
Abstract
Background:
Isolated lateral malleolar fractures may result from a supination-external rotation (SER) injury of the ankle. Stable fractures maintain tibiotalar congruence due to competent medial restraints and can be treated nonoperatively with excellent functional results and long-term prognosis. Stability might be assessed with either stress radiographs or weightbearing radiographs.
Methods:
A consecutive series of patients with closed SER fractures (presumed AO 44-B1) were prospectively enrolled from 2008 to 2015. Patients with clearly unstable fractures (medial clear space more than 7 mm) on the initial nonweightbearing radiograph were excluded and operated on. All other patients were examined with a gravity stress and a weightbearing anteroposterior radiograph. Borderline instability of the fracture was assumed when the medial clear space was 4 to 7 mm. Those were treated nonoperatively.
Results:
Of 104 patients with isolated lateral malleolar fractures of the SER type, 14 patients were treated operatively because of clear instability (displacement) on the initial radiographs. Of the nonoperative patients, 44 patients demonstrated borderline instability on the gravity stress but stability on the weightbearing radiograph (“gravity borderline”); the remaining 46 were stable in both tests (“gravity stable”). At an average follow-up of 23 months, no significant differences were seen in the American Orthopaedic Foot & Ankle Society hindfoot score (92 points gravity-borderline group vs 93 points gravity-unstable group), the Foot Functional Index score (11 vs 10 points), the Short Form 36 (SF-36) physical component (86 vs 85 points), and SF-36 mental component (84 vs 81 points). Radiographically, all fractures had healed with anatomic congruity of the ankle.
Conclusion:
Weightbearing radiographs provided a reliable basis to decide about stability and nonoperative treatment in isolated lateral malleolar fractures of the SER type with excellent clinical and radiographic outcome at short-term follow-up. Gravity stress radiographs appear to overrate the need for operative treatment.
Level of Evidence:
Level III, prospective comparative study
The treatment of isolated lateral malleolar fractures of the supination-external rotation (SER, AO type B) morphology is based on the concept of stability of the fracture.14,19 The deep deltoid ligament is considered an important structure for stability.1,27,28 Its integrity can be assessed with stress radiographs (manual external rotation stress or gravity stress) or with magnetic resonance imaging.5,7,13,15,17,23 Widening of the medial clear space (MCS) or complete rupture of the ligament is assumed to indicate instability, which is usually treated operatively. 23 Weightbearing radiographs of the ankle represent an alternative approach by testing the stability in a more functional fashion. 26 Congruity of the talus to the medial malleolus and tibial plafond is required for stability, and in this case, nonoperative treatment can provide good to excellent results. 26
In addition to the medial ligamentous restraints, dynamic restraints (ie, a postraumatically elevated tension of the posterior tibial muscle) as well as a favorable ankle bony anatomy (ie, a prominent trochlea or a varus alignment of the tibial plafond) may enhance stability. Thus, they might even allow nonoperative treatment of SER type III and IV fractures with torn medial ligaments.
The purpose of this study was to assess the value of gravity stress vs weightbearing radiographs defining SER fracture stability. We hypothesized that weightbearing radiographs alone would be appropriate to determine the stability and therefore the option for nonoperative treatment with good to excellent outcome. Furthermore, the effect of ankle alignment and trochlear shape on the fracture stability was evaluated.
Methods
A consecutive series of 104 patients (64 male and 40 female; mean age 48 years; range, 16-93) with closed isolated lateral malleolar fractures (presumed AO 44-B1, Lauge-Hansen SER type) were prospectively enrolled from September 2008 to August 2015. Two patients with previous hindfoot trauma were excluded, but patients with diabetes mellitus, peripheral neuropathy, or midfoot trauma were included in this study. Of all enrolled patients, 12 (11.5%) patients presented clear lateral subluxation of the talus (lateral edge of talar dome surpassing lateral edge of tibial plafond; medial clear space more than 7 mm) and an unfavorable bony ankle anatomy (valgus alignment of the tibial plafond or nonprominent trochlea) on the initial static nonweightbearing or gravity stress radiographs. These 12 patients were advised to undergo operative fixation (Figure 1). Ninety-two patients (88.5%) were assigned to preliminary nonoperative treatment, and the ankles were immobilized by either a splint or brace. They were instructed to come back for weightbearing radiographs (full body weight equally distributed on both legs, anteroposterior ankle radiograph in 10 degrees of internal rotation) 3 to 10 days after injury. 26 Stability was defined as a medial clear space of less than 4mm. These criteria were used for the gravity stress radiograph and for the weightbearing radiograph. 7 Borderline instability of the fracture was defined as an MCS of 4 to 7 mm.
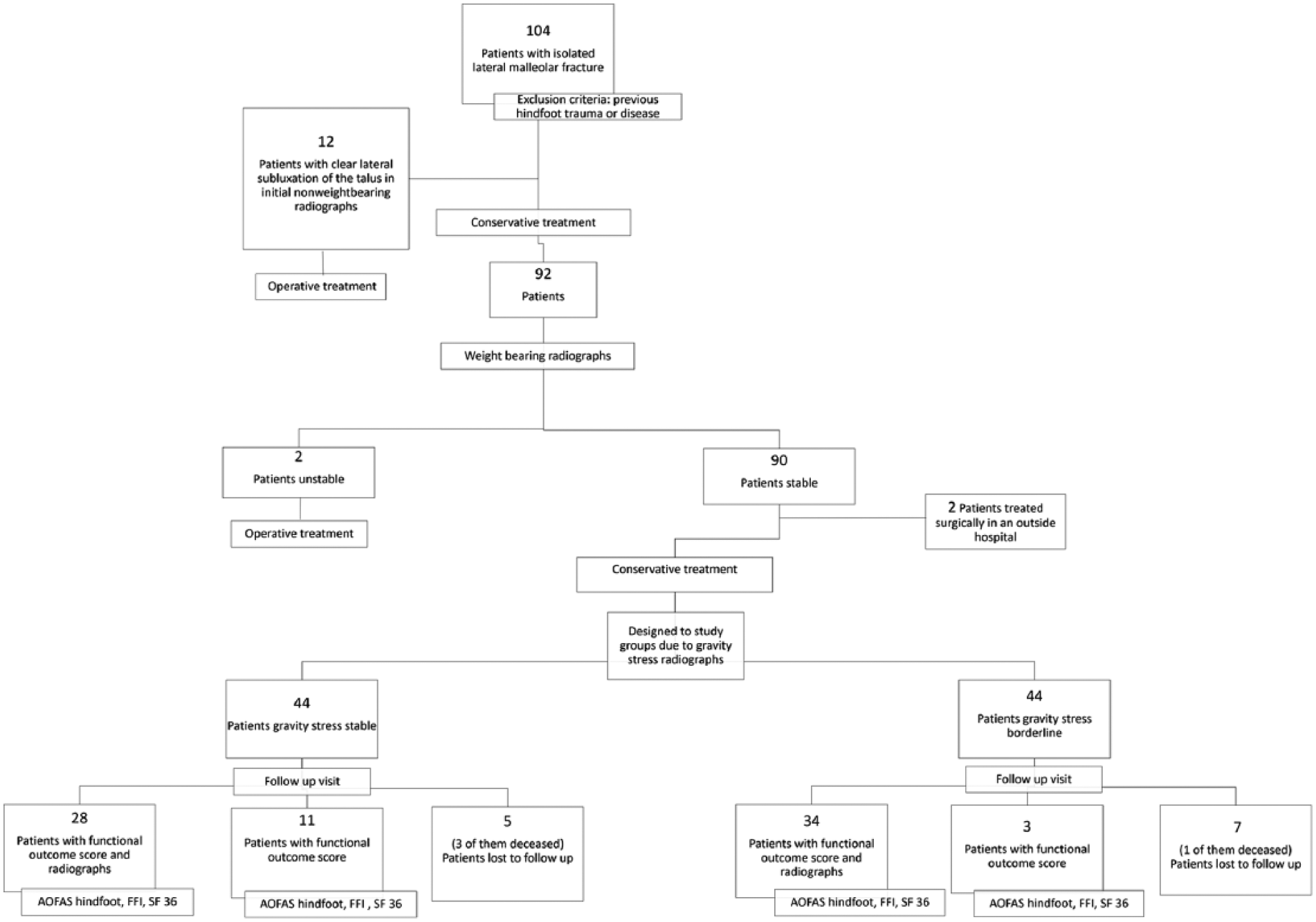
Patient flowchart demonstrating treatment decisions, timetable of the different radiographs, and scores. Finally, in both groups (gravity stable and gravity borderline), 44 patients remained. AOFAS hindfoot, American Orthopaedic Foot & Ankle Society ankle hindfoot score; FFI, Foot Functional Index; SF-36, Short Form 36.
With the weightbearing radiographs, 2 additional patients were identified to fulfill the criteria of major instability and were classified as unstable. The remaining 90 patients were considered borderline or stable and remained in the definitive nonoperative treatment group (Figure 2). These patients were informed they had a stable fracture that allowed unprotected full weightbearing, so there was no need for crutches or a splint. The nonoperative treatment protocol of all patients was the same. If ankle pain was too intense for weightbearing without crutches or bracing, patients were advised to use either or both until pain adequately abated to allow discontinuation of the aids. Only 9 of 90 patients preferred mobilization without a brace or splint. The others used aids for a mean of 27 days.
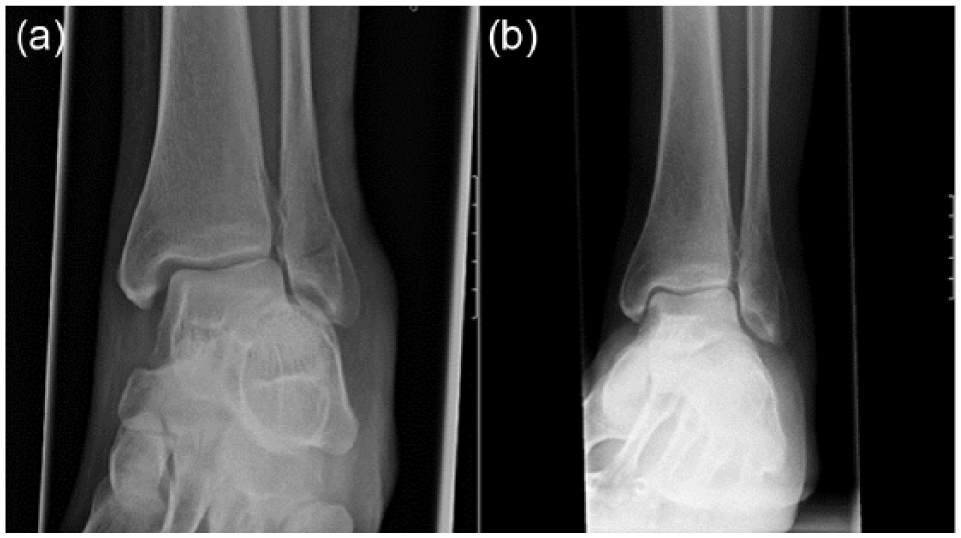
Anteroposterior gravity stress radiograph (a) shows a borderline fracture. However, the weightbearing radiograph (b) demonstrates a clearly stable fracture. Typically, the width of the medial clear space decreased in the weightbearing radiograph.
Two patients did not return for further follow-ups and were treated operatively in another hospital without further examination, proving talar instability. By our protocol, they would have been treated nonoperatively. The remaining 88 patients returned for clinical and full weightbearing radiographic follow-up 6 weeks after trauma. In 39 of the 88 patients (44%), symptoms persisted (painful full weightbearing), and they were seen again 4 to 6 weeks later and radiographs were repeated. At the 3-month follow-up control, 4 of the 88 patients (5%) complained of some discomfort and required further control. As part of this study, all patients were offered 1- and 2-year follow-up, including weightbearing anteroposterior and lateral radiographs of the ankle and standardized questionnaires. The patients who did not return for the 1- or 2-year follow-up were contacted by telephone to answer the questionnaire. The following questionnaires were used to assess the results: American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, 12 Foot Functional Index (FFI), 2 and Short Form 36 (SF-36) score. 24
For the gravity stress mortise radiograph, the patient was positioned laterally on the ipsilateral side of the injured ankle. The most distal half of the leg was dependent off the end of the table, allowing the weight of the foot to create a lateral force across the ankle joint (Figure 3). 17 The MCS was measured on the initial gravity stress radiographs, the first weightbearing radiographs, and the weightbearing radiographs at follow-ups. 7 The MCS is a radiographic criterion and measured as the distance from the medial border of the talus to the lateral border of the medial malleolus on a line parallel to the medial articular surface half the distance between the talar dome and the inferior aspect of the medial articular surface, recorded in millimeters.

Showing how to perform a gravity stress radiograph: For this view, the patient is positioned laterally on the ipsilateral side of the injured ankle. The most distal half of the leg is dependent off the end of the table, allowing the weight of the foot to create a lateral force across the ankle joint. Then a mortise radiograph is taken.
The distal tibial articular surface angle (TAS) and the trochlear angle were measured on the first anteroposterior weightbearing radiographs (Figure 4).18,25 For the TAS, the angle of a line drawn in the center of the fibula from the most proximal point of the radiograph to the level of the tibiotalar joint and a second line from the lateral and medial edge of the tibial articular surface was calculated electronically on digitized radiographs (Sectra, Linköping, Sweden). For the trochlear angle, the angle of 2 lines drawn from the lateral and medial tibial articular surface into the center of the trochlea was measured on the anteroposterior view. On the initial and the last follow-up radiographs, arthritis was graded as “none,” “mild,” “moderate,” and “severe” according to the Kellgren-Lawrence scale. 11
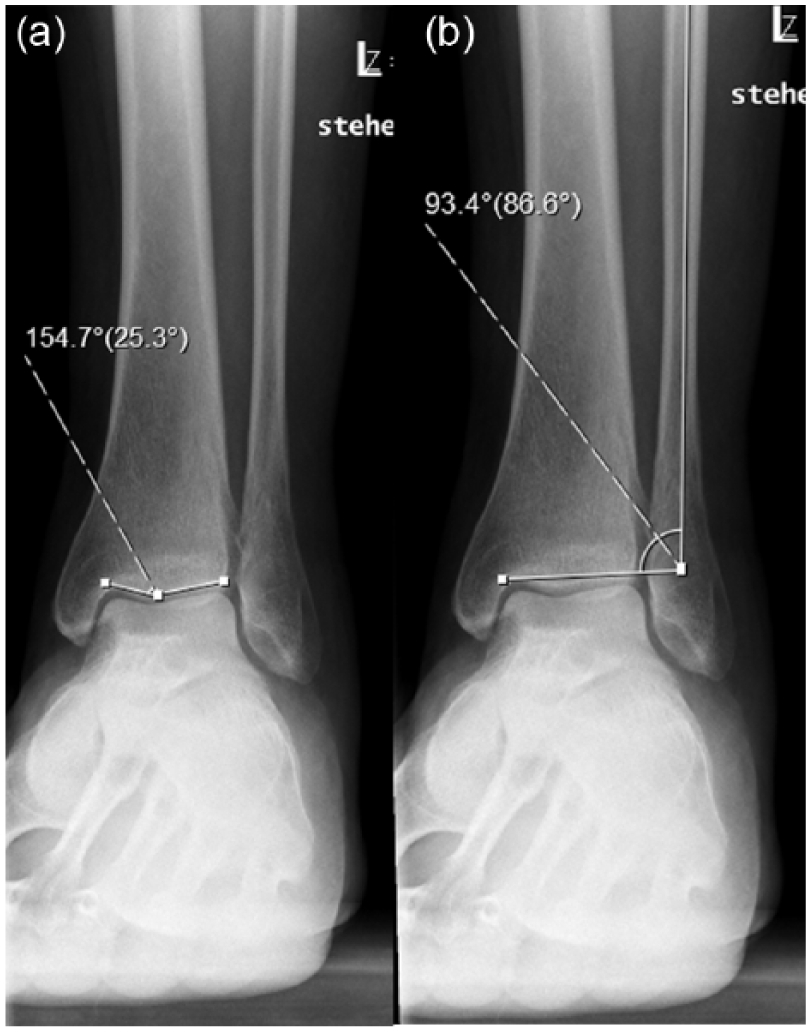
This figure illustrates how the trochlear angle (a) and distal articular surface angle (b) are measured in the weightbearing anteroposterior view.
Patients with an AOFAS score less than 80 points, onset or progression of ankle arthritis, or an ongoing ankle instability as defined above were rated as failures.
For statistic calculations, SPSS statistics (SPSS, Inc, an IBM Company, Chicago, IL) version 19.0 was used. For evaluation of differences of score values and radiographic MCS measurements, the Mann-Whitney U test was applied between the gravity stress–stable/weightbearing-stable (“gravity-stable”) group and gravity stress borderline/weightbearing-stable (“gravity-borderline”) group. Level of significance was set to P < .05. The Spearman correlation was used for the assessment of the correlation of radiographs, functional outcome, and failures. Written informed consent for this study had been obtained from all patients, and the institutional ethic review board approved the study.
Results
Of the study group, 92 had the gravity stress and the weightbearing radiographs 3 to 10 days after injury (mean, 6.5 days). The remaining 12 patients were clearly unstable in the initial radiograph and were treated operatively. Forty-six patients (50%) fulfilled the criteria of stability on both radiographic tests (gravity stable), while 44 patients (47.8%) demonstrated borderline instability on the gravity stress radiograph but stability on the weightbearing radiographs (gravity borderline). Two patients (2.2%) were unstable on the gravity stress radiographs and were unable to accomplish the weightbearing radiographs due to pain and subjective instability. They were therefore advised to have operative treatment. There was no patient with stable gravity stress but unstable weightbearing radiographs and no patient who required conversion to operative treatment.
Seventy-six of the 90 (84.4%) patients who were assigned to the nonoperative treatment group were available for follow-up at a mean of 22.6 months (range, 11.4-59.2 months). Four patients (4.4%) were deceased for reasons unrelated to the malleolar fracture but had not previously reported ankle problems to their relatives. Two of them died of cancer and the other two due to cardiac reasons. Eight patients (8.9%) were lost to follow-up. Of the remaining 76 patients, 62 patients (81.6%) were seen in the outpatient clinic with questionnaires and weightbearing radiographs. The other 14 patients (18.4%) were questioned by telephone and completed the AOFAS ankle-hindfoot score, FFI, and SF-36 score (Figure 1).
The average AOFAS score was 92.8 points (range, 37-100); the FFI, 10.4 points (range, 0-131); the SF-36 physical component, 85.7 points (range, 26.8-100); and the SF-36 mental component, 83.2 points (range, 16.2-100). Comparing the 2 groups of patients (gravity stable and gravity borderline), there was no significant difference in the AOFAS hindfoot score, the FFI, the SF-36 physical component, and the SF-36 mental component (Table 1). The mean follow-up was 22.6 months (23.5 months for gravity-stable group and 21.7 months for gravity-borderline group). Fourteen of the patients with gravity-stable fractures and 12 of the patients with gravity-borderline fractures had a clinical follow-up of 2 or more years.
Outcome Scores. a
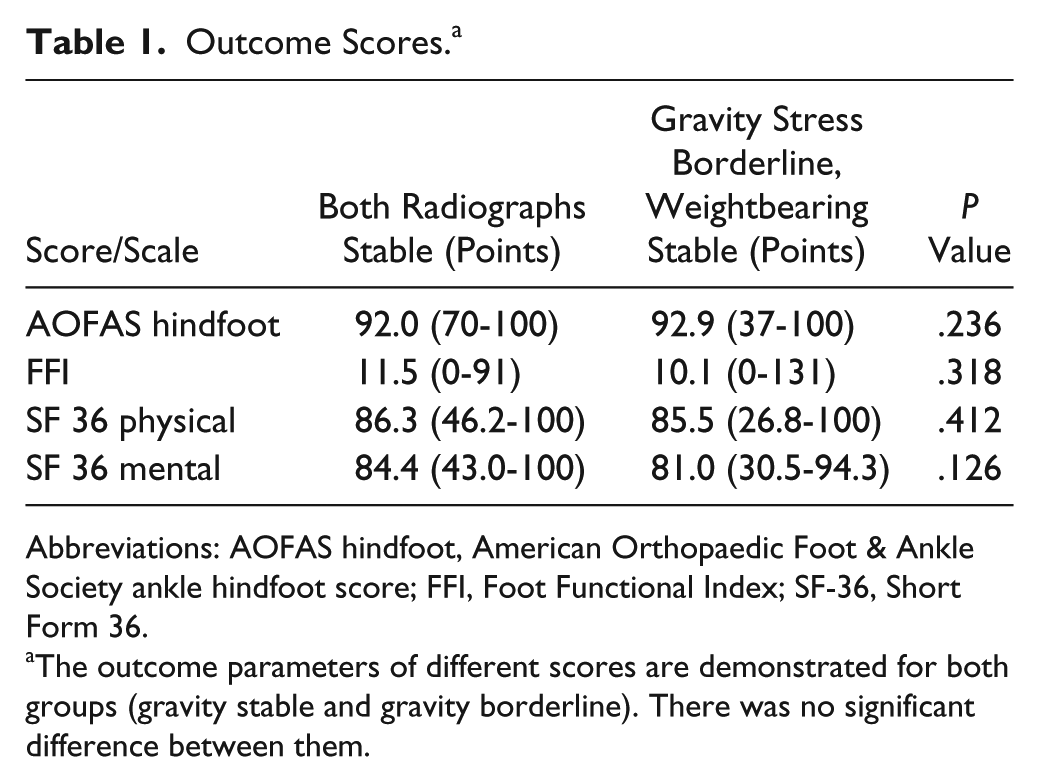
Abbreviations: AOFAS hindfoot, American Orthopaedic Foot & Ankle Society ankle hindfoot score; FFI, Foot Functional Index; SF-36, Short Form 36.
The outcome parameters of different scores are demonstrated for both groups (gravity stable and gravity borderline). There was no significant difference between them.
Analyzing the gravity-stable group, the mean MCS on initial weightbearing radiographs was 2.2 mm (range, 1.2-3.9) and 2.2 mm in the follow-up radiographs (range, 1.0-3.5). For the gravity-borderline group, the mean MCS on the initial weightbearing radiographs was 2.8 (range, 1.2-4) and 2.5 mm in the follow-up radiographs (range, 1.1-3.6), respectively.
The mean MCS on the gravity stress radiographs was 3.3 mm (range, 1.8-3.9) in the gravity-stable group and 5.4 mm (range, 4.1-7.0) in the gravity-borderline group. The statistical analysis of these parameters revealed a significantly wider MCS in the gravity-borderline group for the weightbearing radiographs (P = .001 for initial and P = .015 for radiographs at last follow-up) and also for the gravity stress view (P = .001) (Table 2).
Medial Clear Space. a
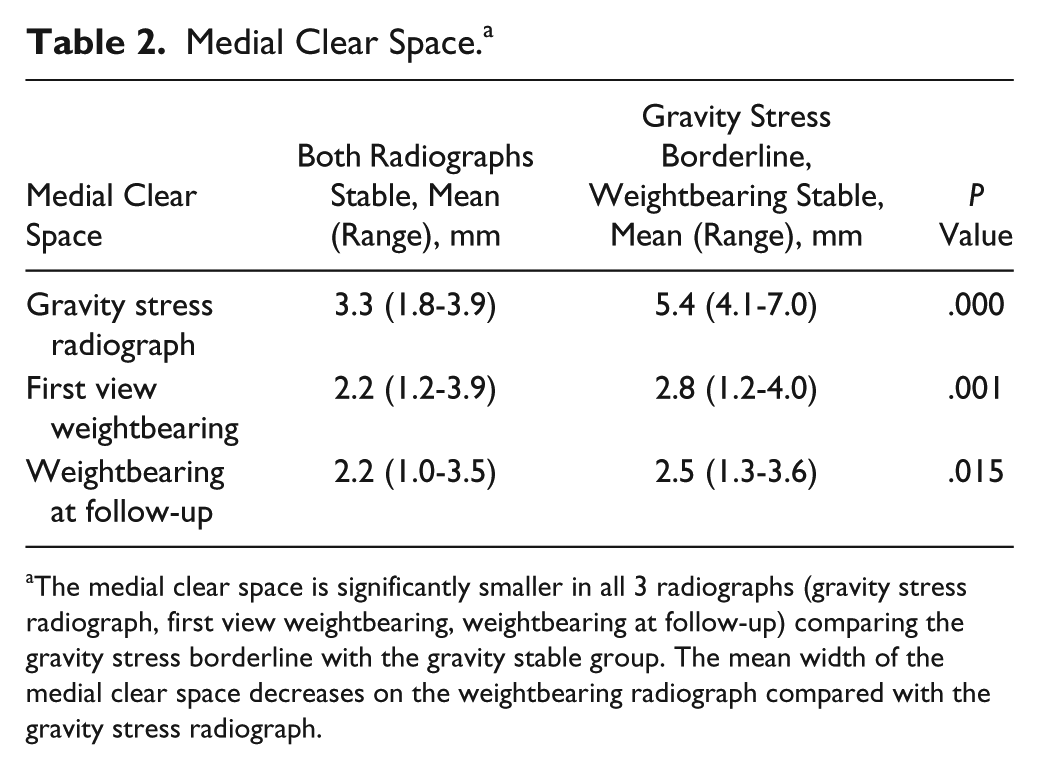
The medial clear space is significantly smaller in all 3 radiographs (gravity stress radiograph, first view weightbearing, weightbearing at follow-up) comparing the gravity stress borderline with the gravity stable group. The mean width of the medial clear space decreases on the weightbearing radiograph compared with the gravity stress radiograph.
The treatment protocol of the gravity-borderline and the gravity-stable group was the same. The time of immobilization in the splint or brace was dependent on the level of pain of the patients at the first follow-up at an average of 6.5 days after injury when the weightbearing radiograph was performed. If patients reported discomfort while walking at the 6-week follow-up, they were seen again at 3 months after the trauma. In 44% of patients, there were persistent symptoms during weightbearing at the 6-week follow-up. Half had a fracture that was borderline in the gravity stress radiograph. Regarding the time of immobilization, 4 patients (all gravity stable) used a cast for 6 days, 10 patients (2 gravity stable and 8 gravity borderline) used a cast for 14 days, and 24 patients (13 gravity stable and 11 gravity borderline) were immobilized for 6 weeks.
In 28 of the gravity-stable group and in 34 of the gravity-borderline group, a radiograph was taken at 1-year follow-up. An additional radiograph 2 or more years after trauma was performed in 6 of the 28 patients (25%) in the gravity-stable group and in 9 of 34 (26%) in the gravity-borderline group. In each group, 2 patients had a slight progression of (preexisting) ankle arthritis (2 patients from Kellgren-Lawrence grade 0 to grade 1 and 2 patients from grade 1 to grade 2). They were therefore rated as failures, but half remained clinically asymptomatic.
There was no significant correlation between the functional and pain outcome score and the trochlear angle (P = .13) or between the scores and the hindfoot alignment as measured by the TAS (P = .15). Similarly, there was no correlation between the outcome measurements and the MCS in the gravity stress radiograph or the initial weightbearing radiograph. In particular, unfavorable ankle anatomy was not seen in the 6 patients rated as failures according to their poor outcome in function and pain.
Overall, 8 patients (13%) were defined as having an unfavorable outcome: 3 patients in the gravity-stable group and 5 patients in the gravity-borderline group (Table 3). Of the 3 patients in the gravity-stable group, 1 patient had posttraumatic midfoot arthrosis prior to the ankle fracture. Another patient had a symptomatic osteochondral lesion. Both lesions probably influenced the outcome independently of our treatment protocol. Thus, only 1 of 28 patients (3.6%) should be assigned as a failure directly due to the nonoperative treatment of the SER fracture. In the group of gravity-borderline fractures, 2 patients with an AOFAS score below 80 had fibromyalgia and complaints of widespread musculoskeletal pain, which was likely a confounding factor. The patient with the lowest AOFAS score of 37 was requesting workers’ compensation. Despite further investigation, no reason for his pain could be found. Thus, only the unfavorable outcome of 2 patients (5.9%)—one of them 83 years old—could be exclusively ascribed to the nonoperative treatment of the ankle fracture.
Unfavorable Outcome.
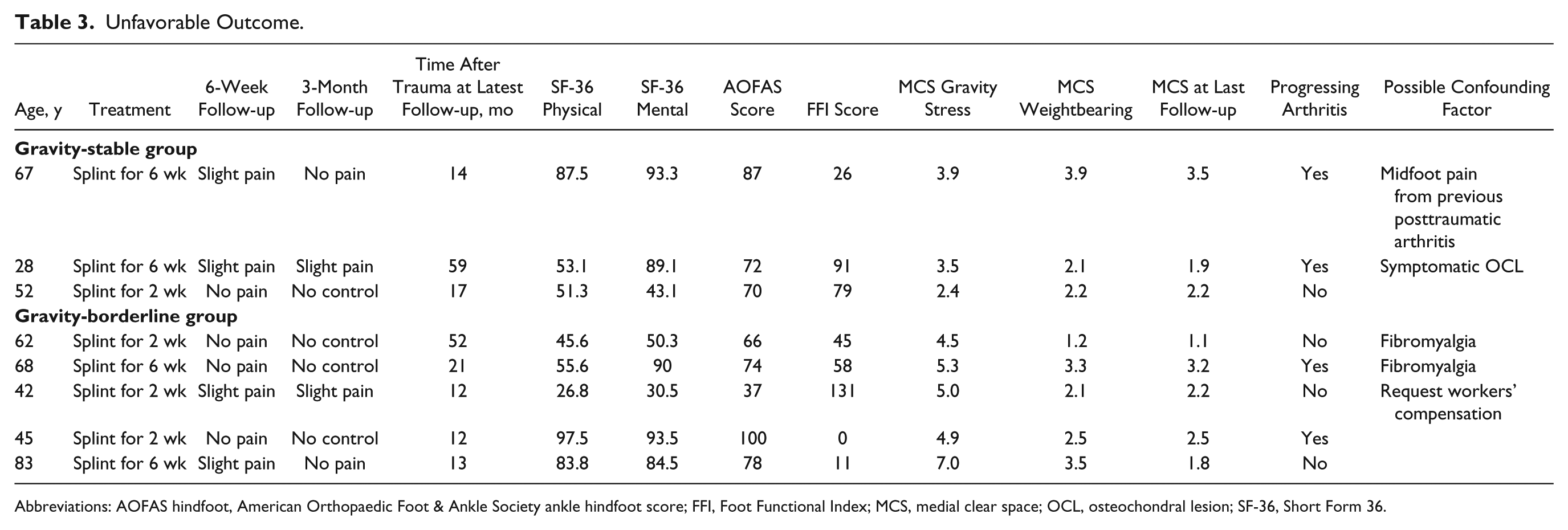
Abbreviations: AOFAS hindfoot, American Orthopaedic Foot & Ankle Society ankle hindfoot score; FFI, Foot Functional Index; MCS, medial clear space; OCL, osteochondral lesion; SF-36, Short Form 36.
Because of the absence of patients with failure by definition and unfavorable bony ankle anatomy (low trochlea angle, valgus TAS) at the same time, the calculation of that correlation was unfeasible.
Finally, in the patient cohort of this study, 14 of 104 patients (13%) were treated operatively due to our criteria of weightbearing radiographs. If the criteria of gravity stress radiographs had been followed, 58 of 104 patients (56%) would have been assigned to undergo surgery.
Discussion
The treatment of isolated lateral malleolar fractures of the SER mechanism 14 is still controversial. If nonoperative treatment is considered, the most important aspect is to evaluate the competence of the deltoid ligament. In cases in which the instability is not clearly visible on the initial radiographs, further radiographic evaluation, such as gravity stress radiographs, is advised since soft tissue indicators (swelling, tenderness, ecchymosis) are not accurate predictors of instability.5,6,15,23
Recently, weightbearing radiographs have been proven to be a reliable method to indicate if sufficient stability for successful nonoperative treatment was present. 26 In our present study, we evaluated the integrity of the deltoid ligament in isolated SER fractures of the lateral malleolus by comparing weightbearing and gravity stress radiographs. Both methods demonstrated comparable good to excellent radiographic and functional outcome at short-term follow-up in most cases. However, our study points out that there is no significant difference in outcome of gravity-stable and gravity-borderline fractures as long as they are stable on the weightbearing radiographs. Therefore, gravity stress radiographs overrated the absolute need for operative treatment in half of the patients. Varus ankle alignment and a pronounced trochlea shape may possibly contribute to fracture stability. However, with the absence of treatment failures for the anatomic reasons given, no statistical correlation was perceived in the study.
Traditionally, a manual external rotation stress or a gravity stress radiograph to evaluate the stability of SER fractures of the lateral malleolus is recommended in the literature.4,7,15,17,23 As already discussed above, some recent studies scrutinized the nonweightbearing stress radiographs, assuming that too many patients might undergo unnecessary surgery.3,8,9,13,26 Hoshino et al 9 used external rotation stress views under fluoroscopy to assess the stability of SER fractures, and the authors correlated the stress-positive fractures to later weightbearing radiographs. As they did not provide information about the width of the MCS in the stress view, a grading of the amount of instability is not possible. Patients with MCS widening in the weightbearing radiographs were advised to have their fracture fixed operatively. One of 36 patients (2.8%) with SER fractures was operated on. Follow-up was on average 12 months, and the average AOFAS hindfoot score was 92 points. The authors stated that using this diagnostic approach reduced the number of unnecessary operations significantly and led to good to excellent results in most cases.
Koval et al 13 suggested the additional use of magnetic resonance imaging (MRI) to assess the integrity of the deltoid ligament in patients with SER fractures and a positive ankle stress test. Nineteen of 21 patients (90.5%) with positive ankle stress tests had at least partial integrity of the deep deltoid ligament on the MRI and were consequently treated nonoperatively with good results. The authors concluded that additional MRI would better define the option of nonoperative treatment. 13
A more straightforward way to evaluate the stability and partial integrity of the deltoid ligament is the use of weightbearing radiographs. In 2010, Weber et al 26 reported on the exclusive use of weightbearing radiographs to assess the stability of SER fractures. Applying weightbearing radiographs, 51 of 57 fractures (90%) were classified as stable and were therefore treated nonoperatively with mainly good to excellent outcome. No conversion of patients to operative treatment was recorded. In contrast to our present study, fractures were evaluated exclusively by weightbearing radiographs without comparing them to stress radiographs. Therefore, the reader is not informed whether all patients would have had negative stress radiographs. The comparison to the gravity stress radiographs in this study allowed us to expand the indication for nonoperative treatment of SER fracture by using the weightbearing radiographs.
Dawe et al 3 reviewed their experience of stability assessment in 312 consecutive patients with SER II to IV fractures. They concluded that patients assessed with gravity stress radiographs were 10 times more likely to undergo surgery and experienced complications more often than those assessed with weightbearing radiographs. It appeared to them that weightbearing radiographs were appropriate for selecting treatment since the short-term results of nonoperative treatment showed low rates of complications or ongoing pain. In contrast to our study, they did not provide any outcome score.
A similar approach was demonstrated by Holmes et al, 8 substantiating the exclusive use of weightbearing radiographs for the evaluation of ankle SER fracture stability. In our present study, 87% of patients with SER fractures were selected for nonoperative treatment. This high number matches well with the results of Holmes et al 8 and Hoshino et al. 9 In contrast, authors exclusively relying on stress radiographs report a substantially higher rate of operations ranging from 36% to 55%.3,15,23
In the present study, 44 patients were defined borderline unstable according to the gravity stress radiographs (gravity-borderline group) and would have undergone surgery in many institutions. Thus, they must have had at least a partial or even a complete tear of the deltoid ligament. However, these patients were stable in their weightbearing radiographs and had successful nonoperative treatment. The results of our study likely indicate that the functional weightbearing condition provides sufficient functional stability of the ankle, even with an incompetent deltoid ligament. It has been reported before that partial integrity of the deltoid ligament provides sufficient stability for nonoperative treatment of SER III and IV ankle fractures. 13
We assume that the highly congruent ankle joint has a high potential for an auto-stabilization. A neutral or varus ankle alignment and/or an appropriate trochlea angulation likely contributes to this functional stability. With the number of patients given, the study did not reveal any statistical correlation between the outcome and a favorable anatomy (prominent trochlea, hindfoot varus alignment). However, it appears reasonable that a nonprominent trochlea or a valgus hindfoot alignment is more likely to increase the instability in type III and IV SER fractures and should therefore be considered in the treatment decision.
The outcome score of an AOFAS score of 92.0 points in the gravity-stable group and 92.9 points in the gravity-borderline group in our patient population is comparable to other studies. Holmes et al 8 found a similar mean AOFAS score of 93 points (52-100 points) in their group of nonoperatively treated SER fractures. In contrast, operatively treated patients in other studies had a similar or lower mean AOFAS score of 76 to 92 points.6,10,16,20 Furthermore, those operatively treated patients had some complications, with a wound infection range of 4% to 16% and even a reoperation rate of 14% to 20%.6,10,16,20,22
Surgeons favoring operative treatment of lateral malleolar fractures at or above the level of the syndesmosis rely on the biomechanical study of Ramsey and Hamilton 21 that analyzed the contact area between talus and tibia with displacement of the tibia. A tibia displacement of only 1 mm significantly reduced the joint contact area by 42% in a cadaver model. However, since for these measurements, all soft tissues of the joints, including ligaments and tendons, were removed and a carbon block was placed in the MCS, the results of contact area reduction cannot be conveyed to the functional weightbearing condition of the ankle. 21 Basically, the static and dynamic effects of the ankle anatomy and the surrounding soft tissues with their high potential for auto-stabilization were not taken into consideration in that biomechanical study.
Our present study supports the hypothesis that weightbearing radiographs identify fracture stability more closely to the actual clinical and biomechanical condition. This study demonstrated that weightbearing radiographs alone would be appropriate to determine ankle SER fracture stability and thereby the option of nonoperative treatment for good to excellent clinical and radiographic outcomes. In contrast to stress radiographs, fewer patients would have unnecessary surgery when weightbearing radiographs were applied for the assessment of SER ankle fracture stability.
A limitation of this study was a short mean follow-up of 23 months and that only 81.6% had an additional radiographic control. Another possible weakness is the low sample size. However, the post hoc power analysis demonstrated that 28 patients per group would be appropriate to statistically detect a clinically relevant difference of the AOFAS hindfoot score. An important strength is the prospective study design. To our knowledge, this is the first study that directly compared the outcome of patients with stable and unstable SER fractures assessed by gravity stress and weightbearing radiographs at the same time.
Conclusion
We demonstrated that weightbearing radiographs were a reliable method to evaluate functional stability in isolated lateral malleolar fractures of the SER type, allowing successful nonoperative treatment. Gravity stress radiographs indicated a higher number of presumed instability. Yet this presumed instability was not clinical relevant as the clinical outcome was equivalent in both groups. No conversion of nonoperative to operative treatment was required in patients with “gravity stress borderline-unstable” but “weightbearing-stable” radiographs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.