
Abstract
Background:
Arthrodesis is a common operative procedure used to manage arthritis and deformity in the foot and ankle. Nonunion is a possible and undesirable outcome in any arthrodesis surgery. Rates of nonunion in the foot and ankle literature range from 0% to 47% depending on the patient population and joint involved. Multiple factors can contribute to developing a nonunion including location, fixation method, tobacco use, diabetes, infection, and others.
Methods:
The case logs of 3 foot and ankle surgeons were reviewed from January 2007 to September 2014 to identify nonunion arthrodesis revision cases. The patient factors reviewed included diabetes, inflammatory arthropathy, tobacco use, history of infection, nonunion elsewhere, neuropathy, Charcot arthropathy, posttraumatic arthritis, and prior attempt at revision arthrodesis at the same site. Operative records were reviewed to identify location of the nonunion, instrumention, use of allograft or autograft bone, use of iliac crest bone marrow aspirate (ICBMA) and use of orthobiologics such as bone morphogenetic protein (BMP) during the revision arthrodesis. Successful revision was defined as radiographic union on the final radiograph during follow-up. Eighty-two cases of revision arthrodesis were identified with an average follow-up of 16 months.
Results:
The overall nonunion rate was 23%. Neuropathy and prior attempts at revision were identified as significant risks (P <.05) for persistent nonunion. Odds ratio calculated based on previous attempts at revision arthrodesis found a 2.8-fold increase in the risk of failure for each attempt at revision.
Conclusion:
Revision arthrodesis for nonunion in the foot and ankle was successful (77%) under a variety of patient and operative conditions. Neuropathy was a significant patient risk factor for persistent nonunions, and we believe it is important to identify even in the nondiabetic patient. As the number of attempts at revisions increases, there is a subsequent 3-fold increase in the risk of persistent nonunion.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Arthrodesis is a common operative procedure used to manage arthritis and deformity in the foot and ankle. Nonunion or failure of the bone to fuse, is a known possible outcome in any arthrodesis surgery and often presents as persistent pain and swelling after an arthrodesis procedure. Published rates of nonunion in the foot and ankle literature range from 0% to 47% depending on the patient population and joint involved.22,23 Multiple factors can contribute to developing a nonunion, including arthrodesis location, fixation method, tobacco use, diabetes, infection, and others. 23
Although all foot and ankle orthopedic surgeons treat nonunions, management recommendations vary widely, from no intervention in the first metatarsophalangeal joint to use of external fixators with bone stimulator in the ankle joint.12,21 Various techniques for augmentation with bone grafting have been discussed in both primary and revision arthrodesis.3,17,19 In addition, over the past several years there have been additional studies looking at the use of orthobiologics in both primary arthrodesis procedures and treatment of fracture nonunion.4,24
Although multiple studies have evaluated subjects with nonunion of an arthrodesis, sample sizes are frequently small and intermixed, with patients undergoing primary arthrodesis. The aim of this study was to comprehensively evaluate all cases of revision arthrodesis for nonunion to identify patient and operative factors that might have affected the success of revision joint arthrodesis in the foot and ankle.
Methods
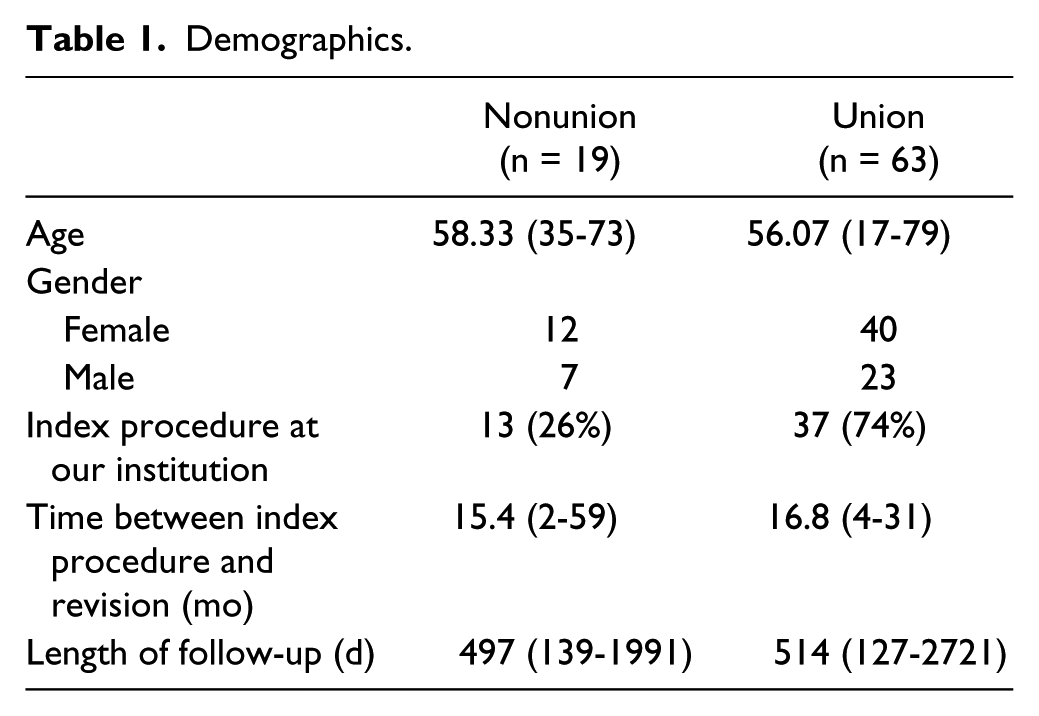
Institutional review board approval was obtained prior to beginning this retrospective review. The case logs of 3 fellowship-trained foot and ankle surgeons were reviewed from January 2007 to September 2014. ICD-9 code 733.82 (nonunion fracture), 998.89 (miscellaneous complication), and a word search for nonunion in case logs were used to identify subjects. Two hundred sixty-five possible arthrodesis nonunion cases were identified. From these 265 cases, a chart review identified 100 cases of revision joint arthrodesis. Patients were excluded from this group if (1) follow-up was less than 120 days (10 patients), (2) the revision procedure addressed toe interphalangeal joints (7 patients), or (3) multiple nonunion sites were treated at different times in the same foot (1 patient). Overall 82 subjects, 32 men and 50 women, were included for analysis with an average follow-up of 16.5 months (range, 4 to 90). The revision procedures took place an average of 16 months (range, 2 to 59 months) after the index procedure. The average length of follow-up for patients was 16 months for the nonunions and 17 months for the unions. Demographic data are presented in Table 1.
Demographics.
Clinical charts were reviewed to identify patient-specific factors for nonunion. The following patient factors were recorded: diabetes, inflammatory arthropathy, tobacco use, history of infection, prior nonunion elsewhere in the body, neuropathy, Charcot arthropathy, posttraumatic arthritis, and prior attempt at revision arthrodesis at the same clinical site. Operative notes were reviewed to identify the location of the nonunion, type of instrumention, use of structural allograft, use of cancellous autograft (CA), use of iliac unconcentrated crest bone marrow aspirate (ICBMA), and use of orthobiologics such as bone morphogenetic protein (BMP) during the revision arthrodesis.
Outcomes of the revision arthrodesis were determined by interpretation of final radiograph during clinical follow-up. Clinic notes were reviewed to determine the attending orthopedic surgeons’ interpretations of the final radiographic images, and these interpretations were compared to the radiologist’s interpretation of the same images. Images were classified into 3 categories: nonunion, union, and indeterminant. If a discrepancy existed between the orthopedic and radiology interpretations, or when the interpretation was indeterminate (neither surgeon nor radiologist stated a firm conclusion), a case was further reviewed. The final radiographs for these patients were blinded without clinical information and examined by the 3 senior authors to determine a consensus interpretation of union or nonunion.
Statistical analysis
In order to assess the association between patient and operative factors, and nonunion following revision arthrodesis, we conducted contingency table (qualitative factors) and logistic regression (quantitative factors) analyses. P values were estimated using the likelihood ratio chi-square test, and Fisher exact test was used when more than 20% of the cells had expected counts less than 5 (P ≤ 0.05 considered significant). Analyses were conducted using PROC FREQ (contingency tables) and PROC LOGISTIC (logistic regression) in SAS version 9.4.
Results
Radiographic interpretation was consistent between the attending orthopedist and radiologist in 60 cases (12 nonunion and 48 union). Twenty-two cases were found to have discordance (20) or “indeterminant” (2) interpretations. After blinded review of these 22 patients’ radiographs, 7 were deemed nonunion, 15 deemed healed. A total of 19 nonunions after revision arthrodesis were identified in the 82 subjects undergoing a revision procedure for the management of an arthrodesis nonunion during the study period.
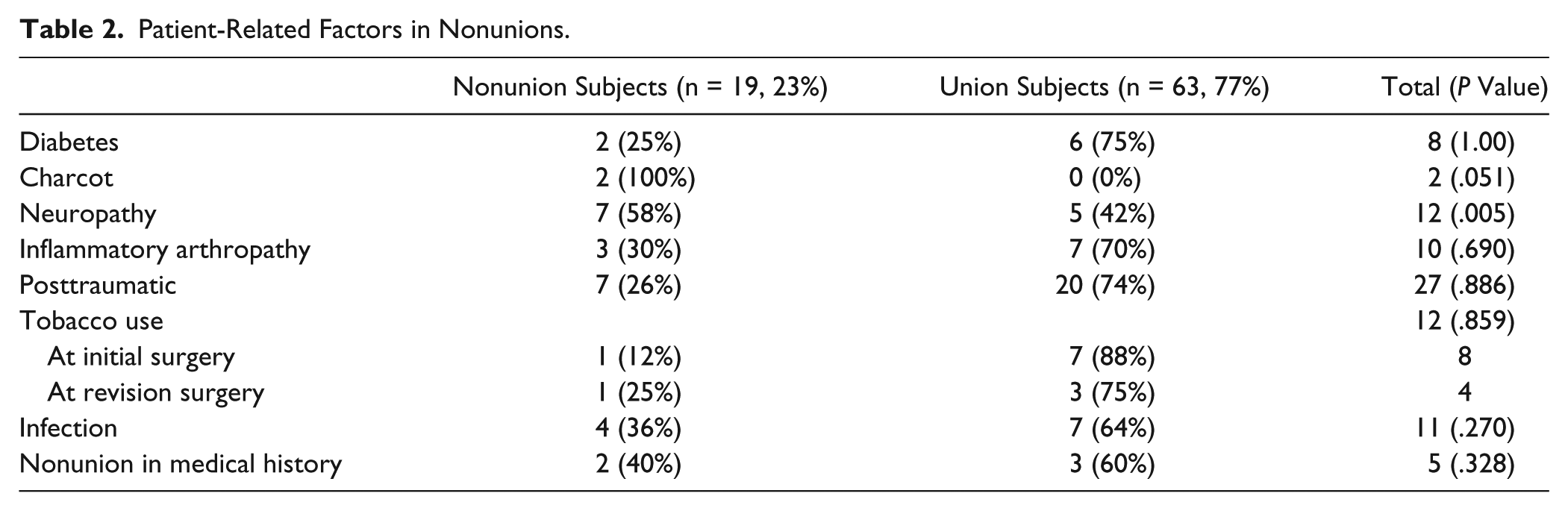
The overall nonunion rate after revision across all patients in this study was 23%. Further analysis of data was performed based on patient-specific and surgery-specific factors. Patient-specific factors included diabetes, tobacco use, Charcot arthropathy, neuropathy, inflammatory arthropathy, infection, posttraumatic arthropathy, and history of nonunion at other sites (Table 2). The surgery-specific factors were defined as the use of allograft, autograft, or orthobiologics at the time of revision (Table 3). In addition, the number of prior revision attempts as well as the location of the nonunion was evaluated for a possible effect on the likelihood of union (Tables 4 and 5).
Patient-Related Factors in Nonunions.
Surgery-Related Factors in Nonunion.
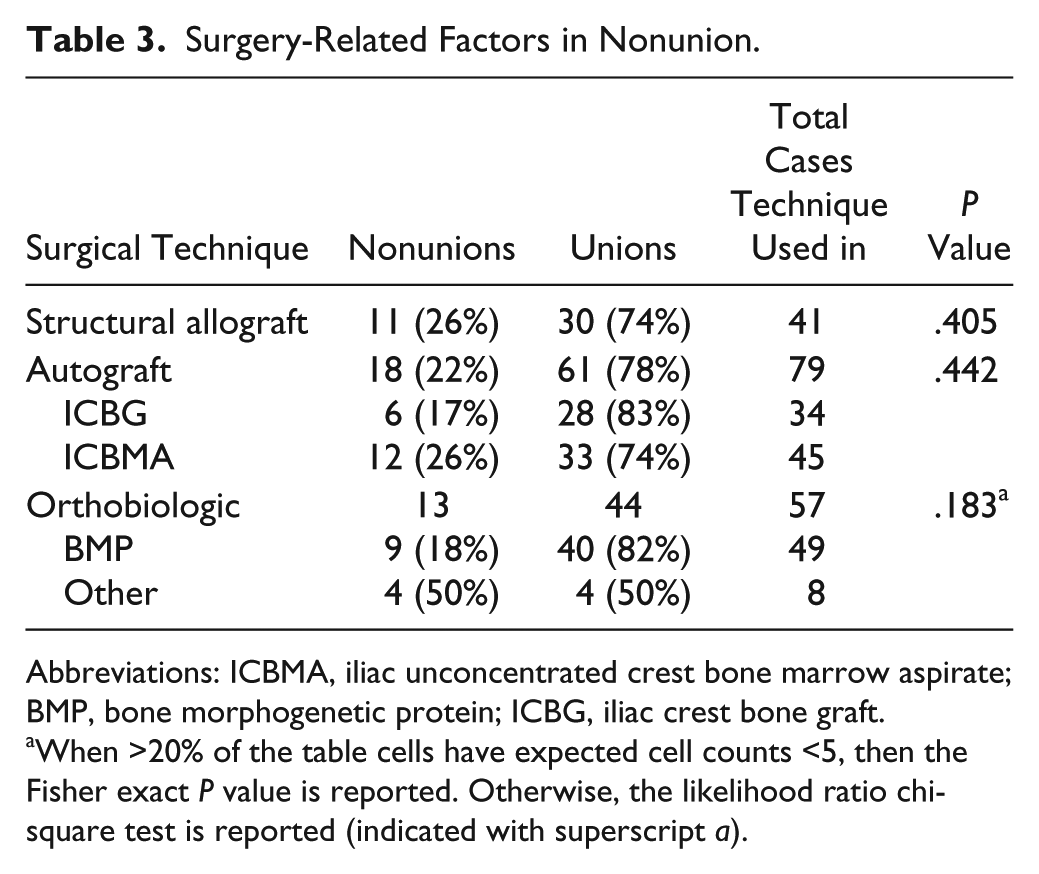
Abbreviations: ICBMA, iliac unconcentrated crest bone marrow aspirate; BMP, bone morphogenetic protein; ICBG, iliac crest bone graft.
When >20% of the table cells have expected cell counts <5, then the Fisher exact P value is reported. Otherwise, the likelihood ratio chi-square test is reported (indicated with superscript a).
Attempts at Prior Revision Surgery.
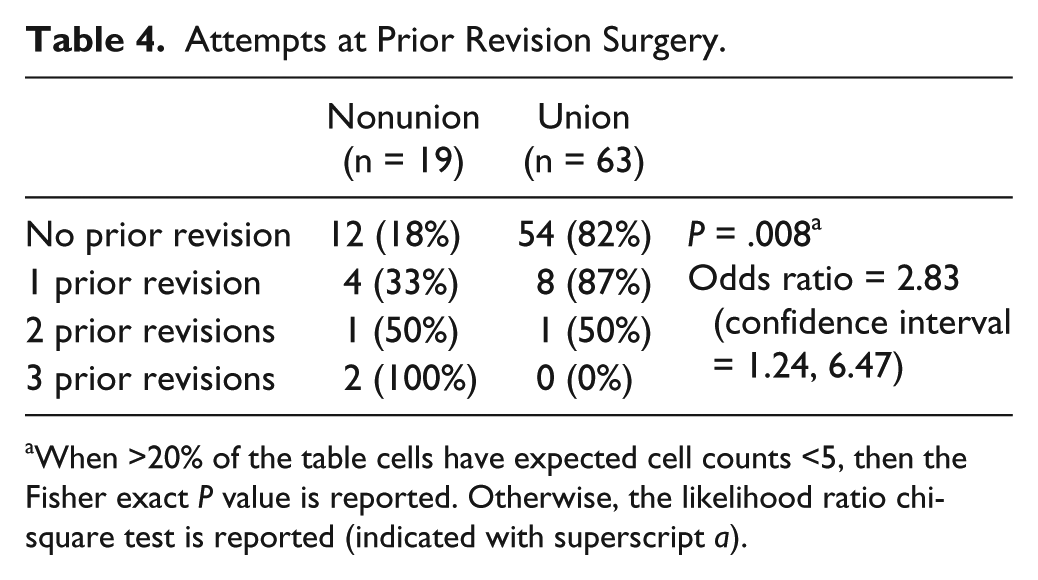
When >20% of the table cells have expected cell counts <5, then the Fisher exact P value is reported. Otherwise, the likelihood ratio chi-square test is reported (indicated with superscript a).
Location of Nonunion.
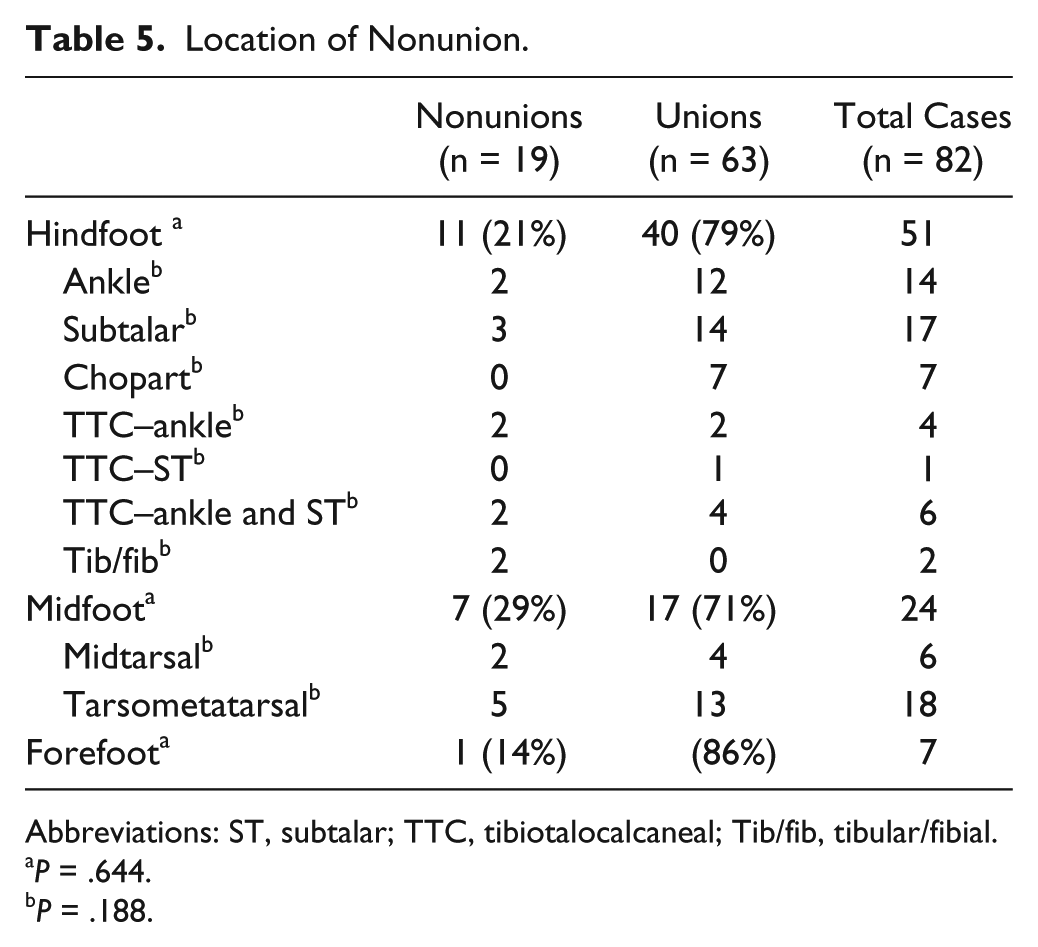
Abbreviations: ST, subtalar; TTC, tibiotalocalcaneal; Tib/fib, tibular/fibial.
P = .644.
P = .188.
Patient-Specific Factors
Of the patient-specific factors studied in this group, neuropathy was identified as a significant risk factor for nonunion (P = .005) in a univariate analysis (Table 2). Diabetes, smoking, inflammatory arthropathy, and posttraumatic arthritis did not influence the risk for nonunion after revision arthrodesis. Charcot arthropathy did not reach significance at P = .051, but the analysis was limited to only 2 patients presenting with this condition.
Surgery-Specific Factors
Surgery-specific factors such as the use of structural allograft (41 patients), CA (34 patients), nonconcentrated ICBMA (45 patients), and orthobiologics (57 patients) (Table 3). CA was primarily iliac crest bone graft (30 patients), with 4 subjects harvested from either the calcaneus or distal tibia. CA was not found to have a significant effect on fusion rates. Orthobiologics included primarily BMP (49 subjects), and “others” including demineralized bone matrix, Ignite, and AlloStem (8 subjects). Univariate analysis was performed evaluating BMP independently and “other” orthobiologics on their own. In both analyses, no statistically significant differences in the rates of nonunion were identified. All subjects were revised using internal fixation, including screws, plate and screw constructs, and intramedullary nailing. Because of the large variation in fixation methods, no statistical analysis was performed.
Prior Revision Attempts
Twenty percent of patients in this study had a previous revision surgery for a nonunion at the operative site (Table 4). Previous revision attempts at the same site were identified as a significant risk factor for nonunion (P = .008). The odds ratio for a nonunion after prior operative treatment for a nonunion was 2.83 (1.24-6.47).
Location of Nonunion
Evaluation of nonunion location was performed by assessing overall foot location (ie, ankle /hindfoot, midfoot or forefoot) and in subgroup analysis looking specifically at each joint (ie, ankle, subtalar, tarsometatarsal, etc) (Table 5). In evaluation of location of the initial nonunion, we did not identify a correlation with persistent nonunion by either region or specific location with the numbers available.
Discussion
Nonunion after arthrodesis procedures is a concern for any foot and ankle surgeon. The rate of nonunion is variable, with many contributing factors reported in the literature. Although nonunions are commonly seen across the spectrum of foot and ankle arthrodeses, the occurrence in specific locations vary, resulting in a deficiency in the literature regarding the management of a nonunion and success rate of attempted revision. This series of 82 patients undergoing revision arthrodesis is the largest case series assessing revision arthrodesis in the literature to our knowledge. This population included all subjects regardless of medical comorbidities and assessed revision fusion rates at all levels of the foot and ankle.
The overall nonunion rate after revision arthrodesis in this case series was 23%. Previously, a small number of case series have investigated the results of revision arthrodesis, primarily at the ankle joint. Midis et al 21 reported on 10 cases of revision ankle arthrodesis for aseptic nonunion using an external fixator, bone grafting, and implantable bone stimulator. These authors found a 100% success rate in this small patient group. Similarly, Katsenis et al 15 reported a 100% success rate in 21 revision ankle arthrodeses using the Ilizarov technique. Midis et al 21 included only 1 patient with diabetes, and no patients had neuropathy, history of infection, or a previous revision attempt. In addition, the use of a bone stimulator and external fixation are operative factors not amenable to the treatment of some nonunions and was not studied in our group of patients, but are factors that may contribute to the rate of union. In our study group, all patients were revised from internal fixation to internal fixation, and 20% of patients had undergone prior revision attempts, which may account for the variation in results. Anderson et al 1 were able to obtain a fusion rate of 85% in cases for nonunion and malunion at the ankle using internal compression screws, although 12 patients required 19 additional surgeries to obtain these results. Similarly, Levine et al 18 reported a union rate of 91% in 23 ankle fusions treated with internal fixation for revision arthrodesis at 14 weeks. Overall, 86% (12/14) of ankle arthrodeses in our series went on to union, a value slightly lower than those reported for primary ankle arthrodesis. 7
Our univariate analysis identified that multiple attempts at revision arthrodesis was a significant risk factor for persistent nonunion after revision surgery. Of the 15 subjects who had previous attempts at revision surgery, only 8 (53%) went on to union after revision at our institution. Although little is written about revision arthrodesis, there is no literature investigating outcomes in cases of multiple nonunion revisions. The best source of literature evaluating persistent nonunion comes from the management of fracture nonunion. Taormina et al 29 found that in the management of long bone fractures, smoking and prior nonunion surgery were the only statistically significant reasons for delay in healing and poor outcomes after revision surgery. In this study, we found that when revising a nonunion of a primary arthrodesis, the risk of nonunion increased by a factor of 3 (odds ratio 2.83). In addition, if the revision attempt resulted in nonunion, the next revision surgery had a further increase in the risk of nonunion (compared to the previous revision surgery) by a factor of 3. The increased risk of nonunion with each revision is likely multifactorial, including both patient-specific factors and decreased capacity for bone healing after multiple surgeries and local vascular compromise with repetitive soft tissue stripping of the bone.
Patients with neuropathy (12) had a statistically significant nonunion rate of 58% (7). Patients with diabetes had a nonunion rate of 25% (2/8) that did not prove to be statistically significant. In our study, 2 subjects undergoing reconstruction for a nonunion with associated Charcot neuropathic arthropathy went on to nonunion but because of the small sample size, we were not able to prove significance (P = .051). In this cohort of patients, not all neuropathic patients had diabetes, in fact many of these patients were identified with idiopathic neuropathy. Previous reports are suggestive that diabetes and/or neuropathy are risk factors in foot and ankle surgery. Whether neuropathy, with or without diabetes mellitus, is a risk factor is unclear. As reported by other authors, patients with idiopathic neuropathy present with a wide variety of abnormalities and often need treatment of their musculoskeletal problem similar to those with diabetes.2,16
Other factors have been investigated related to the risk for developing nonunions in the setting of primary fusion. Recently, a nonunion risk assessment model was developed to identify “total nonunion risk” in foot and ankle surgery. 30 In this model, smoking, diabetes, obesity, poor vascularity, soft tissue compromise, operative site instability, and multiple other factors were used to calculate nonunion risks. In our study, we looked at many of the same patient factors, yet found that many did not increase the patient’s overall risk for nonunion in the setting of revision surgery (Table 2).
In this study group, we identified subjects with a history of infection or compromised wound healing during the index procedure but did not find that this was associated with an increased risk of nonunion. For the purposes of this study, a history of infection was defined as any patient who reported having a history of “wound complications” or “multiple courses of antibiotics” noted in their medical records, the need for postoperative irrigation or documented positive culture results. This identified 11 subjects, of which 7 went on to heal. This broad definition of infection may have resulted in more subjects identified than truly had an infection that would increase the patient’s risk. Perlman et al 23 found that primary ankle arthrodesis in patients with history of open trauma has a nonunion rate of 53%, compared to 28% overall nonunion rate in patients with posttraumatic ankle arthritis. Although this study did not clearly define the grade of open injury, there may be a more significant relationship between exposure to possible infection and the success of arthrodesis procedures. Fracture literature has reported rates of union in infected long bone nonunion from 84% to 97% using a variety of techniques, although it is unclear whether we can accurately compare fracture nonunion to arthrodesis nonunion. 5
There have been multiple studies linking smoking to nonunion in the foot and ankle as well as fracture healing.14,26 A recent systematic review found that the odds ratio for fracture nonunion in smokers was 2.3 times higher than nonsmokers. 26 Smoking was not found to impact the likelihood of successful revision arthrodesis in this patient group; however, the impact of smoking in our study may not be fully appreciated because of the small sample size.
A 23% nonunion rate during revision arthrodesis was identified in this study, which is consistently higher than most values reported in the literature for primary arthrodesis. The highest rate of nonunion was found in the midfoot with 29% (7/24), followed by ankle/hindfoot 21% (11/51) and forefoot 14% (1/7). However, these rates of nonunion by site did not prove to be statistically significant. The rate of nonunion in primary first metatarsophalangeal joint fusion has been reported to be 5.4%, and first tarsometatarsal nonunions similarly 5% in recent systematic reviews.9,25 Ankle nonunion rates have been reported to be as low as 9% in primary uncomplicated open ankle fusion. 7 Other literature has shown nonunion rates to be as high as 47% in foot and ankle arthrodesis frequently associated with various medical comorbidities.22,23 In all of these studies, the numbers are based on nonunion following primary arthrodesis. This study demonstrated that the location of the nonunion did not have an effect on overall success rate. Although certain joints may carry an increased risk of nonunion after primary arthrodesis surgery, the success of a revision does not seem to be dependent on operative site.
The use of bone graft is common in managing nonunions, as a recent study found that 96% of foot surgeons almost always or always use bone grafting during nonunion surgery. 3 In this study, almost every patient had either nonconcentrated ICBMA mixed with either a finely ground allograft powder (54%) or autograft cancellous bone (41%) used during the revision procedure. Osteoprogenitor cells have been found in aspirate from the tibia, calcaneus, and iliac crest in varying quantities, 13 though currently no significant data have been reported on fusion rates with the use of bone marrow aspirate in foot and ankle fusion. 10 In addition, no studies to date compare the use of nonconcentrated ICBMA to ICBG in the outcomes of arthrodesis surgery.
In this cohort, various-sized tricortical iliac crest bone allograft wedges were used for structural support, deformity correction, or bone augmentation in 41 cases. There was no increase in the rate of nonunion (26%) when structural allografts were used. Successful use of allograft has been described for managing high-risk patient populations previously in multiple joints in the foot, and even in the setting of revision first metatarsophalangeal joint arthrodesis.17,19 Our findings are consistent with reports that the use of structural allograft does not increase the risk of nonunion in arthrodesis procedures.
In this patient cohort, orthobiologics were used in 69% of operative procedures. Specifically, BMP was used in 59% (49) of revisions. Other orthobiologics included various demineralized bone matrix (DBM) products. The rates of nonunion in those patients where BMP was utilized (18%) did not differ from those cases where BMP was not used (23%). The use of any orthobiologics did not impact the rate of fusion in these revision cases. These findings are similar to a recent retrospective study assessing the use of iliac crest bone graft with and without BMP in fracture nonunion. These authors did not find any significant improvement in healing rates as both were found to be higher than 95%. 28 In our study, group BMP was used in combination with both ICBG, ICBMA, and allograft bone graft, which may make interpretation of the results more difficult. Multiple studies have found no difference between use of BMP and ICBG in revision nonunions for long bone fractures whereas other reports have shown that BMP use in the foot and ankle has high rates of successful primary fusion (92%) in high-risk patient arthrodesis and fracture nonunion repair, though no controls were used for comparison. 32 In a small number of patients, other orthobiologics, such as DBM and AlloStem, were used and found to have a lower, though not statistically significant, rate of healing (50%). Because of the small sample size, it is unclear if these alternate orthobiologic agents contributed to healing. However, the lower rate of healing in this subgroup is not expected. Thordarson et al 31 found that the use of DBM did not affect the rates of fusion in the ankle or hindfoot compared with historical controls, making it unclear why this small cohort of patients appeared to heal at a lower rate than others.
There are several limitations to this study. The wide variety of nonunion location, treatment methods, and patient variables make it very difficult to compare subjects. The retrospective design does not allow conclusions to be made about the best practice for management of nonunions. In our study, outcomes were based on radiographic results of nonunion surgery, not the clinical outcomes of each procedure. Although this is the largest case series of subjects undergoing revision arthrodesis in the foot and ankle, there were relatively low numbers of subjects with persistent nonunion. There was a small prevalence for the presence of key potential predictors of nonunion in this patient cohort. Prevalence for the presence of diabetes, history of infection, and history of smoking ranged from 10% to 15%. With this small prevalence of important patient subgroups, the study had adequate statistical power (ie, 80%) to detect only large between-group differences in nonunion rates; differences ranging from 44% to 49%. In our patient cohort, the observed between-group differences in nonunion rates for these predictors were substantially less and ranged from 2% to 15%. For these predictors, nonsignificant results may be due to inadequate sample size and an associated lack of statistical power.
In addition, metabolic parameters such as vitamin D levels were not taken into account during the time frame of this study. It has been established that vitamin D deficiency exists in a high percentage of patients presenting with foot and ankle injury and even in groups of patients presenting for elective foot or ankle surgery.20,27 Although some data exist suggesting that vitamin D deficiency may play a role in nonunion of fractures, the role of vitamin D in arthrodesis nonunion has not been studied. 6 In a prospective, randomized study of proximal humerus fractures, Doetsch et al showed improved fracture callus formation in a group of patients treated with vitamin D3. 8 Further study is required to identify the relation between calcium metabolism and vitamin D and healing in arthrodesis of the foot and ankle.
However, one factor is clear, the risk of nonunion with subsequent revision surgery increases with each attempt at revision. This is an important factor in counseling patients regarding their unique risk with a revision arthrodesis. After more than one attempt to revise a nonunion, further revision surgery becomes an endeavor with a very low likelihood of success. Attempts to revise a joint in these circumstances may primarily be performed with a goal of increased stability or decreased deformity without an expectation of radiographic fusion. Patients should be counseled carefully that a history of nonunion places them in a group with a unique risk factor. In addition, this study further emphasizes the critical role that neuropathy plays in complications after foot and ankle surgery.
Future studies evaluating the outcomes of nonunions may benefit from a focus on clinical outcomes to determine if there is a functional value to revision surgery. In addition, prospective studies with uniformity in the use of arthrodesis adjuncts, may allow us to better understand their role in management of nonunions. Larger cohorts of retrospective studies may help us better identify risk factors for nonunion. At a cost of $11 300 for fracture nonunion revisions, determining the most successful means of obtaining a successful fusion would be beneficial. 11
Conclusion
Revision arthrodesis for nonunion in the foot and ankle was successful (77%) under a variety of patient and operative conditions. Neuropathy was a significant patient risk factor for persistent nonunion and we believe is important to identify even in the nondiabetic patient. As the number of attempts at revisions increased, there was a subsequent 3-fold increase in the rate of persistent nonunion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Washington University acknowledges OMeGA Medical Grants Association and the support of Zimmer, DePuy Synthes, and Biomet Orthopedics for their generous Foot & Ankle Fellowship Grant.