
Abstract
Background:
Metatarsalgia is frequently associated with hallux valgus. The aim of this study was to evaluate how the relative length and position of the first metatarsal head influenced metatarsalgia and plantar callosities beneath the lesser metatarsal heads.
Methods:
A retrospective analysis of the clinical data and radiographs of 102 cases was performed at a mean follow-up of 16 months after biplane interlocking osteotomies. Clinical evaluation was made using the Japanese Society for Surgery of the Foot (JSSF) hallux scale. Radiologic evaluation was made with standard weight-bearing anteroposterior radiographs, and the hallux valgus angle (HVA), intermetatarsal 1-2 angle (IMA), distal metatarsal articular angulation (DMAA), and the sesamoid position were evaluated. Relative first metatarsal length (RML) was determined according to Nilsonne/Morton’s technique.
Results:
The mean preoperative HVA decreased from 37 to 3 degrees, and the mean IMA from 17 to 4 degrees. The mean JSSF-hallux score improved from 56 to 96 points. The mean preoperative area of plantar callosities decreased from 3.1 to 1.5 mm2. Sixty percent of metatarsalgia cases improved, and 85% of painless callosities disappeared postoperatively. Among radiologic parameters, postoperative RML was most significantly associated with JSSF score (P < .0001) and the presence of postoperative metatarsalgia (P < .0001). Receiver operating characteristic analysis revealed that the RML cut-off point was −3 mm for avoiding metatarsalgia, with an area under the curve of 0.88, a specificity of 88%, and a sensitivity of 85%.
Conclusion:
Preservation of relative first metatarsal length during first metatarsal osteotomy was important to prevent postoperative metatarsalgia.
Level of Evidence:
Level IV, retrospective case series.
Keywords
Introduction
Metatarsalgia is frequently associated with hallux valgus.2,8,15,26 Discrepancies in metatarsal lengths are believed to be an etiology of metatarsalgia in hallux valgus patients.4,12,23 Lesser metatarsals that are relatively long predispose individuals to mechanical overload under the metatarsal heads during the propulsive phase of gait. 4 Continuing pressure at the metatarsal heads induces inflammation of the plantar soft tissue as well as reactive keratosis of the plantar skin and results in painful plantar callosities, which is known as metatarsalgia.4,12
When correcting moderate to severe hallux valgus, first metatarsal osteotomy is usually required in combination with distal soft tissue procedures. It is well accepted that shortening of the first metatarsal occurs after most metatarsal osteotomies. As shown by several studies, the major problem with excessive shortening is the occurrence of a transfer lesion under the second metatarsal head.3,8,14,28 However, there has been no consensus regarding what degree of shortening of the first metatarsal is acceptable during corrective osteotomy for hallux valgus.
The aim of this study was to evaluate how the relative length of the first metatarsal influenced the development of metatarsalgia and plantar callosities of the lesser metatarsal heads in hallux valgus patients.
Methods
We retrospectively evaluated 51 patients (102 feet) who underwent surgery between January 2011 and December 2013 by a single surgeon in a single center. Forty-eight cases were bilateral. There were 43 women and 8 men. The median age was 58 years (range, 11−80). The mean follow-up was 16 months (range, 12−29). The inclusion criterion was symptomatic hallux valgus with no previous surgical intervention. Patients with rheumatoid arthritis and gout were excluded. Information on metatarsalgia, plantar callosities, radiographic analysis, and complications were obtained from the patients’ medical records. Clinical evaluation was conducted using the Japanese Society for Surgery of the Foot (JSSF) hallux scale, which is a modification of the American Orthopaedic Foot & Ankle Society scale (Supplemental Table).20,21 Patient demographics are shown in Table 1. The mean follow-up duration was 16 months (range, 12–29).
Pre- and Postoperative Comparison of Radiographic and Clinical Indices.
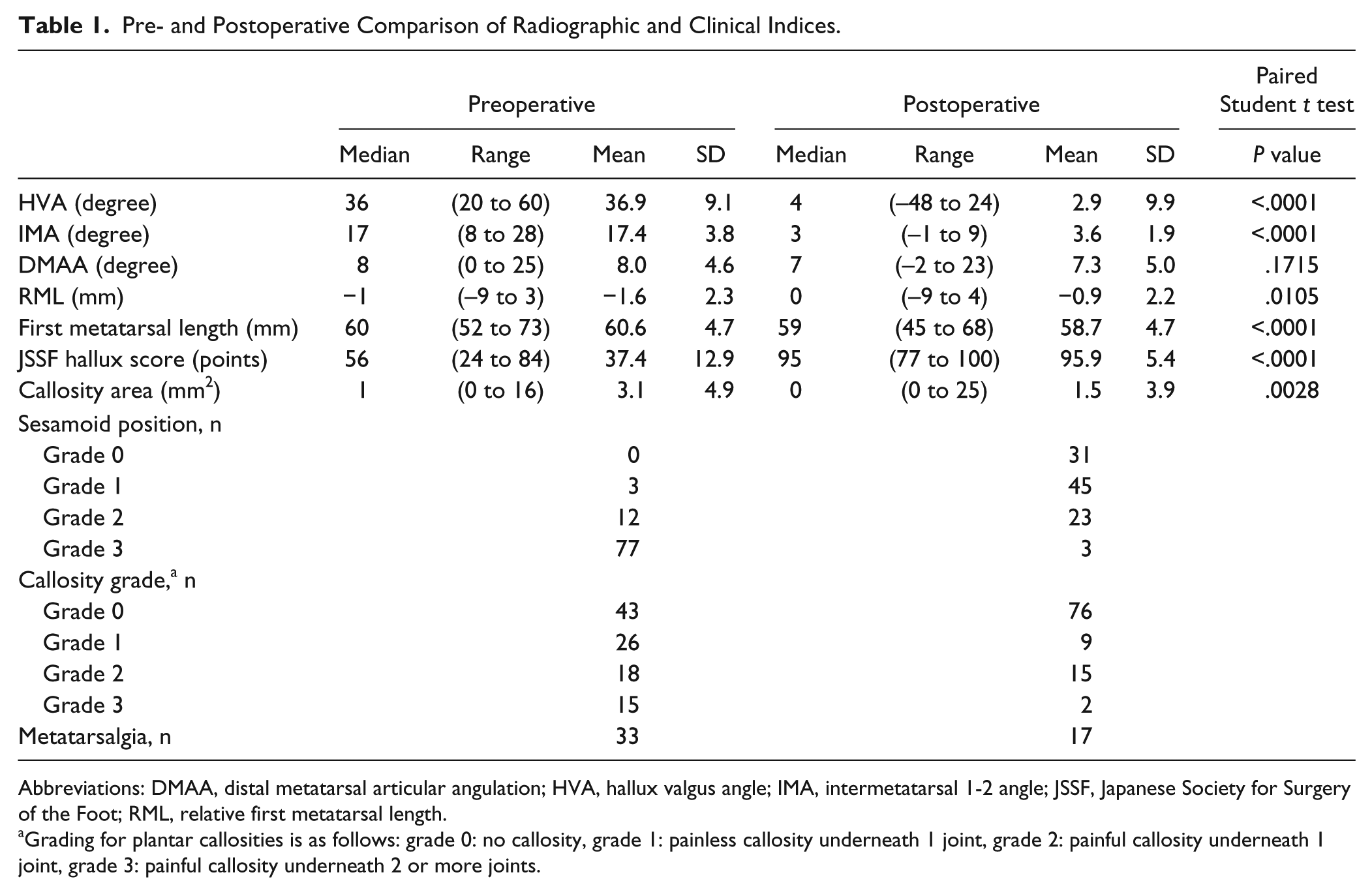
Abbreviations: DMAA, distal metatarsal articular angulation; HVA, hallux valgus angle; IMA, intermetatarsal 1-2 angle; JSSF, Japanese Society for Surgery of the Foot; RML, relative first metatarsal length.
Grading for plantar callosities is as follows: grade 0: no callosity, grade 1: painless callosity underneath 1 joint, grade 2: painful callosity underneath 1 joint, grade 3: painful callosity underneath 2 or more joints.
We evaluated the severity of plantar callosities, taking into account the distribution of each callus and the presence of pain. Regarding the area of callosities, both long (L) and short (S) axes were measured using a ruler, and the area was calculated as (L × S) (mm2). The presence of pain was noted if the patient felt pain when walking barefoot on a floor. The grading scale we developed in this study was as follows: grade 0, no plantar callosities; grade 1, callosity without pain; grade 2, painful callosity beneath 1 joint; grade 3, painful callosity beneath 2 or more joints (Figure 1). The areas of callosities were significantly different between different grades (except for grades 0 vs 1; Table 2).
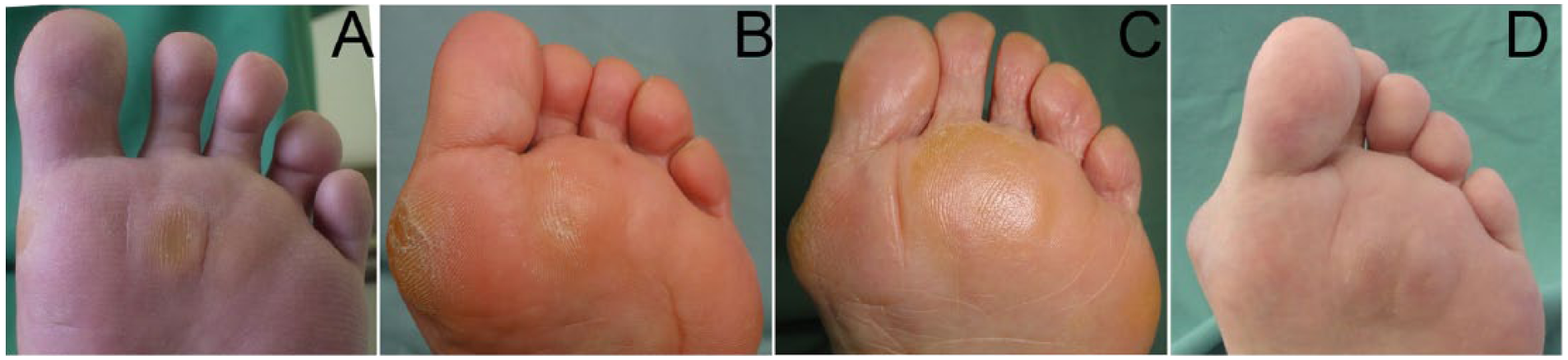
Grading of plantar callosities. The grading scale we developed in this study was as follows: Grade 0, no plantar callosities (not shown). Grade 1, callosity without pain (A). Grade 2, painful callosity beneath 1 joint (B). Grade 3, painful callosity beneath 2 joints or more (C and D).
Changes in the Grades of Plantar Callosities Beneath Lesser Metatarsal Heads.
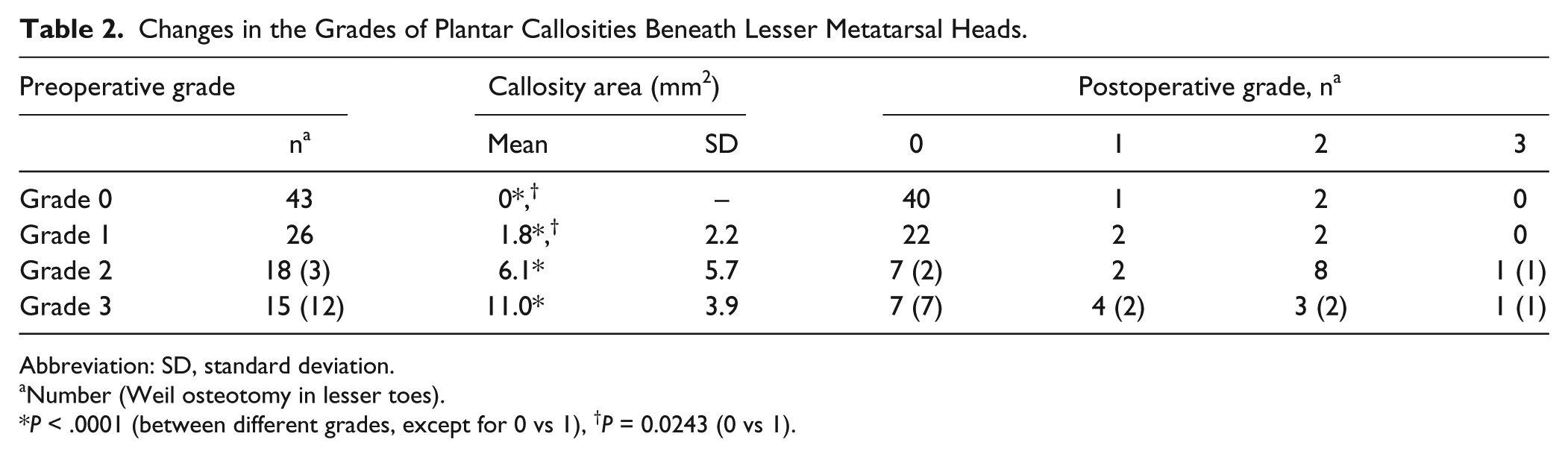
Abbreviation: SD, standard deviation.
Number (Weil osteotomy in lesser toes).
P < .0001 (between different grades, except for 0 vs 1), †P = 0.0243 (0 vs 1).
Metatarsalgia was defined as present if the patient felt pain when walking barefoot on a floor. All patients with metatarsalgia (n = 33) presented with plantar callosities (grade 2, 18 feet; grade 3, 15 feet).
Radiologic evaluation was based on standard weight-bearing anteroposterior radiographs, and the hallux valgus angle (HVA), inter-metatarsal 1-2 angle (IMA), and distal metatarsal articular angulation (DMAA) were measured. The sesamoid position was evaluated using the methods of Smith et al. 27 The length of the first metatarsal was measured using the method of Munuera et al 17 with some modification. A long axis was drawn on the first metatarsal as when measuring HVA and IMA. Points of intersection of the long axis with the distal end of the metatarsal head (A) and the proximal end of the metatarsal base (B) were marked. The length of the first metatarsal was determined as the distance between A and B. Relative first metatarsal length (RML) was evaluated according to Nilsonne/Morton’s technique16,22 and was defined as the distance between tangents on the ends of the metatarsal heads drawn perpendicular to the longitudinal axis of the second metatarsal. A positive index implied that the first metatarsal was longer than the second (Figure 2).
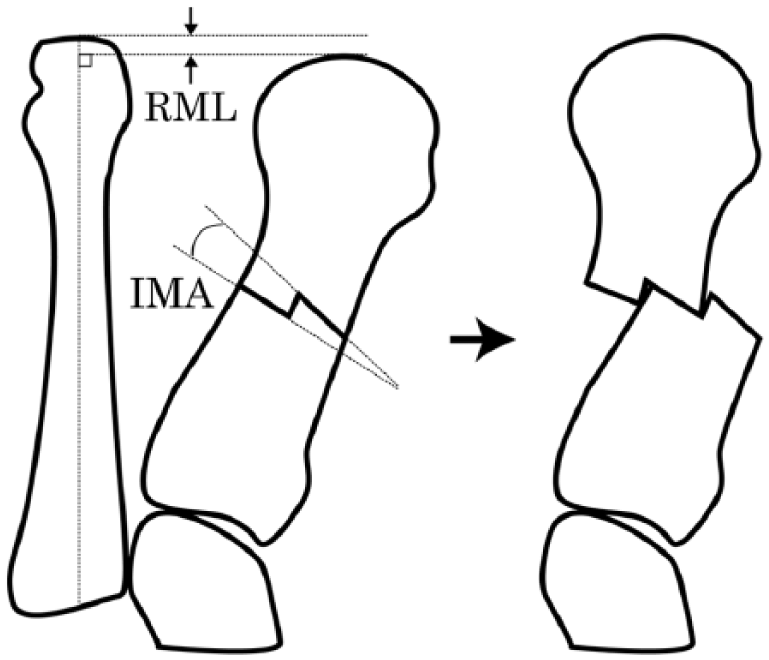
Biplane interlocking osteotomy, depicting (1) 2 osteotomy lines with an angle identical to the intermetatarsal angle (IMA), (2) lateral translation, and (3) interlocking of the medio-proximal corner of the distal segment with the inclined lateral plane of the proximal segment. With more angulated (varus) osteotomy lines, the first metatarsal can be elongated if necessary. Relative metatarsal length (RML) is also indicated.
Complications included any infection, delayed wound healing, malunion, recurrence of hallux valgus (HVA greater than 20 degrees), and hallux varus (HVA less than 0 degrees).
Statistical analyses were performed using JMP Pro 10.0.2 (SAS Institute Inc, Cary, NC). The preoperative data were compared with the results at follow-up using the paired Student t test at the 95% significance level. The association between callosity grading and radiologic parameters was analyzed using the t test. Receiver operating characteristic (ROC) analysis was used to obtain a representative cut-off value for RML based on the presence or absence of postoperative metatarsalgia.
Surgical Technique
Hallux valgus was corrected using biplane interlocking osteotomy (BIO).18,19 A medial longitudinal incision was made on the first metatarsophalangeal (MTP) joint. A chevron capsulotomy was performed, exposing the MTP joint, and the medial eminence was then resected. A lateral release was always performed through a separate dorsal incision. The first metatarsal was exposed in the midshaft subperiosteally, and the BIO procedure was then performed. Drill holes (1.2-mm) were made in the midpoints of both the longitudinal and transverse axes. Two osteotomy lines were marked. A medial line was drawn distal to the drill hole, and a lateral line was made proximally with the same angle as the IMA. Biplane osteotomy was completed using a micro bone saw. The distal fragment was slid laterally, and the step was interlocked with the medial corner of the distal stump of the proximal metatarsal fragment. Depending on the osteotomy lines, the first metatarsal length could be lengthened (Figure 2). Fixation was performed with a ring screw (Nakashima Medical, Okayama, Japan) and locking plate (LPS or TOM plate; Wright Medical, Memphis, TN) (Figure 3). The medial side of the capsule was plicated until the intraoperative HVA was smaller than 5 degrees. The abductor hallucis tendon was also plicated dorsally.

Pre- and postoperative radiographs of the same patient showing correction of hallux valgus after biplane interlocking osteotomy. Fixation was performed with a ring screw and locking plate. The first metatarsal length was 61 mm preoperatively and 60 mm postoperatively. The relative metatarsal length improved from −1 mm preoperatively to 0 mm postoperatively.
Weil’s shortening osteotomy of the second metatarsal was additionally performed in 15 feet (3 feet with grade 2 and 12 feet with grade 3), as follows. Bone slice resection was not performed. The metatarsal head was shifted backward approximately 3 to 7 mm until the MTP joint was easily reduced, and the metatarsal head fragment was then fixed with 2 small screws (Charlotte Snap-off screw [Wright Medical] and a modular hand screw [DePuy Synthes, West Chester, PA]). The lesser toes were fixed with a K-wire for 3 weeks.
Each affected foot was placed in a soft bulky dressing, and a fiberglass cast was applied over the dressing for 1 week. At 2 weeks, the patients were weightbearing on the lateral side of the foot with a stiff-soled shoe, with the hallux kept in a neutral to slightly varus position. At 4 weeks, the patients were weightbearing outside with a stiff-soled shoe that was used until the bone healing was complete.
Results
The mean HVAs pre- and postoperatively were 36.9 and 2.9 degrees, respectively (P < .0001). The mean IMAs pre- and postoperatively were 17.4 and 3.5 degrees, respectively (P < .0001). The mean DMAAs pre- and postoperatively were 8.0 and 7.3 degrees, respectively (P = .1715). The mean decrease in the first metatarsal length was 1.9 mm (range, –9 to 11) (P < .0001). Preoperatively, the majority (97%) of feet showed a sesamoid position of grade 2 or 3. Postoperatively, 83% of feet showed an improvement in the sesamoid position to grade 0 or 1. Metatarsalgia (grades 2 and 3) was observed pre- and postoperatively in 33 feet (32%) and 17 feet (16%), respectively. The mean callosity areas pre- and postoperatively were 3.1 and 1.5 mm2, respectively (P = .0028). The mean JSSF-hallux scores pre- and postoperatively were 56.2 and 95.9 points, respectively, a mean improvement of 39 points (range, 16–74) (Table 1). The results were excellent for the overall JSSF score as well as the scores of each subcategory. Among the radiologic parameters, postoperative RML was significantly associated with the area of callosities (P < .0001) and the JSSF score (P < .0001).
Three feet (2.9%) developed recurrence of the hallux valgus (HVA of greater than 20 degrees), which required no treatment. Twenty-two feet (22%) developed hallux varus deformity (HVA of less than 0 degrees; 0 to −10, 16 feet; less than −11, 6 feet), all of which were flexible and required no treatment. Three feet (2.9%) had nonunion, which required revision surgery followed by low-intensity pulse ultrasound (LIPUS). Six feet (5.7%) had delayed union that was treated with LIPUS. One patient had an infection that required plate removal.
To evaluate metatarsalgia, we graded plantar callosities according to the presence of pain and the distribution of the lesions (Figure 1). Preoperative plantar callosities (grades 1, 2, and 3) were observed in 59 feet (57.7%). Higher grades were associated with larger lesion areas, supporting the rationale of this grading system (Table 2).
Preoperative metatarsalgia (grades 2 and 3) was observed in 33 feet (32%), and 20 feet (61%) were pain free postoperatively (Table 2). Weil’s shortening osteotomy of the second and/or third metatarsal was additionally performed in 15 feet in this group. Feet that underwent Weil’s osteotomy demonstrated a higher recovery rate (73%; 11 feet became pain free) than those that did not (50%, 9 of 18 feet) (P = .1569). New-onset metatarsalgia developed postoperatively in 4 feet, and was considered to be transfer metatarsalgia. The presence of postoperative metatarsalgia was significantly associated with postoperative RML and the first metatarsal length (P < .0001, logistic regression), but not with HVA or IMA.
Table 3 shows the difference in RML between each grade of callosity. Preoperative RMLs in feet with grade 2 and 3 metatarsalgia were significantly smaller than those in feet of grade 0 (P < .001 and P = .0175, respectively). With the numbers available, no significant difference was observed between grades 0 and 1 or 1 and 2. Postoperatively, the RML of grade 2 cases (−3.9 mm) was significantly smaller than that of lower grades (−0.4 and −1.0 mm, P < .001). These data suggest that an excessive decrease in the relative first metatarsal length caused painless callosities and subsequent metatarsalgia as shortening increased. In addition, in grade 2 cases, postoperative RML (−3.9 mm) was much smaller than that preoperatively (−1.9 mm). This indicates that in the preoperative hallux valgus, metatarsalgia was likely to be associated with even mild shortening of RML as compared with postoperative feet.
Association of Relative Metatarsal Length With Plantar Callosities.
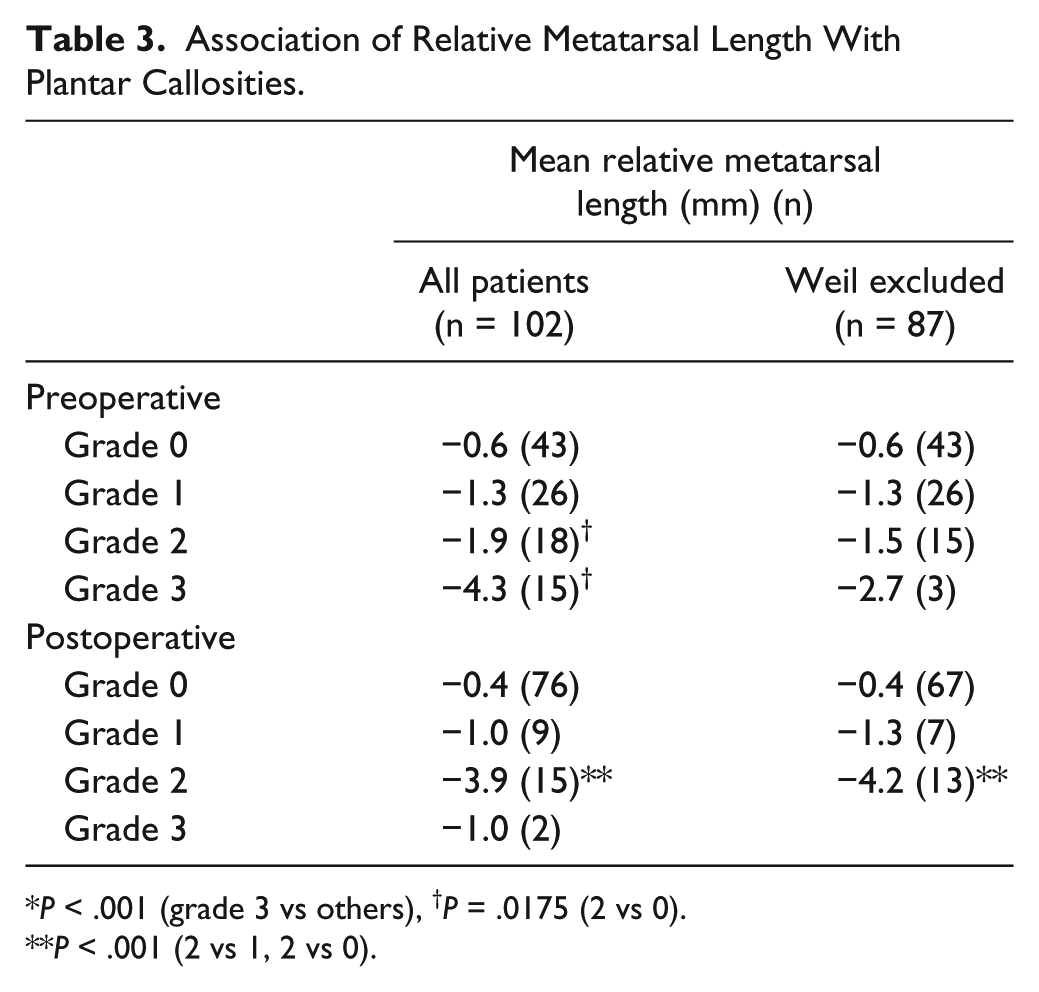
P < .001 (grade 3 vs others), †P = .0175 (2 vs 0).
P < .001 (2 vs 1, 2 vs 0).
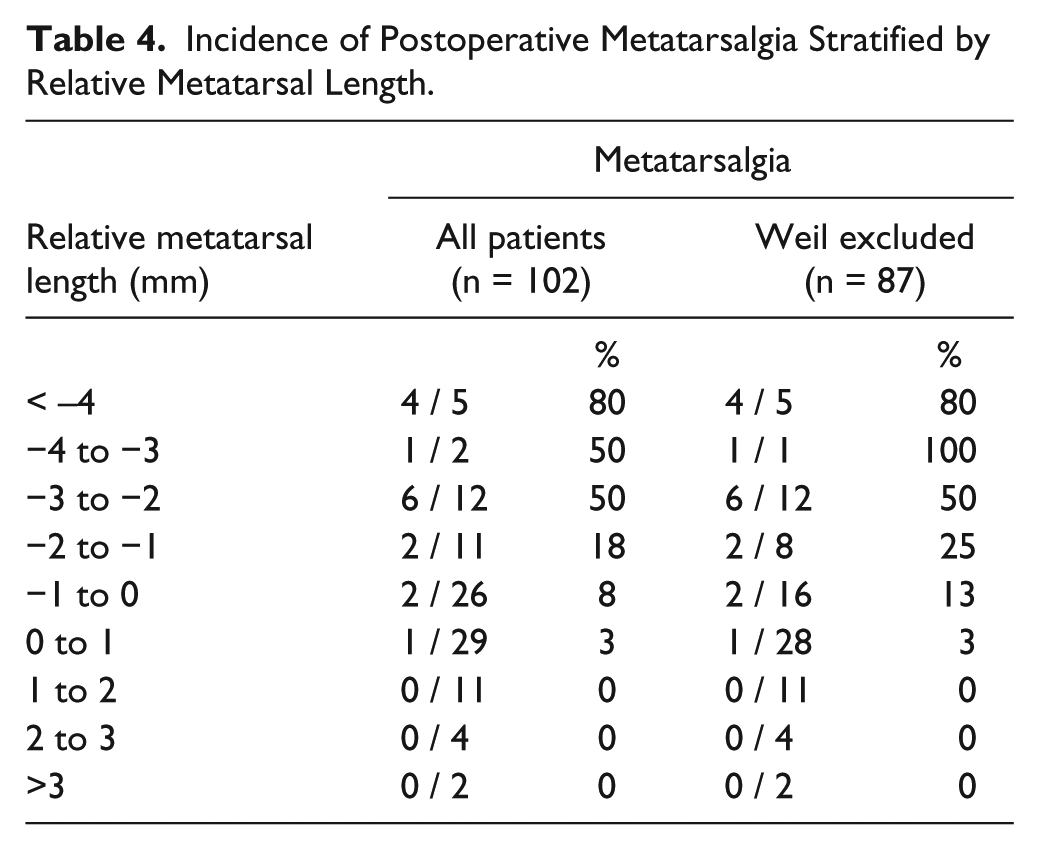
Table 4 shows the incidence of postoperative metatarsalgia and RML. No callosities were observed in feet with RML greater than 1 mm, regardless of whether Weil’s shortening osteotomy was performed. To determine the acceptable shortening in RML, ROC analysis was performed. Fifteen feet that underwent Weil’s osteotomy of the second metatarsal were excluded from the analysis, because this procedure not only affects RML directly but also changes the sagittal alignment of the second metatarsal. The cut-off point for the presence of metatarsalgia was −3 mm, with an AUC of 0.88, a specificity of 88%, and a sensitivity of 85%.
Incidence of Postoperative Metatarsalgia Stratified by Relative Metatarsal Length.
Discussion
There has thus far been no consensus regarding the ideal length and position of the first metatarsal head during corrective osteotomy for hallux valgus. 6 Many authors have reported that too much shortening of the first metatarsal should be avoided because of the risk of transfer metatarsalgia.3,5,7,14,26,28 For example, Carr and Boyd reported 4 mm as an acceptable range for postoperative shortening. 3 In this study, we utilized the method of Nilsonne/Morton to measure the relative shortening of the first metatarsal as RML. The incidence of postoperative metatarsalgia was significantly associated with shorter mean RML (P < .0001), indicating the importance of the relative length of the first metatarsal. ROC analysis revealed that an RML of −3 mm predicted postoperative metatarsalgia with a specificity of 88% and a sensitivity of 85%. We believe that measuring RML using Nilsonne/Morton’s method is reasonably quick, easy to perform intraoperatively under fluoroscopic guidance, and useful in daily practice.
Several studies have reported the surgical outcomes of metatarsalgia associated with hallux valgus. Recovery rates (the disappearance of metatarsalgia) after hallux valgus correction without lesser metatarsal osteotomy have ranged from 48% to 80%.11,13,24,29 In our study, the recovery rate of preoperative metatarsalgia in the feet without Weil osteotomy was 50% (9 of 18 feet with preoperative grades 2 and 3). In contrast, 15 feet with additional Weil osteotomy (grade 3, 12 feet; grade 2, 3 feet) showed a higher complete recovery rate of 73% (11 of 15 feet), although this difference was not significant (P = .157). In the group of feet where callosity grades worsened postoperatively, the mean postoperative RML was −4.0 mm. The mean postoperative increase in RML was 0.6 mm, and the mean preoperative RML in grade 3 feet was significantly smaller than other grades, at −4.3 mm (P < .001). These observations suggest that in feet with small RML or grade 3 callosities preoperatively, further shortening of the first metatarsal should be avoided and additional shortening osteotomy of the second metatarsal may be considered.
A literature review identified no studies that analyzed the relationship between the severity of plantar callosities beneath the lesser metatarsals and the postoperative position of the first metatarsal head. In this study, we developed a new grading system for plantar callosities, based on the pain and size of the lesion. The area of the lesion was correlated with the severity of the grade (Table 2), supporting the rationale of this grading system. Among the 4 radiographic parameters evaluated (HVA, IMA, M1 length, and RML), RML was most significantly associated with the incidence of plantar callosities (P < .0001), further indicating the importance of the axial position of the first metatarsal head.
Our BIO procedure has the advantage of avoiding shortening of the first metatarsal, which occurs after most metatarsal osteotomies.18,19 Chevron osteotomy was reported to result in an average shortening of 2.2 mm. 9 Greater shortening, as much as 10 mm, has been reported after Wilson osteotomies. 10 Compared to prior reports, the average shortening in this study was much less (1.0 mm, range 0-2). In our BIO procedure, the distal segment is displaced laterally and distally so that the first and second metatarsals are parallel to each other. This oblique sliding can compensate for, or even overcome when necessary, the shortening caused by the step (1.2 mm) between the medial and lateral planes. After the medial corner of the distal segment interlocks with the inclined lateral plane of the proximal segment, a locking plate firmly fixes both segments. This plate fixation makes the correction powerful and long lasting, and minimizes the negative effect of shortening of the first metatarsal. When performing the BIO procedure, we usually design the osteotomy lines to obtain an RML of 0 mm, which results in an actual postoperative RML of approximately −1.0 mm.
The reported frequency of hallux varus after hallux valgus surgery is 2% 25 to 12% 13 ; however, we observed a high proportion of cases with hallux varus (22%) postoperatively. We usually correct HVA to 0 degrees by tightening of the medial MTP joint capsule. In addition, the hallux is kept in a neutral to slightly varus position in a postoperative stiff-soled shoe, which we believe is useful in maintaining correction. As a result, the recurrence rate of hallux valgus in our study was relatively low (2.9%) compared with previous reports (3% 13 to 30% 1 ). Although none of the patients with hallux varus were dissatisfied and required further treatment, both intraoperative correction and postoperative management require optimization in the future.
Several limitations of this study should be considered. First, there were no data to evaluate the sagittal plane alignment, because it was difficult to assess the dorsiflexion of the first metatarsal on lateral radiographs. Second, we used a mean intermediate follow-up duration of 16 months. A longer follow-up study is recommended.
Conclusion
Preservation of relative metatarsal length during first metatarsal osteotomy was important to prevent postoperative metatarsalgia. We found the RML cut-off point was −3 mm for avoiding postoperative metatarsalgia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.