
Abstract
Background:
Large cystic osteochondral defects of the talus can be challenging to treat. This retrospective control study looked at the use of osteochondral autograft transfer combined with cancellous allograft in patients with advanced cartilage and subchondral bone damage of the talus.
Methods:
Thirteen patients were treated with large cystic osteochondral defect of the talus between February 2010 and July 2013. All of these cystic osteochondral defects were larger than 15 mm in diameter. The subchondral defects were filled with cancellous allograft and the center of the lesions were sealed with an osteochondral cylinder autograft that was harvested from the ipsilateral medial femoral condyle. The visual analog scale (VAS) score for pain during daily activities, American Orthopaedic Foot & Ankle Society Ankle and Hindfoot (AOFAS-AH) scores and subjective satisfaction survey rating were obtained. Plain radiographs and magnetic resonance imaging of the ankle were obtained before and after surgery. In 5 cases, arthroscopy was performed 12 months postoperatively, and the cartilage repair was assessed with the criteria of the International Cartilage Repair Society. Twelve patients were available for follow-up at a mean of 25.4 months (range, 18 to 48 months).
Results:
Average postoperative AOFAS-AH score 12 months after surgery was 88±7 compared with 64±10 preoperatively. The mean VAS score decreased from 6±1 preoperatively to 1±1 at the latest follow-up. Seven patients rated their result as excellent, 5 as good and none as fair. The radiolucent area of the cysts disappeared on the plain radiographs in all cases. The mean International Cartilage Repair Society arthroscopic score from follow-up arthroscopy was 9±1 points.
Conclusions:
The use of osteochondral autograft transfer combined with cancellous allograft was an effective option for the treatment of large cystic talar osteochondral lesions.
Level of Evidence:
Level IV, retrospective case series.
Osteochondral lesions of the talus (OLTs) were described as early as 1922. 17 These lesions involve the talar articular cartilage and subchondral bone, which are relatively common injuries in patients with chronic disabling pain after ankle sprains.1,7,8,10,12,13,26 Previous trauma is reported as the main cause of OLTs in lateral lesions (93%-98%) and less so in medial lesions (61%-70%).3,15,31
The OLTs were classified first 5 in 1959: stage 1, small area of subchondral bone compression; stage 2, partly detached osteochondral fragment; stage 3, completely detached, but undisplaced, osteochondral fragment; stage 4, displaced osteochondral fragment. Two authors 28 found that large cysts were occasionally seen below the talar articular defects. They categorized this kind of talar cysts as a type V lesion in 2001. Nonoperative treatment fails frequently.10,12,13,26 Common operative treatment methods include debridement and microfracturing, osteochondral autograft transfer system and mosaicplasty, autologous chondrocyte transplantation, autologous chondrocyte implantation, and bulk allograft transplantation. *
The cystic lesions (type V) require different treatment from the other types of OLTs. Because of the presence of a structural defect, the shaving or drilling procedure alone often does not work well. Antegrade or retrograde bone grafting may fill the defect, but the injured articular surface remains unhealed and may cause further problems. 27 The operative treatment is even more challenging when the cystic lesion of the talus is larger than 15 mm in diameter. Sometimes joint-sacrificing surgery such as arthrodesis or total ankle arthroplasty is performed. The joint-preserving surgeries include osteochondral autografts, allografts, or autologous chondrocyte implantation. 32 Large cystic lesions may not be amenable to osteochondral autograft alone because of unacceptable donor site morbidity with harvesting high-volume areas of cartilage from the knee. Allografts avoid donor site morbidity. But the relatively poor chondrocyte viability has limited its widespread clinical application. Autologous chondrocyte implantation has only recently been applied for osteochondral lesions of the ankle. 12 However, the lack of generally agreed-on operative guidelines and a paucity of quality comparative studies have led to continued controversy regarding the utility of this technique. 22
Osteochondral autograft transfer combined with cancellous allograft may fill the talar defect as well as seal the damage of the cartilage at the top of the talus. The purpose of this study was to report our experience in treating patients with large cystic osteochondral defects of the talus, determine the functional scores, patients’ satisfaction, and radiologic results.
Methods
Thirteen patients with unilateral large cystic osteochondral defects of the talus underwent osteochondral autograft and cancellous allograft transfer between February 2010 and July 2013. There were 5 women and 8 men, with a mean age of 40.5 years (range, 34-60 years). Each patient had a history of severe ankle sprain from once to several times. Their main symptoms were pain (100%), ankle instability (38%), and stiffness (15%). All patients failed nonoperative treatment, including nonsteroidal anti-inflammatory medication and physical therapy. According to the preoperative imaging evaluation (plain radiographs and computed tomographic [CT] scan), all of these patients were diagnosed with osteochondral lesion of the talus with large subchondral cysts. All these cystic osteochondral defects were larger than 15 mm in diameter.
Clinical examination of the ankle joint included range of motion, sagittal and inversion/eversion stability, location of tenderness, and alignment of the hindfoot. Five of the 13 patients had mild stiffness of their involved ankle. There were 4 ankles with mild laxity on the anterior drawer test, but the patients did not have clear symptoms of instability, so no lateral ligament repair was planned.
Initial diagnostic imaging of the foot and ankle consisted of plain radiographs (weightbearing anteroposterior/lateral radiographs, and the hindfoot alignment view [Saltzman view]) to assess alignment and exclude other pathologies other than OLT. Mortise and talar neck view (Canale view) were taken to show the talar dome. 13 Magnetic resonance imaging (MRI) was performed to determine the condition of the cartilage and accompanying soft tissue pathology. 4 CT scan assessed the extent of the bony lesion accurately. All these patients received both CT and MRI examination.
Four lesions involved the right ankle, and 9 lesions involved the left ankle. All the cystic osteochondral lesions were located at the medial side of the talus. The cystic osteochondral lesion was 19 mm long, 15 mm wide, and 15 mm deep (mean volume 34 275 mm3; range: length, 15-25 mm; width, 10-20 mm; height, 9-28 mm). None of the roofs of these cystic lesions were intact (articular surface of the talar dome and the subchondral bone were injured). No other pathology was found on imaging such as tendinopathy. Twelve patients were available for follow-up at a mean of 25.4 months (range, 18-48 months). One patient was lost to follow-up 3 months after surgery as a result of inconvenient communication and transportation.
The visual analog scale (VAS) score for pain during daily activities and American Orthopaedic Foot & Ankle Society Ankle and Hindfoot (AOFAS-AH) scores 18 were recorded before and after surgery. A subjective satisfaction survey rating was obtained 1 year after surgery. Plain radiographs were taken at every follow-up until evidence of bone healing. MRI of the ankle was obtained before and 1 year after surgery. Arthroscopy was performed 12 months postoperatively in 5 patients. The cartilage repair was assessed with the criteria of the International Cartilage Repair Society 30 (12 points: normal, 11-8: nearly normal, 7-4: abnormal, 3-1: severely abnormal). The institutional review board (IRB) approval of this study was obtained from the ethics committee of our hospital.
Operative Technique
The patient was positioned supine with no bump under the ipsilateral hip in order to allow easy external rotation of the leg intraoperatively. The patient received general anesthesia, and a thigh tourniquet was used. The longitudinal skin incision was 1 cm anterior to the center of the medial malleolus, starting 5 cm proximal to the tip of the malleolus and extending distally for approximately 7 cm. A medial malleolar osteotomy was performed from approximately 5 cm above the tip of the medial malleolus and extended to the lateral margin of the talar lesion with a microoscillating saw. The defect in the overlying cartilage was easily identified, and a small curette was used to unroof the cyst and remove the intracystic gelatinous material. The wall and base of the lesion were abraded and curetted down to viable subchondral bone. After the debridement, the lesions often looked like a jar. Allograft cancellous bone was used to fill the defect first. Then cylindrical autologous osteochondral plugs taken from the ipsilateral medial femoral condyle were inserted into the defect to resurface the articular cartilage. Cannulated screws were introduced to stabilize the osteotomy. Fluoroscopic images (anteroposterior, lateral, and mortise) were obtained (Figure 1).
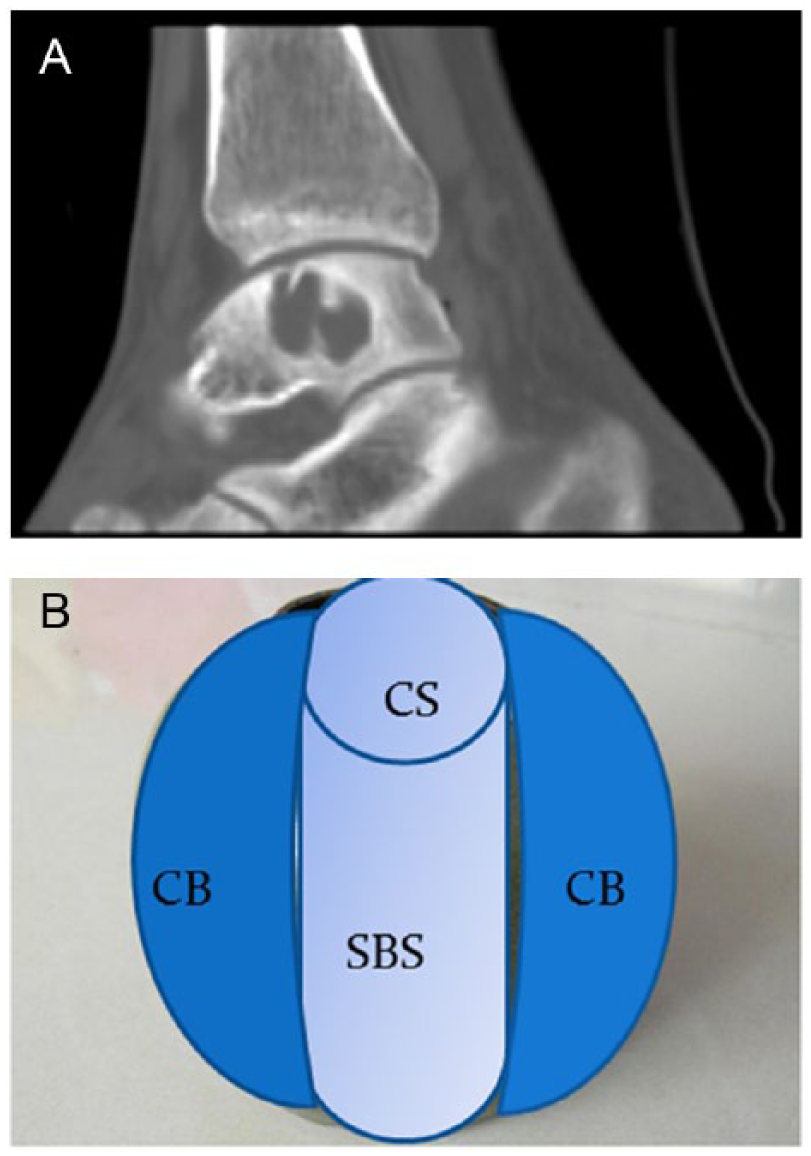
The shape of the cystic lesion and the schematic diagram of the procedure. (A) The cyst is larger than the chondral surface defect which is on the top of it. (B) Schematic diagram of a hybrid method filling with osteochondral autograft at the center and the roof of the lesion, and cancellous allografts around the autograft. CB, cancellous bone graft; CS, cartilage surface; SBS, subchondral bone cylinder.
Postoperative Care
The ankle and knee were wrapped in a bulky bandage for 2 weeks. Passive range of motion (ROM) of the ankle and knee joint began at 2 weeks after operation. A posterior splint was changed to a boot 2 weeks after surgery. At 6 weeks, the patient was encouraged to partial weight-bear and perform ROM of the ankle. Full weight bearing began after the radiographs showed enough evidence of bone healing at about 8 weeks. Return to sports was after 6 months. The patients were seen in the outpatient clinic 2, 6, 8, and 12 weeks after the surgery for a clinical follow-up examination and conventional radiographs. After that, the clinic follow-ups were every 3 months.
Data Analysis
Statistical analysis was performed using the Student t test to determine if there were significant changes in the preoperative and postoperative VAS and AOFAS scores. The significance level was set at P <.05.
Results
All the osteotomies healed at an average time of 8 weeks. The mean VAS score decreased markedly by the latest follow-up. All the patients were satisfied with the results of pain relief. Average postoperative AOFAS-AH score 12 months after surgery was increased compared with that preoperatively. Ten patients gained normal range of motion of their ankle and hindfoot at the latest follow-up. Two patients had mild stiffness of the ankle. All of the patients returned to work at the latest 6 months after surgery. Six of the 12 patients returned to low-impact competitive sports. Seven patients rated the result as excellent, 5 as good, and none as fair (Tables 1 and 2).
Demographics and Clinical Data of Patients Who Had Osteochondral Lesions of the Talus Treated With Osteochondral Autograft and Cancellous Allograft.
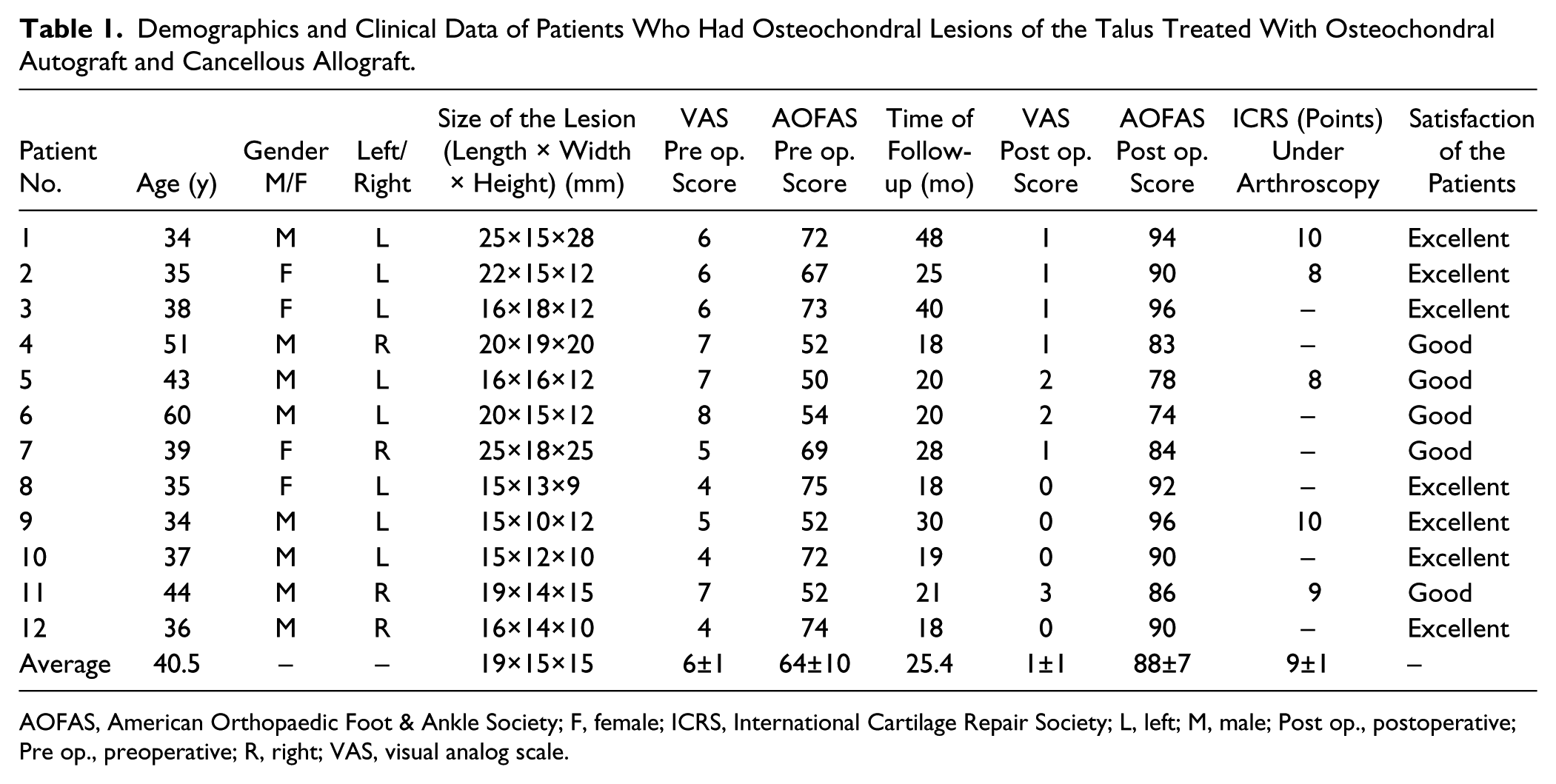
AOFAS, American Orthopaedic Foot & Ankle Society; F, female; ICRS, International Cartilage Repair Society; L, left; M, male; Post op., postoperative; Pre op., preoperative; R, right; VAS, visual analog scale.
VAS and AOFAS Scores Before and After the Surgeries of Patients Who Had Osteochondral Lesions of the Talus Treated With Osteochondral Autograft and Cancellous Allograft.
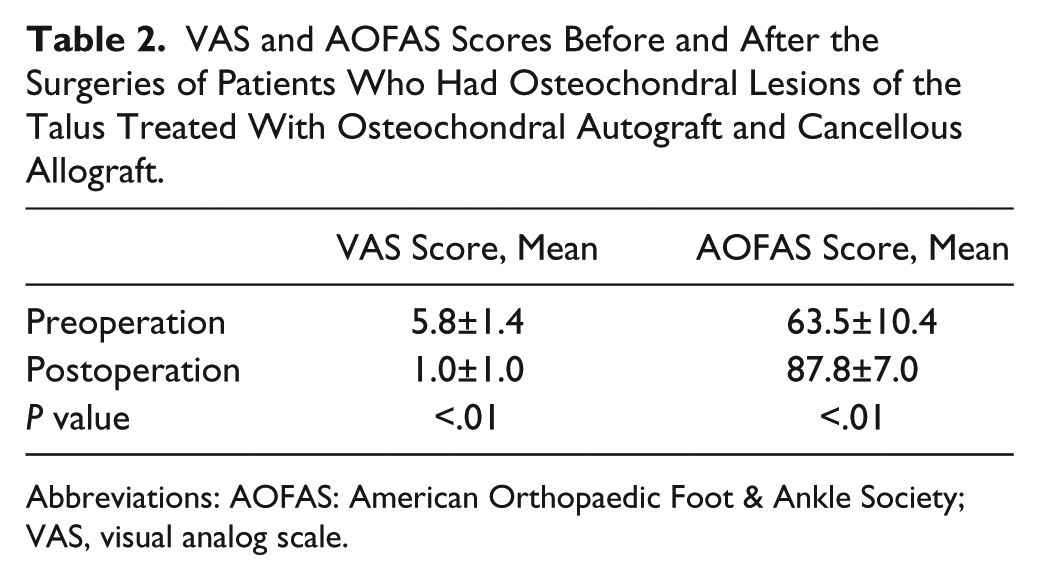
Abbreviations: AOFAS: American Orthopaedic Foot & Ankle Society; VAS, visual analog scale.
The radiolucent area of the cysts disappeared on the plain radiographs in all cases from immediately after the surgery up to the latest follow-up. Every patient received CT and MRI scan 1 year after surgery and the radiographic results were compared with those before surgery. The follow-up CT scan showed that the grafts were well consolidated with the subchondral bone. The MRI results showed that the cartilage surface of the reconstructed site was smooth and congruent. Neither edema nor degenerative articular change could be found at the follow-up MRI (Figure 2).
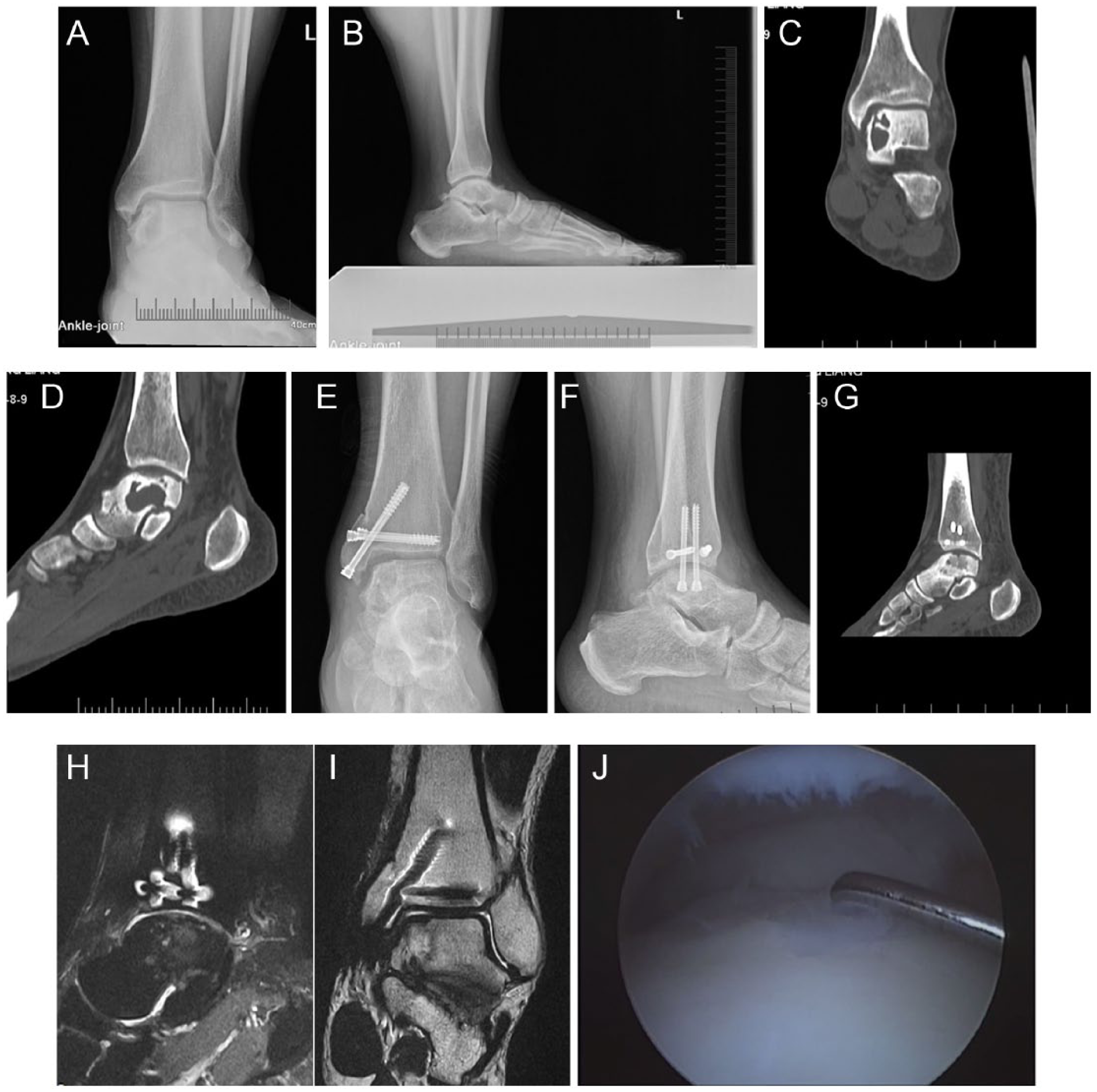
Large cystic talar lesion case, receiving the surgery of osteochondral autograft transfer combined with cancellous allografts. A 34-year-old male patient complained of intermittent ankle pain, mild swelling, and stiffness. He had to quit playing soccer, which he used to play once a week. (A and B) A large radiolucent area can be found at the medial side of the subchondral bone of the talus on his left ankle from the plain radiograph image. (C and D) A large cystic osteochondral lesion of the talus can be found. Part of the cartilage was involved. (E and F) Osteochondral autograft transfer combined with cancellous allografts was used to treat this patient. The medial malleolar osteotomy was performed to expose the lesion and secured by screws. (G) CT scan 8 weeks after surgery showed the defect had been well filled with grafts. (H and I) MRI evaluation 1 year after surgery showed that the cartilage surface was congruent and smooth, and the grafts were well consolidated with the subchondral bone around. No edema sign can be found. (J) Arthroscopy was performed to evaluate the cartilage directly. The cartilage looked and felt stable, firm, and consolidated.
Five patients requested hardware removal for cultural reasons although none of them had symptoms. They received the second surgery from 12 to 18 months after the previous surgery. The hardware was removed and at the same time an arthroscopy was performed with the permission of these patients. The mean International Cartilage Repair Society arthroscopic score from follow-up arthroscopy represented near normal cartilage (Tables 1 and 2, Figure 2).
The donor site morbidity of the knee was followed. International Knee Documentation Committee (IKDC) score and Lysholm score were used to evaluate the knee at 6, 12, and 18 months after the surgery. 20 The patients did complain of knee pain at 6 months, but the pain diminished gradually by 12 months after surgery. At the follow-up of 18 months after surgery, no patients had knee complains.
Discussion
The present results showed that outcomes of patients who had large cystic lesions of the talus with cartilage damage were improved after treatment with osteochondral autograft transfer combined with cancellous allograft. The cyst was always larger than the chondral surface defect both in coronal and sagittal view. This made the “hybrid” graft treatment possible. After the wall and base of the cystic lesion were abraded and curetted down to viable subchondral bone, allograft cancellous bone was used to fill the defect. Then cylindrical autologous osteochondral plugs harvested from the ipsilateral medial femoral condyle were inserted into the center of the defect to resurface the articular cartilage. With this method, the defect of the subchondral bone was well filled with grafts, and the roof of the lesion was sealed with autograft cartilage. Only one or two 8-mm-diameter osteochondral autograft cylinders was harvested from the nonweightbearing region of medial femoral epicondyle. The donor site morbidity was minimal. The radiolucent area of the cysts disappeared on the plain radiographs in all 12 cases at the 1-year follow-up. The CT scan and the MRI also showed that the cystic lesions were filled with bone.
The talar articular cartilage of these cases were reevaluated with MRI 1 year after the surgery. From this evaluation, the cartilage surfaces were found congruent and smooth. Arthroscopy was performed in 5 patients from 12 to 18 months after the surgery. The transferred cartilage appeared stable, firm, and consolidated with the cartilage around them.
Osteochondral autograft transplantation 21 involves transferring an osteochondral graft from a nonweightbearing region to the chondral defect. 27 The main drawback for osteochondral autograft transplantation is donor site morbidity. 24 According to the literature, the donor site can be on the medial side of femoral epicondyle, 19 lateral side of femoral epicondyle, 2 and the intercondylar notch. 24 To our knowledge, studies on the outcomes of these 3 donor sites cannot be found. One investigation showed that there was generally lower pressure on the medial aspect of the trochlea than the lateral side. 9 Some authors have reported that the patella translates and tilts laterally relatively to the femur during knee flexion. 6 The osteochondral autograft cylinder was harvested from the medial side instead of lateral side of the femoral epicondyle in this study. The authors believe that the donor site from the medial side of the epicondyle may have less impact on the knee. The limited amount of osteochondral graft harvested from the knee (1 or at most 2 cylinders) also reduced the risk of donor site morbidity.
The limitations of this study were the retrospective design without control group, and the small number of cases. Although osteochondral lesions of the talus are encountered frequently in clinical practice, the OLTs with large cysts are not as common. Knee cartilage does not have the same biomechanical properties as ankle cartilage, so long-term follow-up is needed. The AOFAS score has been widely used to evaluate OLTs in the literature, but it is not a validated scale. We tried to evaluate the results more comprehensively by adding the VAS score, arthroscopic score, and radiographic results including plain films, CT scan, and MRI.
In conclusion, the use of osteochondral autograft transfer combined with cancellous allograft was an effective option for pain relief and functional improvement with return to low-impact sports for treatment of large cystic talar osteochondral lesions. This joint-preserving procedure had good bone consolidation as well as good articular resurfacing. The reconstructed cartilage was from the patient’s own body. Allograft cancellous bone and autograft osteochondral plugs were used together to minimize the amount of autograft so donor site morbidity was reduced to a minimum.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China (grant 81272051).