
Abstract
Background:
We aimed to compare the efficacy, postoperative pain scores, adverse effects, additional analgesic requirements, and patient satisfaction scores of ultrasonography-guided sciatic nerve block by popliteal approach with spinal anesthesia for hallux valgus correction surgery.
Methods:
Sixty patients scheduled for hallux valgus correction surgery were enrolled in this prospective randomized study. Unilateral spinal block was performed on patients in the spinal anesthesia group. Popliteal block group patients received popliteal sciatic nerve block with guidance by both nerve stimulator and ultrasonography. Durations of anesthetic and operative interventions and time until the initiation of surgery were recorded for both groups. Pain magnitude of the patients at the 2nd, 4th, 6th, 12th, and 24th hours following anesthetic interventions were assessed with a visual analog scale (VAS). Adverse effects such as postoperative urinary retention and postdural puncture headache were recorded. Also, patient satisfaction was recorded. Patients were interviewed by phone for anesthetic and operative complications at 72 hours postoperatively.
Results:
Spinal anesthesia group patients exhibited hypotension, bradycardia, postdural puncture headache, and urinary retention rates of 6.6%, 3.3%, 10%, and 3.3%, respectively. Popliteal block group patients showed none of these adverse effects. Moreover, VAS scores of the patients at the 2nd, 4th, 6th, and 12th hours were significantly lower (P < .001, P = .003, P < .001, P <.001, respectively), postoperative first analgesic requirement times were significantly longer (P < .001), and pain satisfaction scores were significantly higher (P < .001) in the popliteal block group.
Conclusion:
Given the complications related to spinal anesthesia and its insufficiency to maintain analgesia postoperatively, we believe the preferred anesthetic method should be peripheral nerve blocks for hallux valgus correction surgeries.
Level of Evidence:
Level I, randomized prospective study.
Introduction
Hallux valgus is the most frequent foot deformity, with rates up to 23% in the population between ages 18 to 65 and 35% in those older than 65 years, 9 affecting females more frequently in comparison to males and surgical correction is a common operation. 1 Anesthetic methods including general anesthesia, local anesthesia, peripheral nerve blocks, epidural anesthesia, and spinal anesthesia are used. However, spinal anesthesia is the preferred method for lower extremity surgery in some clinics because of the reduced risk of thromboembolic, cardiovascular, and pulmonary complications.6,10 With increasing use of ultrasonography for guidance of peripheral nerve blocks, they have become a popular method of anesthesia in hallux valgus operations.
Although ultrasonography-guided peripheral nerve blocks performed in preoperative preparation rooms reduces the time between admission to the operating room and the initiation of the surgical procedure, longer duration in comparison with spinal anesthesia and requirement of experience limit its widespread use. 5 Besides this disadvantage, use of peripheral nerve blocks still hold many advantages such as providing longer-term analgesia, reduction of analgesic requirements and higher patient satisfaction. The goal of our study was to compare postoperative pain scores, adverse effects, use of analgesics, and patient satisfaction scores of patients who received either popliteal sciatic nerve block or spinal anesthesia for hallux valgus correction surgery.
Methods
This study was performed after obtaining a local ethics committee approval. Sixty patients between 18 and 60 years old who had an American Society of Anesthesiologists (ASA) physical status score of 1 or 2 were enrolled in this prospective randomized study. Written and signed consents were obtained from all participants. Patients who had infection at the intended injection site for spinal anesthesia, had bleeding diathesis, were receiving anticoagulant medications, or who refused spinal or peripheral nerve blocks were excluded. Thirty patients received unilateral spinal anesthesia, and another 30 patients received sciatic nerve block via popliteal approach and saphenous nerve block to prevent tourniquet pain. Anesthetic intervention durations, surgery initiation times, anesthetic efficacies, and adverse effects between groups were compared. Patient demographics were similar between groups (Table 1).
Demographics and Clinical Data.
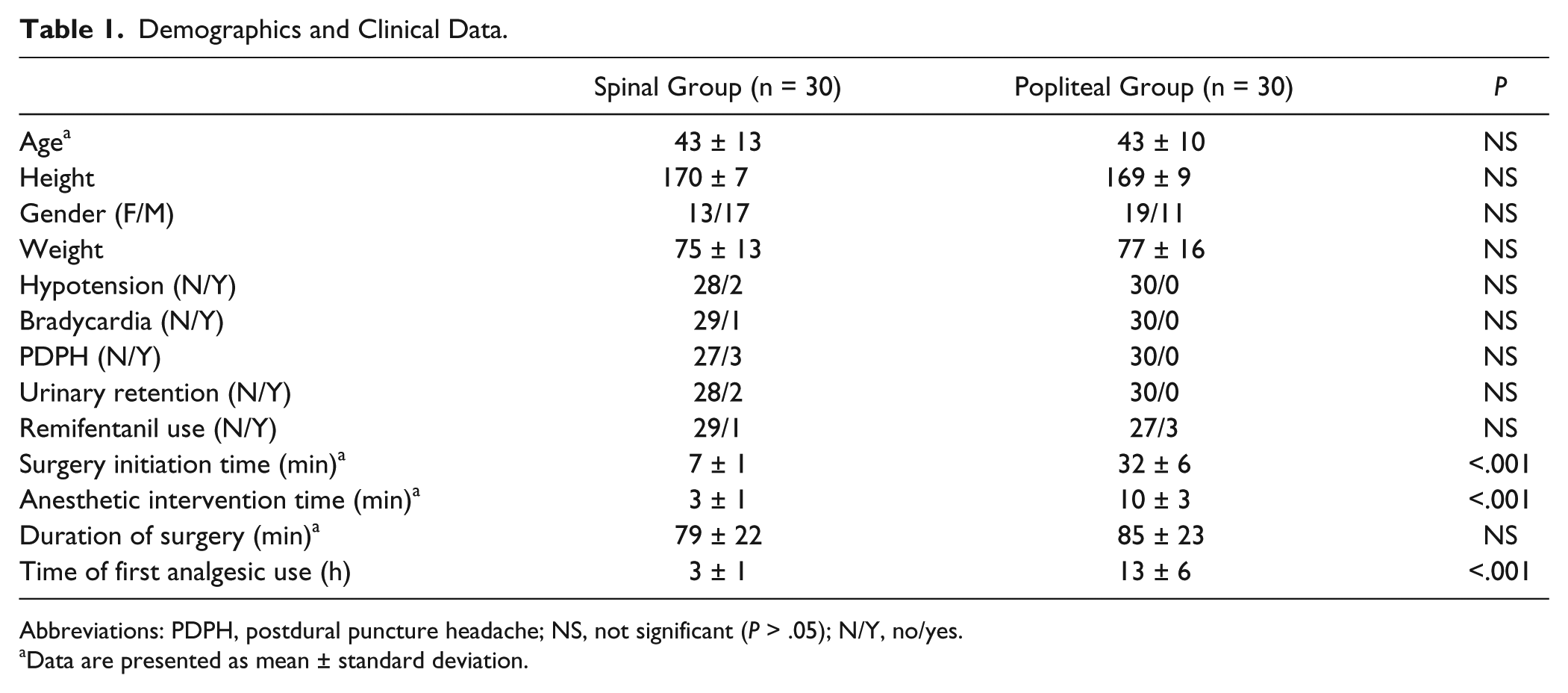
Abbreviations: PDPH, postdural puncture headache; NS, not significant (P > .05); N/Y, no/yes.
Data are presented as mean ± standard deviation.
Patients’ blood pressures, heart rates, and peripheral oxygen saturations were measured and recorded following a 5-minute rest in the supine position before anesthesia. Patients in both groups were sedated with 0.03 mg/kg midazolam via intravenous line. Patients in the spinal anesthesia group (n = 30) had 2.5 mL of 0.5% hyperbaric bupivacaine injected with a slow injection rate.
Popliteal block group patients (n = 30) received sciatic nerve block via a popliteal approach with ultrasonography guidance and confirmation with a nerve stimulator. The procedure was performed with 18-G 100 mm peripheral block needle (Contiplex S Ultra, Braun, Melsungen, Germany) by in-plane technique after visualization of the sciatic nerve 5 to 10 cm proximal to the popliteal fossa. A linear ultrasonography probe with 7.5 to 12 MHz frequency was used for imaging. After adequate placement of the needle was confirmed with motor response to stimulation at 0.5 mA current, 20 mL (12 mL for tibial nerve and 8 mL for common peroneal nerve) of 0.5% bupivacaine (containing 5 μg/mL ephedrine) was administered. Saphenous nerve block was performed to provide adequate analgesia for pain emerging from pressure of the calf tourniquet. Nerve block was performed as infiltration anesthesia. Ten milliliters of 1% prilocaine was administered between the tibial tuberosity and medial head of the gastrocnemius subcutaneously.
A 3-cm longitudinal incision was made along the medial aspect of the first metatarsal. A capsulotomy was performed, and medial eminence was excised. A second incision was performed laterally and the adductor hallucis tendon and lateral capsule was loosened. The site of osteotomy was approached via a third medial incision. An osteotomy with an appropriate angle to correct the metatarsus primus varus was performed, and then the osteotomy was fixed with Kirschner wires.
Hemodynamic parameters of patients in both groups were measured and recorded in 5-minute intervals. Patients suffering from procedural pain were administered an infusion of remifentanyl (from 0.05 to 0.2 μg/kg/min dose to avoid respiratory depression) for sedation and analgesia. Durations of anesthetic and operative interventions and time until the initiation of surgery were observed and recorded. Intraoperative bradycardia (patients with heart rate <50 bpm were administered 0.5 mg atropine) and hypotension (patients with mean arterial pressure lower than 50 mmHg were administered 5 mg of ephedrine) were recorded when present. Patients were followed for approximately 1 hour in the postanesthesia care unit and then transferred to the orthopedics ward.
Seventy-five milligrams of diclofenac sodium was administered to every patient once every 12 hours via the intramuscular route postoperatively. Tramadol HCl at a dose of 1 mg/kg was administered intramuscularly to overcome additional analgesic requirements. Visual analogue scale (VAS) pain scores for both groups after anesthetic intervention at the 2nd, 4th, 6th, 12th, and 24th hour was assessed. Adverse effects such as postoperative urinary retention, urinary catheterization, and postdural puncture headache were recorded. Patients with postdural puncture headache were treated with acetaminophen tablets containing caffeine once every 6 hours and adequate hydration. All of the patients were treated successfully and epidural blood patch treatment was not necessary for any of the patients. Splints were used until swelling was resolved and wound recovery started. Patients were examined for foot drop once every 24 hours. Range of motion exercises and partial weigthbearing exercises were initiated. Full weightbearing was initiated after a solid union of the osteotomy was achieved. Patients without headache and surgical complications at the end of the third day were discharged. Patients were phoned and questioned about the anesthetic procedure and its complications (sensory and motor deficit) and patients’ satisfaction scores.
A power analysis was performed with an assumption of a 30% decrease in the 2nd-hour VAS score in the popliteal group, and the required sample size was calculated as 32 patients for each group to detect an existing difference between groups.
Statistical analyses were performed with Statistical Package for Social Sciences version 18 (SPSS Inc, Chicago, IL). Numerical data fitting normal distribution were expressed as mean ± SD, and numerical data not fitting normal distribution were expressed as median (minimum-maximum). Categorical data were expressed as percentage. Difference between mean or median values of the numerical data was assessed with Student t test or Mann-Whitney U test according to distribution of the data. Significance between categorical data was assessed either with Mann-Whitney U test or chi-squared test. P values lower than .05 were interpreted as significant.
Results
Anesthetic intervention durations and surgery initiation times were significantly shorter in the spinal anesthesia group (P < .001). Spinal anesthesia group patients exhibited hypotension, bradycardia, postdural puncture headache, and urinary retention rates of 6.6%, 3.3%, 10%, and 3.3%, respectively. However, popliteal group patients showed none of these adverse effects. Although intraoperative narcotic analgesic requirements were similar, analgesic requirements of the spinal anesthesia group patients emerged significantly earlier in comparison to popliteal block group patients (P < .001) (Table 1). Moreover, VAS scores of the patients at the 2nd, 4th, 6th, and 12th hours were significantly lower in popliteal block patients (P < .001, P = .003, P < .001, P < .001, respectively). Pain scores at the 24th hour were similar between groups (Table 2). Patient satisfaction was found to be significantly higher in the popliteal group (P = .022). Fifty percent of the patients in the popliteal block group were very satisfied with the procedure, and 20% of the patients were very satisfied with the procedure in spinal block group (Table 3). None of the patients had numbness or nerve pain in the first 72 hours.
Superficial Pain Scores. a
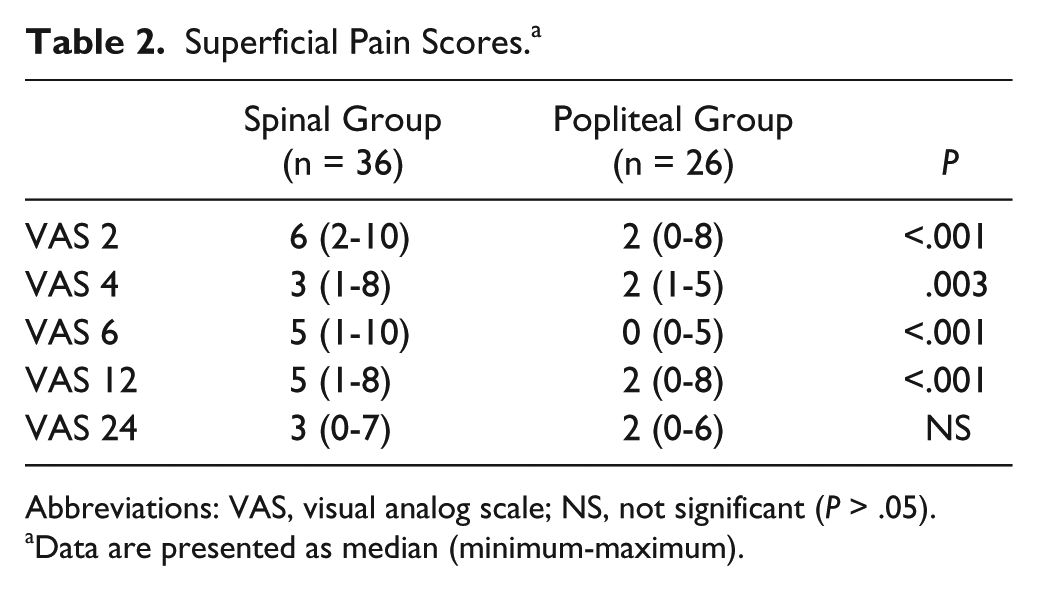
Abbreviations: VAS, visual analog scale; NS, not significant (P > .05).
Data are presented as median (minimum-maximum).
Patient Satisfaction Ratings (P = .022). a
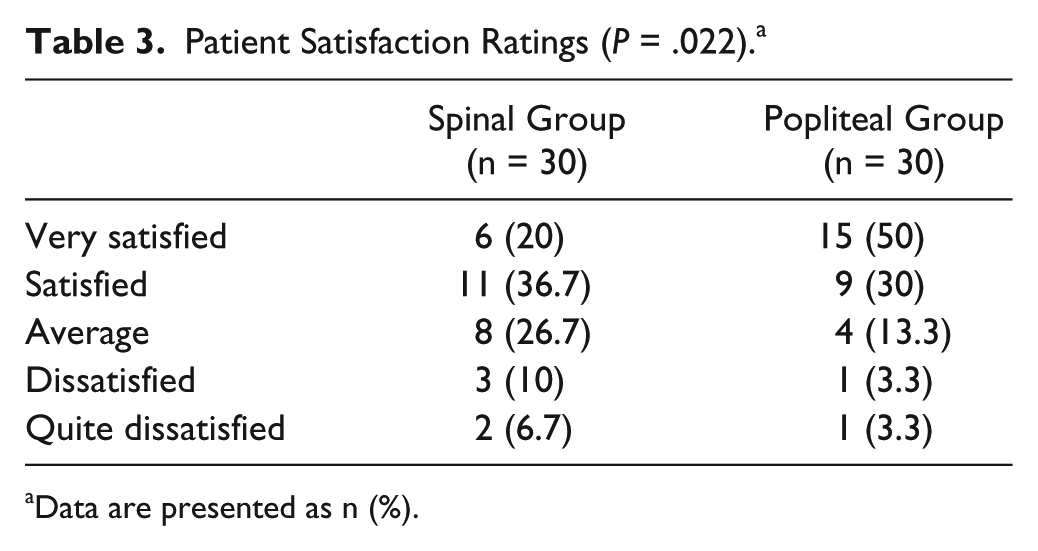
Data are presented as n (%).
Discussion
Peripheral popliteal nerve block is a good alternative to spinal anesthesia for hallux valgus surgery because of lower complication rates, better postoperative pain management, and reducing the time between admission to the operating room and the initiation of the surgical procedure. Foot surgery often causes serious and prolonged postoperative pain. In our study, we concluded that peripheral nerve blocks provided a longer and more effective analgesia compared to spinal anesthesia. We assessed VAS scores of the patients in both groups and observed significantly higher pain scores in the spinal anesthesia group at the 2nd, 4th, 6th, and 12th hours. We found that the time to first analgesic use in the popliteal block group was significantly longer compared with the spinal group (12.6 ± 6.2 vs 2.5 ± 1, respectively, P < .001). This may be explained by the perineurium of the peripheral nerve playing the role of a neutral barrier for local anesthetics and slow absorption of a large amount of local anesthetic surrounding the nerve from peripheral tissue, 11 as well as with a longer onset of action of the peripheral nerve block compared with spinal anesthesia.
Patients can require high doses of parenteral opioid use following hallux valgus surgery. Opioid drugs cause many adverse effects, including nausea, vomiting, hypotension, hypertension, constipation, pruritus, drowsiness, and respiratory depression. These adverse effects can limit the use of opioid drugs on orthopedic wards where advanced monitoring devices are not feasible. This limitation causes poor pain control, which should be considered when choosing an anesthetic technique. Implementation of peripheral nerve blocks provides long-term analgesic effects and avoids such adverse effects. Popliteal block provides excellent postoperative pain control for foot surgery. 8 In our study, patients in the spinal anesthesia group showed higher analgesic requirements. Thus, we concluded that performing popliteal sciatic nerve block could avoid the adverse effects of analgesics, opioids in particular. Also, performing peripheral nerve blocks may reduce adverse effects such as nausea, vomiting, hypotension, and bradycardia related with central blocks. Although none of the patients in the popliteal block group demonstrated adverse effects, 3 patients in the spinal anesthesia group had nausea and vomiting, 5 patients had hypotension, and 5 patients had bradycardia. Observed adverse effects were treated with adequate fluid management and sympathomimetic agent administration. In our study, the patient population between 20 and 60 years old and ASA physical status score of I-II was considered to be a facilitator for treatment response. However, considering late physiological responses and unstable hemodynamic balance of the more elderly patient population, considering peripheral nerve blocks as a method of choice might be crucial in maintaining hemodynamic stability. 2
Another important factor for the choice of anesthetic technique is patient consent and patient satisfaction. Popliteal sciatic nerve block provides effective analgesia and high patient satisfaction following foot surgery. 7 Our study also showed more effective analgesia and higher patient satisfaction scores in patients who underwent surgery with popliteal sciatic block compared with those who underwent surgery with spinal anesthesia.
We found anesthetic intervention durations (popliteal: 10 ± 3 vs spinal: 3 ± 1, P < .001) and surgery initiation times (popliteal: 32 minutes ± 6 vs spinal: 7 ± 1, P < .001) to be significantly longer in the popliteal block group. Longer intervention durations with a popliteal block may constitute a serious disadvantage, but this is easily resolved by the block being performed in the preoperative preparation room. As transport following spinal anesthesia may carry risks concerning patient safety, anesthesiologists would rather have this procedure performed in the operating room to minimize the risk of falling. Therefore, surgery was initiated later in patients with spinal anesthesia compared to patients with popliteal sciatic nerve block. These features probably ensure a better and more effective use of the operating room in patients who undergo surgery with popliteal sciatic nerve block.
Besides all these advantages of peripheral nerve blocks, there are also limitations related to their use. These limitations include direct nerve injury, local hematoma, and subsequent ischemic injury, infection, inefficient block, and systemic toxicity following vascular injection. The most common complication related to popliteal nerve block is prolonged numbness or nerve pain during the postoperative period. We did not observe any of these complications for 72 hours following the anesthetic procedure. One recent study suggests nerve injury related to popliteal nerve block becomes apparent in the early postoperative period, whereas earlier studies show that a 72-hour follow-up may not be sufficient time to detect and diagnose all complications related to peripheral nerve blocks.3,4,12 This creates a limitation for our study and accentuates the necessity for long-term studies assessing chronic pain and neurologic complications.
In conclusion, popliteal sciatic nerve block served as a good alternative to spinal anesthesia for hallux valgus correction surgery. Lower complication rates, better postoperative analgesia, and better patient comfort made popliteal block a better choice for hallux valgus operations in comparison to spinal anesthesia. An apparent disadvantage of popliteal block was longer intervention durations, which could easily be resolved by performing the intervention in the patient premedication room.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.