
Abstract
Background:
Up to 60% of patients with an osteoarthritic ankle joint develop talar tilt with progression of the osteoarthritic process. The configuration of the subtalar joint, in particular the posterior facet, may contribute to the development of this wear pattern. Recently, the subtalar vertical angle (SVA) was used to describe the posterior facet of the subtalar joint in the frontal plane. The aim of this work was to analyze if the orientation of the subtalar joint may influence the type of asymmetric ankle osteoarthritis.
Methods:
In total, 60 ankles were retrospectively analyzed including 40 osteoarthritic patients and 20 healthy controls. The osteoarthritic ankles were divided into 4 groups: varus ankle joints with (incongruent) or without (congruent) a tilted talus and valgus ankle joints with (incongruent) or without (congruent) a tilted talus. The orientation of the subtalar joint was described using the SVA. The SVA was determined for every patient using weightbearing CT scans. Additionally, the inter- and intraobserver reliability was assessed using intraclass correlation coefficients (ICCs).
Results:
The inter- and intraobserver reliability was excellent (ICC > 0.989 and >0.975, respectively). The varus groups (incongruent and congruent) had significantly lower SVA values, that is, more varus orientation of the subtalar joint than the valgus groups (P < .05). The SVA of the control group was between the values of the varus and valgus ankles.
Conclusion:
The SVA provided a reliable and consistent method to assess the varus/valgus configuration of the posterior facet of the subtalar joint. In our cohort, varus osteoarthritis of the ankle joint occurred with varus orientation of the subtalar joint whereas in patients with valgus osteoarthritis, valgus orientation of the subtalar joint was found. Our data suggest that the subtalar joint orientation may be a risk factor for the development of ankle joint osteoarthritis.
Level of Evidence:
Level III, retrospective case control study.
Introduction
A majority of the patients with ankle osteoarthritis present with an asymmetric wear pattern (eg, varus or valgus type). 19 Furthermore, up to 60% of the patients suffering from an osteoarthritic ankle joint develop talar tilt with progression of the osteoarthritic process.4,6,11,19 Reasons for this are thought to be deformities of the lower leg and knee joint, ligamentous laxity, tendon dysfunction and neurologic disorders.2,8,9,12,15,17,18 Recently, however, it has been proposed that the adjacent joints and, particularly, the subtalar joint may have a major influence on this process.3-5,14 Hayashi et al described in 2008 the configuration of the posterior facet of the subtalar joint using plain radiographs in a cohort of 80 patients (133 ankles) with primary varus osteoarthritis of the ankle. 4 A more pronounced valgus inclination of the subtalar joint was recognized until the intermediate stage of ankle osteoarthritis. Consequently, a compensatory mechanism of the subtalar joint was discussed. However, it is rather difficult to evaluate the orientation of the subtalar joint using conventional radiographs; CT scans would be more appropriate.
To distinguish between varus/valgus configuration of the subtalar joint, Van Bergeyk et al introduced in 2002 the subtalar vertical angle (SVA) using nonweightbearing CT scans. 20 Today, weightbearing CT scans can be performed, leading to a better understanding of the functional anatomy of the hindfoot. Recently, Colin et al described the morphology of the subtalar joint in a healthy cohort using weightbearing CT scans. 3 In this article, the subtalar joint orientation in the frontal plane was determined using the SVA.
However, the frontal plane orientation of the subtalar joint in patients with asymmetric ankle joint osteoarthritis has not been examined. Furthermore, the reliability of the SVA is unknown. Using weightbearing CT scans, we assessed the reproducibility of the SVA and analyzed the orientation of the subtalar joint in patients with asymmetric ankle osteoarthritis. We hypothesized that the SVA would provide reliable and reproducible measurements in varus ankles presenting with a varus subtalar joint and valgus ankles with a valgus orientation of the subtalar joint, respectively.
Methods
Data Source and Study Population
The local Ethics Committee approved the protocol and the study was done according to the Declaration of Helsinki and the Guidelines for Good Clinical Practice. Included were patients with asymmetric osteoarthritis of the ankle. Exclusion criteria were unmanageable joint instability or neurovascular disease. Furthermore, patients with an arthrodesis of the hind- or midfoot or talocalcaneal coalition were also excluded. Four groups were defined according to the type of ankle osteoarthritis: varus and valgus ankles were further divided into ankles with a tilted talus (incongruent) and ankles without a tilted talus (congruent). 10 Each group contained 10 patients (total 25 male, 15 female, mean age 60, range 25-85 years). Additionally, a group of 20 volunteers without hindfoot pathology were included as controls (10 male, 10 female, mean age 47, range 16-63 years).
Imaging and Measurement Methods
Asymmetric osteoarthritis was diagnosed on a plain, weightbearing anteroposterior (AP) and lateral radiograph of the ankle. The angle between the tibial shaft and the surface of the talar dome (TTS) was measured on the AP radiograph (Figure 1). 4 Valgus deformity was defined as a TTS of more than 94.2 degrees and varus as a TTS of less than 83.8 degrees. 14 Additionally, the tibial articular surface angle (TAS, normal values 91 to 93 degrees) was measured on the medial side of the AP radiograph. 7 By calculating the difference between the TAS and the TTS, the congruency of the tibiotalar joint was determined. 10 A difference of less than 4 degrees was defined as a congruent joint and a difference of more than 4 degrees as an incongruent joint. 10 For the determination of the TAS and TTS, all radiographs were imported into an image processing software (Image ims Client, Version 12.23.019, Glattbrugg, Switzerland), where the angles were measured digitally.
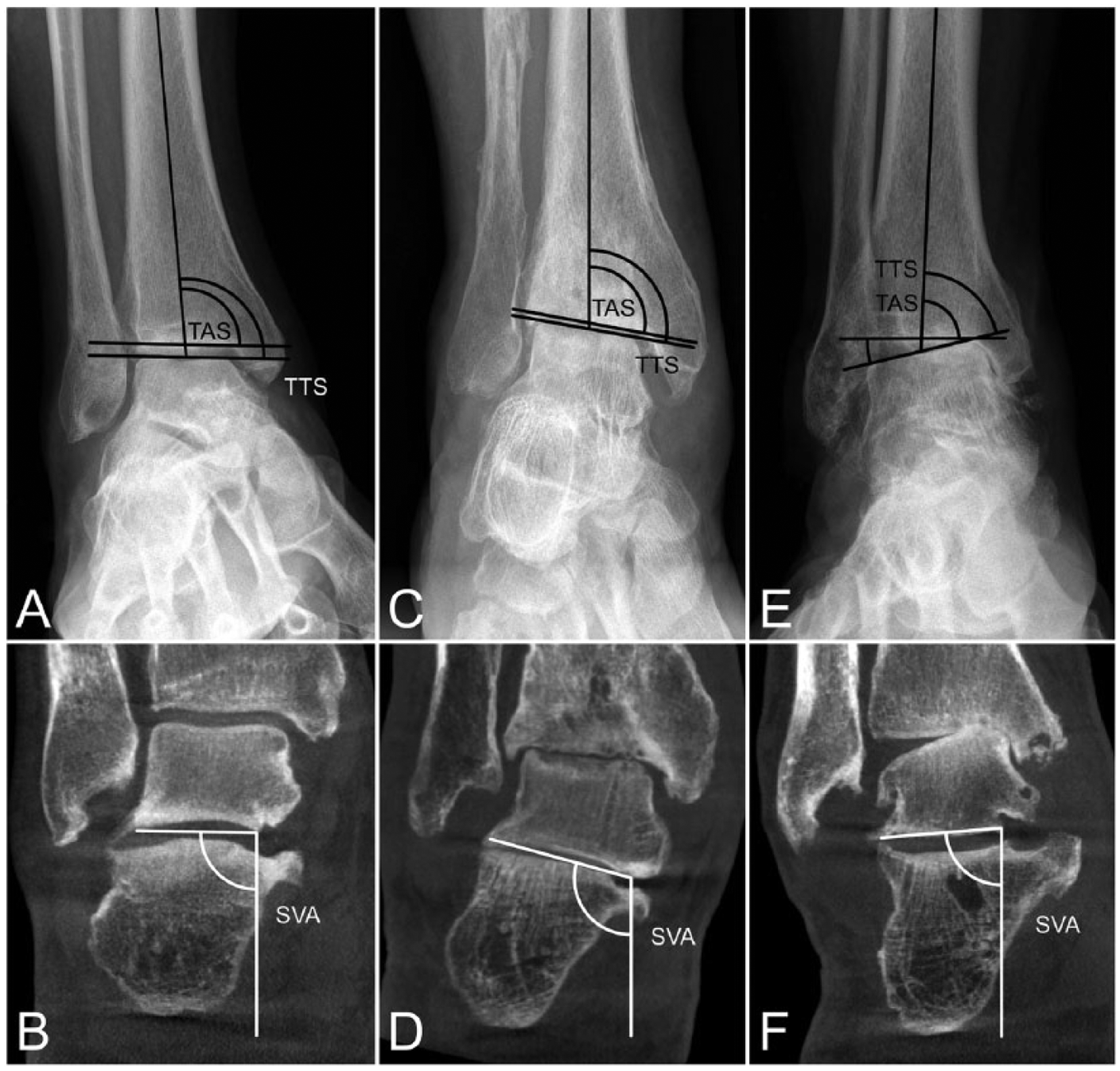
Plain radiographs were used to distinguish between the different ankle deformities. Using the tibiotalar angle (TTS) and the angle of the tibiotalar joint surface (TAS), patients were divided into 4 groups. The subtalar vertical angle (SVA) was determined using coronal weightbearing CT scans. (A, B) Example of a healthy volunteer. (C, D) Example of a congruent osteoarthritic valgus ankle. (E, F) Example of an incongruent osteoarthritic varus ankle.
The SVA was measured using weightbearing CT scans according to Van Bergeyk et al (Figure 1).3,20 The CT scan was done with a standardized setting at our radiology department. The longitudinal axis of the lower leg was placed perpendicular to the ground. The CT scan was started 10cm proximal to the tibiotalar joint and terminated at the sole of the foot with the subjects standing upright and fully weightbearing on 1 foot (Planmed Verity®, Planmed Oy©, Helsinki, Finland; 0.2mm slice thickness, 1mm slice interval). A sagittal plane was set parallel to the projection of a line connecting the center of the heel and the base of the second metatarsal (Figure 2). A cut through the middle of the subtalar joint on the sagittal plane was defined as the middle coronal plane used to measure the SVA (Figure 2). According to the method of Colin et al, an additional anterior coronal plane was defined as 5 mm anterior to the middle coronal plane and an additional posterior coronal plane as 5 mm posterior to the middle coronal plane. 3 The measurements in these different coronal planes were used to account for possible changes of the orientation of the posterior facet in the frontal plane because of the screw-shaped anatomy of the subtalar joint. 7 SVA values lower than 90 degrees were defined as varus and values more than 90 degrees as valgus configuration. In respect to a possible subluxation of the subtalar joint in osteoarthritic varus or valgus ankles, which may have had an effect on the SVA, different axes in the axial plane were used for the reconstruction. Using the center of the heel as a pivotal point, the principal axis (conjunction between the center of the heel to the base of the second metatarsal) was rotated 5, 10, and 20 degrees laterally and medially to ensure the consistency of the SVA (Figure 2).
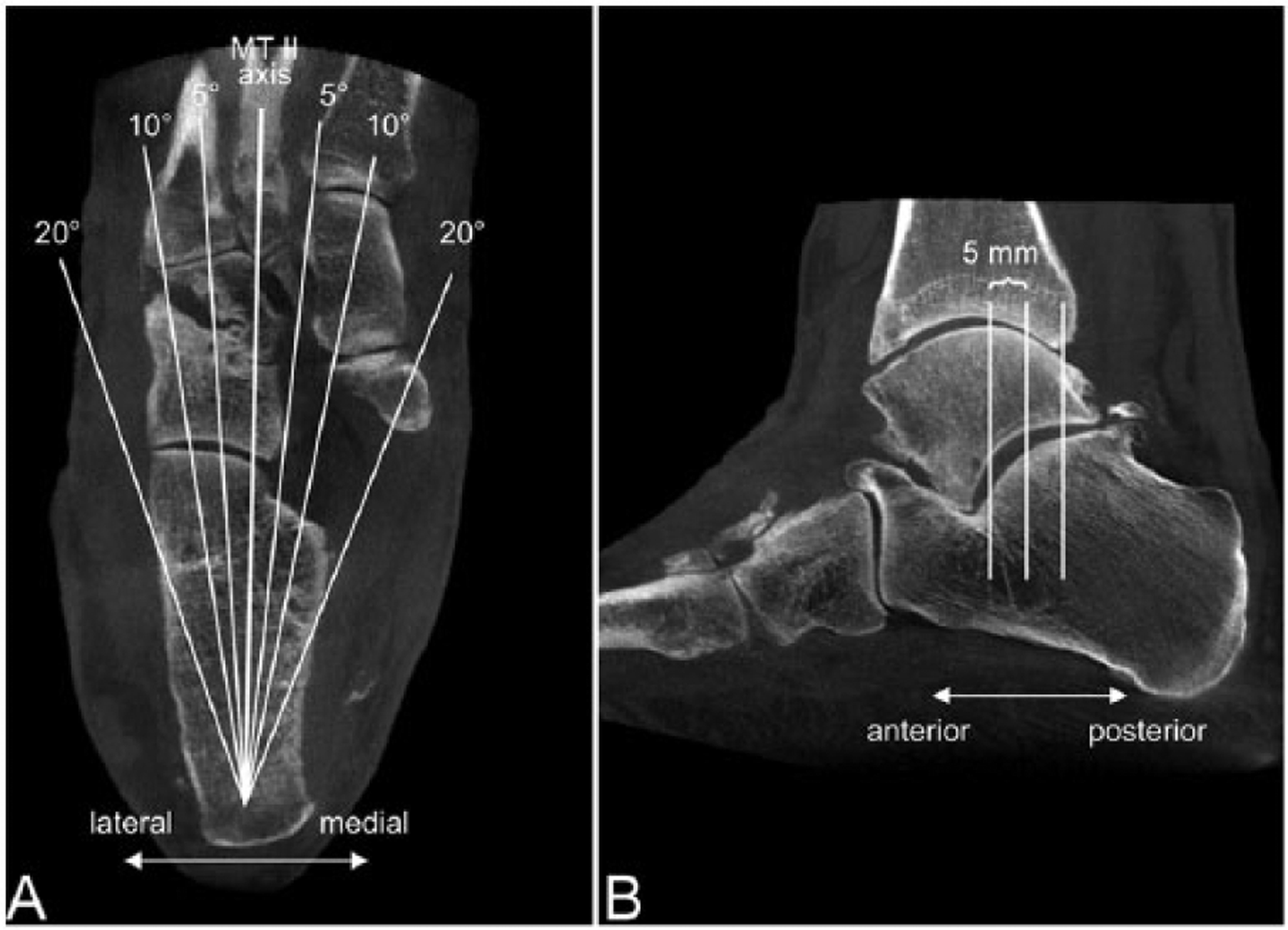
Lateral and medial deviation from the principal axis on the axial plane was done to ensure the consistency of the subtalar vertical angle (SVA, A). Furthermore, the sagittal plane was used to distinguish between an anterior, middle and posterior plane of the posterior facet of the subtalar joint (B).
Images were saved as Digital Imaging and Communications in Medicine (DICOM) files. A 3D Multi-Planar Reconstruction (3D-MPR) was performed using an image processing software (OsiriX MD®, Pixmeo©, Geneva, Switzerland). Three independent investigators (1 orthopaedic resident, NK; 1 medical student, MT; and 1 scientific associate, LB) measured the SVA in 120 images (40 patients) in a randomized order. One investigator (MT) randomly assessed the measurements 3 times at an interval of 2 weeks in order to determine the intraobserver reliability. Measurements used for the assessment of the reliability were done on osteoarthritic ankles using the principal axis in the axial plane for reconstruction.
Statistical Methods
All measurements are expressed as mean ± standard deviation (SD). A Shapiro-Wilk test was performed to verify whether data were normally distributed for continuous variables. The sample size for determination of the reliability of the SVA was based on studies by Walter et al. 21 Minimum intraclass coefficient (ICC) was set at 0.8, and the desired ICC at 0.9. With 3 measurement replicates and a significance level of 0.05 with a power of 80%, a minimum of 33 samples were required. For the inter- and intraobserver reliability of the SVA, the 2-way random intraclass correlation coefficient (ICC 2,1) with single measurements and absolute agreement was calculated for each level and presented with a 95% confidence interval (95% CI). A 1-way analysis of variance followed by a Bonferroni post hoc comparison test was performed to test differences between the groups. Statistical significance was set as P <.05. IBM SPSS Statistics, version 22.0 (Armonk, NY), was used for all statistical analyses.
Results
Inter- and intraobserver reliability was excellent (ICC >0.989 and >0.975, respectively) for the SVA when using weightbearing CT scans (Table 1). Slightly higher values were seen for the interobserver reliability.
Reliability Assessed by ICC (2,1). a
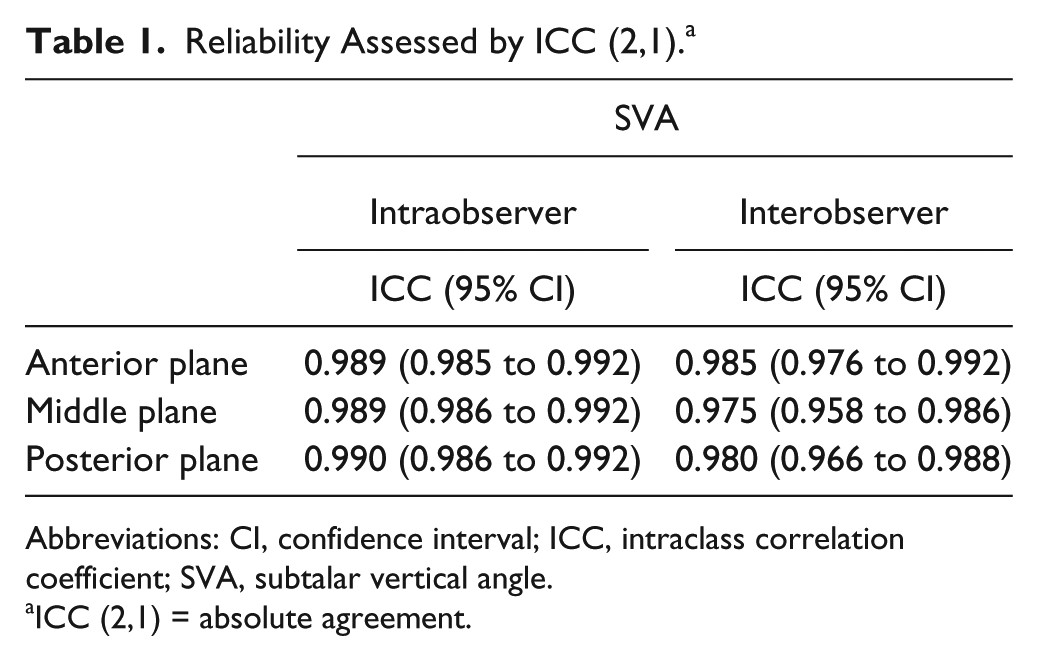
Abbreviations: CI, confidence interval; ICC, intraclass correlation coefficient; SVA, subtalar vertical angle.
ICC (2,1) = absolute agreement.
Using the connection between the center of the heel and the base of the second metatarsal in the axial plane for further reconstruction, the overall mean of the SVA (middle plane) of the healthy cohort was 98 (range 85-114) degrees. The mean SVA of the varus groups (incongruent and congruent, middle plane) was 91 (range 72-109) degrees and that of the valgus groups (incongruent and congruent, middle plane) 109 (range 97-120) degrees. Significant lower values of the SVA were measured for the varus groups (incongruent and congruent) compared to the valgus groups (P < .05; Table 2). This observation was independent of the coronal plane used for the determination (anterior, middle, or posterior) and independent of the rotation of the axis in the axial plane (5, 10, and 20 degree medial or lateral). The mean SVA of the control group was between the value of the varus and valgus groups (Figure 3).
Differences of the Subtalar Vertical Angle Between the Osteoarthritic Ankle Groups and the Control Group.
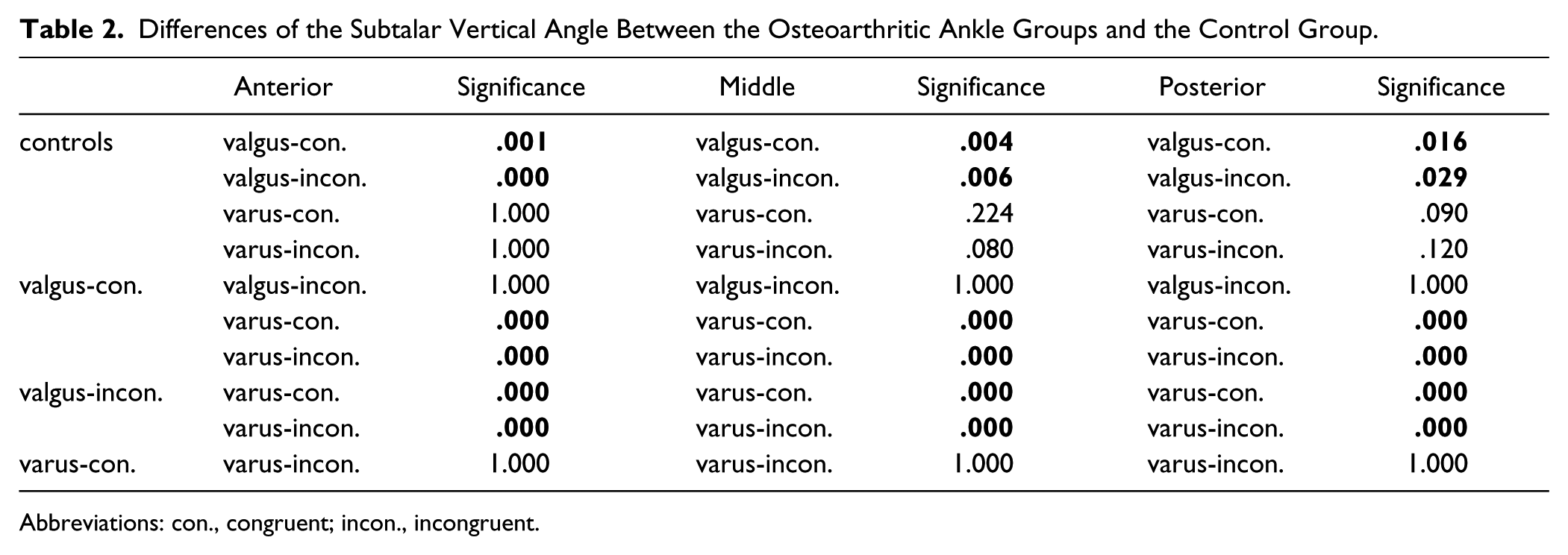
Abbreviations: con., congruent; incon., incongruent.
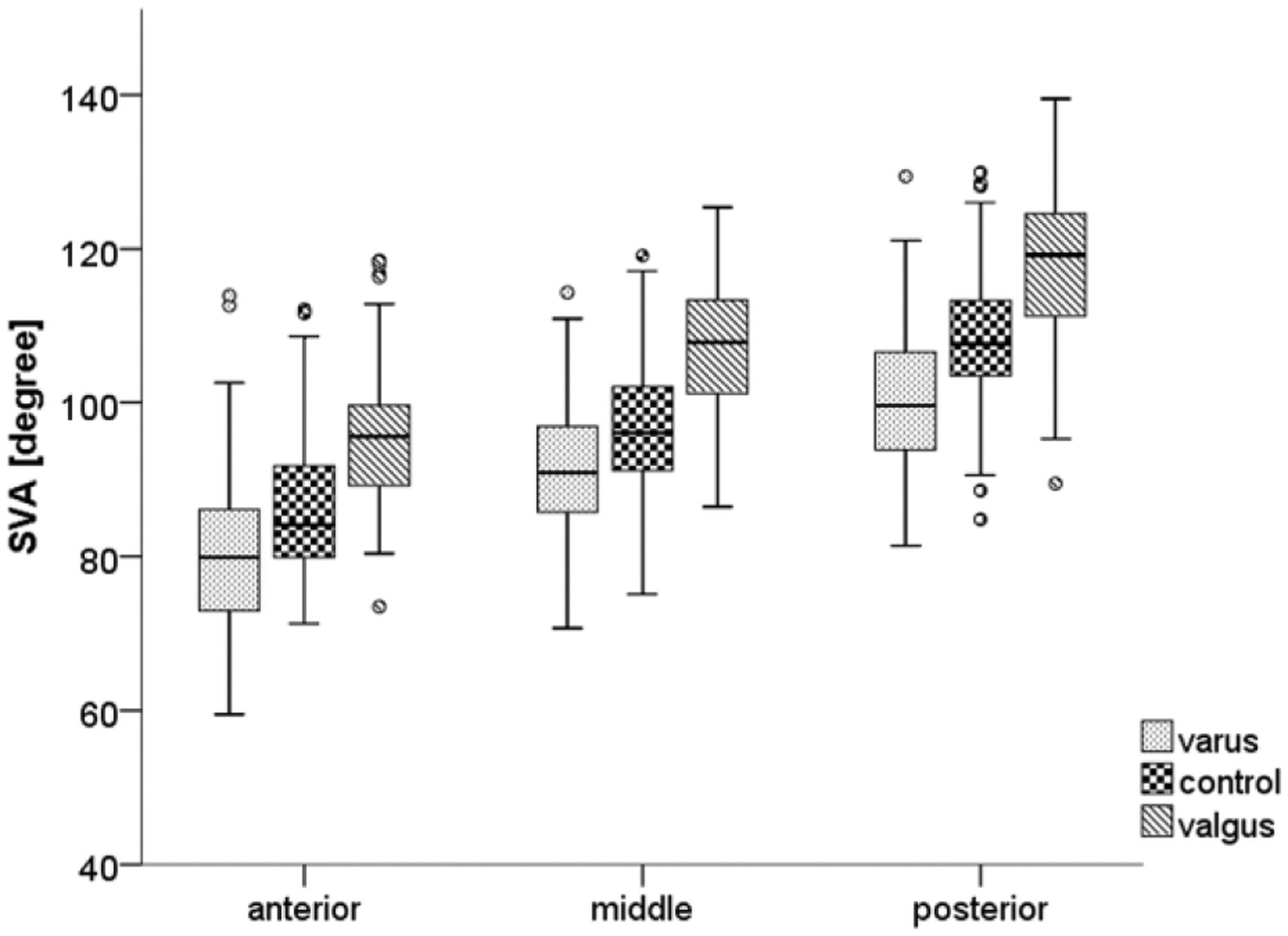
Mean of the subtalar vertical angle (SVA) in the varus groups (incongruent and congruent), control group and the valgus groups (incongruent and congruent). Significant differences of the SVA was determined between the varus and valgus groups (P < .05). No significant differences (P > .05) were found between the incongruent and congruent joint in each of the varus and valgus group.
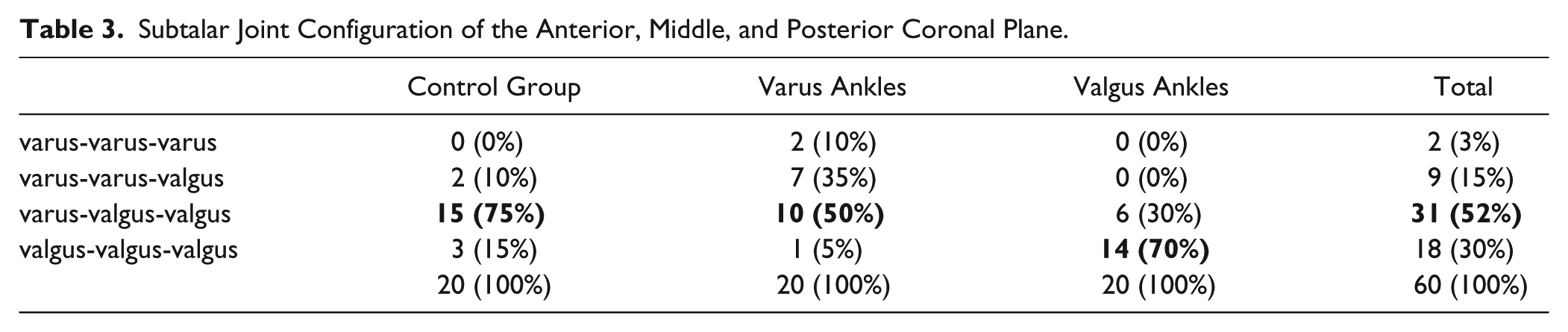
Subdivided into an anterior, middle, and posterior plane used for the determination of the SVA in the coronal plane, a varus-valgus-valgus configuration was the most common in the healthy control group (75%; Table 3). A varus-valgus-valgus configuration was mostly seen for arthritic varus ankles (50%), whereas a valgus-valgus-valgus configuration was usually seen in arthritic valgus ankles (70%). Significantly higher SVA values were observed on the posterior plane compared to the anterior plane (P < .05; Figure 3).
Subtalar Joint Configuration of the Anterior, Middle, and Posterior Coronal Plane.
Rotating the axis in the axial plane led to higher SVA values the more lateral the axis was set. No significant difference of the SVA was seen after rotating the principal axis in the axial plane 5 degrees medially or laterally (P > .05). A significant difference was only found between groups with a divergence of more than 20 degrees.
Discussion
Osteoarthritis of the ankle joint is relatively common and found in 1% of the world’s population. 19 A majority of these patients present with an asymmetric wear pattern in the affected ankle joint, that is, more degenerative wear in either the medial or the lateral aspect.4,6,11,19 Reasons are thought to be deformities of the lower leg and knee joint, ligamentous laxity, tendon dysfunction, and neurologic disorders.2,8,9,12,15,17,18 Recently, however, it has been proposed that the subtalar joint may have a major influence on this process.3-5,14 Authors have suggested that morphology and stability of the subtalar joint may influence hindfoot biomechanics. The present study analyzed the reliability of the assessment of the subtalar joint in the frontal plane and its orientation on weightbearing CT scans in osteoarthritic ankles compared to healthy ankles. The results suggest that the morphology of the posterior facet of the subtalar joint may play an important role in the evolution of ankle joint osteoarthritis.
Clinical and radiographic assessment of the subtalar joint is difficult. Therefore, there is a paucity of literature regarding the clinical impact of subtalar joint stability and morphology on hindfoot deformities. Plain radiographs of the hindfoot often do not allow an accurate assessment of the subtalar joint. Recent publications have assessed the use of weightbearing CT scans to analyze the subtalar joint morphology in hindfoot deformity.1,3,16 In our study, we were able to reliably reproduce the measurements of Van Bergeyk et al and Colin et al and found an excellent inter- and intraobserver reliability (>0.989 and >0.975, respectively) for the SVA.3,20 Furthermore, we were able to show that rotation in the axial plane did not influence the SVA if it did not exceed 5 degrees.
Little is known of the influence of the subtalar joint on the development of ankle joint osteoarthritis. Hayashi et al assessed the subtalar orientation in osteoarthritic ankles on plain radiographs. 4 In their study, the authors described the loss of the subtalar joint compensation in advanced stages of ankle joint osteoarthritis. They hypothesized that this loss may accelerate the degenerative wear in the ankle joint. However, having only used plain radiographs, the authors could not analyze the shape of the subtalar joint. Furthermore, the study only included patients with varus-type ankle joint osteoarthritis. Earlier studies using weightbearing CT scans stated that subtalar joint morphology is a risk factor for the development of tibialis posterior tendon dysfunction and subsequent flatfoot deformity.1,16 These authors described a pronounced valgus tilt of the subtalar joint in patients with acquired flatfoot deformity. However, to our knowledge, the present study is the first CT-based assessment of subtalar joint morphology, which may be a parameter that is a potential risk factor for ankle joint osteoarthritis.
The strength of this study is that all patients were assessed on a full weightbearing CT scan. This is in contrast to a majority of earlier reports, where simulated weightbearing was used.1,13,22 Accuracy of the SVA was tested by rotating the measurement plane in different directions, to assess reproducibility of the measuring method. The measurements were done by 3 independent examiners showing excellent inter and intraobserver reliability. In addition to the reference values of the SVA, we reassessed 20 healthy volunteers and observed similar findings as described in earlier publications. 3 Furthermore, the SVA was determined on an anterior, middle, and posterior coronal plane taking into consideration the screw-shaped anatomy of the posterior facet. For the determination of the varus/valgus configuration of the subtalar joint, the assessment was sufficient using the middle coronal plane.
Our study has numerous limitations. Only patients with advanced stages of the osteoarthritic process and consequently a distinct varus/valgus deformity were included. The previous studies using the SVA exclusively included normally aligned, healthy hindfeet.3,20 The SVA may be influenced by the tilt in the ankle joint. We tried to assess this potential bias by subtracting the measured tilt angle (TTS) on the radiographs from the SVA. In our cohort this did not have an influence on the principle findings, that is, varus angles in the SVA remained in varus and valgus angles remained in valgus. Future investigations will need to elucidate whether the SVA or the measurements used by Probasco et al are more reliable in the malaligned hindfoot.3,16,20 Second, the anatomy of the subtalar joint varies considerably and in a majority of cases consists of 3 facets. Therefore, the observed varus/valgus orientation of the posterior facet may have a limited effect on the load distribution in the ankle joint.
In summary, the SVA measured on weightbearing CT scans was a reproducible and consistent method to determine the varus/valgus configuration of the posterior facet of the subtalar joint. For both the varus and the valgus type of ankle joint osteoarthritis, we found significant differences of the SVA when comparing them with a healthy cohort. This suggests that the orientation of the subtalar joint may play an important role in the development of ankle joint osteoarthritis.
Footnotes
Authors’ Note
This study was approved by the ethics committee EKNZ (number 313/13 and 2014/303).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by a grant from the Swiss Foot and Ankle Society.