 patient with rheumatoid arthritis (4.5%). Source of index infection was diverse, with 15 infections secondary to trauma and subsequent reconstructive surgeries, 1 Lyme disease joint infection, hematogenous seeding of a native joint, and 2 unknown sources.
TAA from various manufacturers were implanted based on the surgeon’s preference at the time of surgery. They included 3 InBone I (Wright Medical Technology, Arlington, TN), 2 InBone II (Wright Medical Technology, Arlington, TN), 11 Salto-Talaris (Tornier, Bloomfield, MN), and 6 Scandinavian Total Ankle Replacement (Stryker, Kalamazoo, MI). Patients were followed clinically and radiographically for a mean of 29.3 months (range = 11.4-83.8 months).
Results
Of the 22 ankles with prior bone or ankle joint sepsis that were felt to be resolved, none were diagnosed with periprosthetic reinfection after primary TAA at the time of most recent follow-up. Four had intraoperative specimens taken for culture and microscopic examination. All final culture results were negative, with pathology showing no evidence of acute inflammation.
The length of complete symptom-free interval between the index infection to time of TAA was 8.8 years (range = 0-44 years). These patients had a mean 2.7 (range = 0-13) procedures involving the ipsilateral ankle joint prior to TAA.
The final postoperative patient-reported outcome scores demonstrated improvement from the preoperative baseline. Eleven ankles were followed for more than 2 years, with postoperative VAS scores decreasing from 53.1 (range = 12-90) to 20.6 (range = 0-89) of 100. Ten of the 11 patients had 2-year follow-up of AOFAS ankle-hindfoot and SF-36 scores. Their AOFAS ankle-hindfoot score increased from 38.9 (range = 10-61) to 70.1 (range = 29-90), and SF-36 score improved from 40.6 (range = 3.3-76.4) to 67.6 (range = 36.4-85.4).
Fifty percent (11/22) of patients also had at least 1 additional concomitant procedure. The most commonly performed concomitant procedure was tendo-achilles lengthening or gastrocnemius recession. No ankles had radiographic loosening or subsidence that required revision at the latest follow-up.
Early complications consisted of 3 patients who experienced delayed wound healing. One patient developed postoperative medial plantar nerve paresthesias that ultimately resolved by the time of final follow-up. Another patient sustained a nondisplaced medial malleolar fracture that was discovered after the patient began initial weightbearing and mobilization. The fracture was managed nonoperatively with cast immobilization for 3 months and ultimately healed.
Although no patient had deep reinfection that required revision surgery in our series, 14% (3/22) of patients did have subsequent nonrevision procedures. Two patients required subtalar arthrodesis for symptomatic hindfoot pain. One patient developed an enlarging periprosthetic cyst without component loosening that was treated with grafting.
Discussion
A critical component of success after any joint arthroplasty is the absence of postoperative periprosthetic infection. History of prior ankle joint sepsis or osteomyelitis has traditionally been considered a relative, if not absolute, contraindication to total joint arthroplasty. This study demonstrated that in patients who have resolution of an index infection and who later develop subsequent symptomatic end-stage ankle arthritis, TAA can be a viable option, with good success at early follow-up. To the authors’ knowledge, there are no previous published reports of the outcomes in this patient population.
TAA in patients with prior bone or ankle joint sepsis in this series showed no deep reinfections by the time of final follow-up. Patton et al had shown that prolonged wound drainage and dehiscence were a significant infection risk factor after TAA. Although 14% of our study group did experience postoperative delayed wound healing, none required additional wound-related surgeries. These results are similar to previously reported rates of 6.6% to 15% in the general population without a history of prior infection who underwent the same operation.9,10,15,26 Our findings suggest that prior septic history of the native ankle or bone that is determined to be resolved may not be an absolute contraindication to TAA. Postoperatively, these patients may also experience significant improvement in pain and subjective functional scores as expected in the general population without prior ankle or bone sepsis.1,11,20,21,26 The overall implant survival rate in this population was 100% at the latest follow-up. Previous literature reports total ankle implant survival rates of 70% to 98% at similar mean follow-up times.1,5,17,28
There was marked clinical improvement in patient-reported outcomes in this population. Functional improvement may be secondary to pain relief postoperatively.1,12,24 Both postoperative VAS pain and AOFAS ankle-hindfoot scores were better than preoperative baseline values. One patient did not experience pain relief after the TAA, with postoperative VAS pain scores of 89. At the last follow-up, she complained of continued pain secondary to a single medial malleolar screw and her resolving midfoot stress fracture.
Despite improvement in postoperative pain and functional scores, 14% (3/22) of the patients in this series required at least 1 nonrevision procedure involving the affected ankle and foot during the study period. This is also consistent with previously reported rates.1,12,23,26 These procedures were aimed to address the recognized preoperative pain triggers and were often scheduled as staged reconstruction of the foot and ankle. These procedures do not, however, indicate that the TAA procedure had failed.
Length of a symptom-free interval has been shown to correlate inversely with reinfection rates in patients with old native knee joint sepsis who underwent total knee arthroplasty. 16 This relationship, however, was not observed in our series of TAA. Seven patients with posttraumatic ankle arthrosis never were truly symptom free since the index traumatic event. They underwent TAA, often years later, for traumatic ankle arthrosis rather than infection. Instead of using a pain scale to evaluate the symptom-free interval, the authors in retrospect should have documented suspected infection-free interval, such as the number of years without wound dehiscence, drainage, and exposed hardware.
There are limitations to this study. The TAA procedures were performed by orthopedic foot and ankle specialists who have extensive combined experience. TAA complication rates tend to be lower in those who are no longer on the initial learning curve.8,19,25 The results of this study, therefore, may not be reflective of those of a novice surgeon. We experienced difficulty in determining clinical resolution of quiescent infection. Of the patients in this series, no patient had an obvious sinus tract or radiographic changes that were diagnostic of an active infection at the preoperative evaluation. Candidacy for surgery was determined by each surgeon independently based on his clinical experience, as there was no established protocol in either diagnostic or treatment strategy. Given the retrospective nature of this study, we did not have a control group and can only compare our series to published outcomes after TAA. Additionally, we did not routinely obtain preoperative inflammatory lab workup that could help confirm the eradication of prior infections, and old records did not always define the origin of prior infections and specific microorganisms, nor did we obtain intraoperative cultures in all cases. Although patients reported a clear history of prior infection, not all provided clear documentation of the organism isolated, antibiotic treatment, or number of procedures required to eradicate the infection. Intraoperative positive cultures that match the original infection organism would favor the theory that any reinfection is likely from prior bone or joint sepsis rather than a new organism. Given the individual patient’s presentation and clinical findings, the decision to obtain a culture was based on the surgeon’s intraoperative suspicion. However, none of the cultures that we did collect were positive. The third limitation was our small sample size because of the exclusivity of this patient population. We reviewed patient factors such as diabetes, obesity, smoking history, and clinical ASA grades, which might have predisposed any orthopedic patient to reinfection. None of these comorbidities correlated with deep reinfection. Although the mean follow-up of our study group was 29.3 months, there was still a slight possibility that a subclinical indolent infection existed in these patients.
Patients with prior infection about the ankle should be evaluated with high clinical acuity. It is the authors’ opinion to approach these patients first based on clinical history looking at the infection-free rather than pain-free interval. Next, we would focus on the quality of the soft tissue envelope that includes healing potential of the skin, mobility of the subcutaneous tissue, and defects of the fascia. When there is any suspicion of an infection, such as erythema or possible sinus tract, we would obtain laboratory values including C-reactive protein and erythrocyte sedimentation rate. With a high index of suspicion, we then would consider obtaining open or percutaneous bone biopsy for patients with previous osteomyelitis and aspiration for those with previous ankle joint sepsis. Quiescent infection may be difficult to rule out based on clinical or laboratory evaluation when used in isolation.
Conclusion
Single-stage TAA can be a viable option for patients with resolved bone or ankle joint infection, producing improved outcomes in pain and function. Early results in this small series are encouraging without recurrence of infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.