
Abstract
Background:
Total joint surgeons have successfully performed hip, knee, and shoulder arthroplasty procedures in the outpatient setting without compromising safety, satisfaction, or results. The purpose of this study was to evaluate outpatient total ankle arthroplasty (TAA) as compared with overnight or extended inpatient stay, with regard to 90-day medical and operative complications, reoperations, readmissions or emergency room visits, and pain control.
Methods:
The medical records of patients who underwent TAA with 1 fellowship-trained orthopedic foot and ankle surgeon were reviewed. Outcome measures included operative complications, adverse medical events, readmission or emergency room visit for any reason, or reoperation within 90 days following surgery; surgeon’s office contact before first postoperative visit regarding pain or other issues; visual analog scale pain score at the first postoperative visit; and need for narcotic refill. Outcomes were assessed by admission status: outpatient, overnight observation, or inpatient admission. Standard statistical analysis was used, and P < .05 was considered significant.
Results:
Eighty-one patients underwent TAA who met inclusion criteria, and 8 had a complication (10%). A significant difference in complication rate was seen among groups (P = .01) but not rate of readmission or reoperation. Of 16 patients, 5 (31%) who were admitted for 2 or more nights following surgery had a complication, as opposed to 3 of 65 (5%) who were outpatient or admitted overnight (P = .01). There were no differences in frequency of postoperative phone calls, narcotic refills, or visual analog scale pain scores at the first postoperative visit. There were no adverse medical events.
Conclusion:
With proper instruction, TAA was performed safely in the outpatient setting. As health care policy continues to evolve in the United States, safe and efficient practices will remain a priority.
Level of Evidence:
Level III, retrospective comparative study.
Total ankle arthroplasty (TAA) continues to be an increasingly utilized treatment option for end-stage ankle arthritis, up 7-fold from 1998 to 2010. 22 TAA is commonly performed at a hospital, as opposed to an outpatient surgery center, and average length of stay following the procedure is reported to be 2.5 to 3.2 days.3,14,22 High-volume TAA surgeons (volume greater than 90th percentile) have been shown to average about 1 day less in length of stay, and in recent years many have routinely admitted patients for a single night of observation. 3 However, outpatient TAA—meaning a stay of less than 12 hours and same day discharge home—is rarely performed.
As health care policy in the United States continues to evolve, treatment delivered in a safe and cost-effective manner has become a priority. Over the past decade, other joint replacement procedures—including total knee arthroplasty, unicompartmental knee arthroplasty, total hip arthroplasty, and total shoulder arthroplasty—have been successfully performed in an outpatient setting with equivalent results and no compromise to patient safety.1,4,5,7,9,11,12,15,16 Concerns regarding pain control, patient compliance, and perioperative complications have previously prevented joint replacement surgeons, including foot and ankle surgeons, from allowing same-day discharge. However, appropriate patient selection, improvements in operative technique, advances in regional anesthesia and multimodal pain management, and expedited rehabilitation protocols have made outpatient joint replacement a viable option.
Ankle arthrodesis and many other foot and ankle procedures are increasingly being performed at outpatient surgery centers, but TAA has yet to catch on to this trend for reasons previously listed.6,18 The safety and efficacy of outpatient TAA have not been described in the literature. The purpose of this study was to evaluate outpatient TAA as a safe option to alternative admission status, with attention to 90-day global period medical and operative complications, reoperations, readmissions or emergency room visits, and pain control.
Methods
Following institutional review board approval, the medical records of consecutive patients who underwent primary TAA with 1 fellowship-trained foot and ankle orthopedic surgeon (S.G.P.) were reviewed from January 2013 to July 2016. Patients were included if medical records were available at least 90 days following surgery, which represents the global period commonly used by insurance companies. Those undergoing a revision ankle arthroplasty were excluded. One primary arthroplasty patient was excluded because of involvement in a motor vehicle accident 1 month following surgery. Trauma was sustained to the operative extremity resulting in anterior wound full-thickness breakdown that necessitated readmission and reoperation (debridement and irrigation, polyethylene exchange, and radial forearm flap).
Retrospective review of all clinic, operative, and hospital records was conducted for data collection. Patient demographic data were recorded—including age, sex, American Society of Anesthesiologists (ASA) score, operative extremity, diagnosis, medical comorbidities, ankle arthroplasty implant used, operative time, and additional procedures. Outcomes examined were length of stay and any complication, adverse medical event, readmission or emergency room visit for any reason, or reoperation within the first 90 days following surgery. Also collected was any notation of phone call or email to the surgeon’s office prior to first operative visit regarding pain or other issues, visual analog scale (VAS) pain score at the first postoperative visit at 1 week, and need for narcotic refill at the first postoperative visit at 1 week. Outcomes were assessed among 3 cohorts: those who were “outpatient” and discharged the same day of surgery, those who were admitted overnight for 23-hour “overnight observation” period, and those who received “inpatient” admission and stayed 2 or more nights in the hospital. As an adjunct to the primary purpose of the study, outcomes were compared by arthroplasty implant used.
All patients had clinical and radiographic indications for TAA consistent with end-stage ankle arthritis. Ultimate decision making included consideration of age, comorbidities, and social issues. Preanesthesia evaluation was performed for all patients prior to the day of surgery for a thorough review of their medical history, and in all cases an ASA score was applied as a subjective assessment of overall health status. In all cases a fellow or resident, in addition to a physician assistant, was available to assist. The operation was performed by the senior author (S.G.P.), and wound closure was done under his direct supervision by a qualified assistant.
Implants used were at the discretion of the surgeon and included the Cadence (Integra LifeSciences, Plainsboro, NJ), Inbone II (Wright Medical, Memphis, TN), Infinity (Wright Medical, Memphis, TN), Salto Talaris (Integra LifeSciences, Plainsboro, NJ), STAR (Stryker, Mahwah, NJ), and Zimmer Trabecular Metal (henceforth, Zimmer TM; Zimmer Biomet, Warsaw, IN). There are some fundamental differences in operative technique for each implant, and surgeons should refer to their respective technique guides for specific details. Of note, the Inbone II prosthesis requires a plantar incision and drilling through the calcaneus and talus for insertion of the tibial component. The Zimmer TM prosthesis is implanted through a lateral approach. For all except the Zimmer TM implant, a standard 10-cm anterior ankle incision was utilized with care to incorporate prior incisions or leave an adequate skin bridge. The Zimmer TM implant utilized a 10-cm lateral incision. Guides were used to make bone cuts appropriate for implantation of the prosthesis according to the manufacturer’s guidelines. Custom guides created with computed tomography assistance were not used. In some cases, additional procedures were performed to balance the foot and ankle. An additional procedure was defined as “major” if it required osteotomy or extensive dissection that could lead to increased chance for pain or complication. Such procedures included peroneal allograft reconstruction, tendon transfer, or osteotomies of the calcaneus, medial cuneiform, first metatarsal, and fibula. Other procedures were not considered major, such as hardware removal, tendo-Achilles lengthening, and ligament balancing included with the TAA bundle. Prior to closure, the operative site was copiously irrigated with a dilute antibiotic solution. The operative site was closed in layers, including the deep ankle capsule, the extensor retinaculum, the subcutaneous tissue layer, and the skin. In those cases utilizing an anterior approach, a DermaClose device (Wound Care Technologies, Chanhassen, MN) and a PICO negative pressure wound therapy device (Smith & Nephew, Hull, UK) were used. A well-padded short leg splint was applied.
All patients received a general anesthetic and regional anesthetic either as (1) a single-shot popliteal block with ropivacaine from the anesthesiologist, followed by periarticular liposomal bupivacaine at the end of the procedure given by the surgeon, or (2) a continuous popliteal catheter with ropivacaine infusion alone placed by the anesthesiologist. Early in the series (after 6 patients), the surgeon transitioned regional anesthesia techniques to include liposomal bupivacaine in consecutive patients. The technique described by Matsumoto and Parekh was utilized. 17
Following surgery, all patients were initially transferred to a postanesthesia care unit. All procedures were performed in a hospital setting; however, patients were predetermined to either go home the same day of surgery or be observed overnight on the orthopedic floor of the hospital with the possibility of a multiple-night stay due to a variety of factors. This decision included input from the surgeon, anesthesiologist, preoperative medical consultants, and the patient but to some degree was dictated by insurance carrier. No patients were held overnight who had planned on going home the day of surgery, and vice versa. For those planning on same-day discharge, once they could urinate without assistance, pain control was adequate, and they could safely transfer and mobilize nonweightbearing to the operative extremity, discharge home was initiated. Patients being admitted were transferred to the orthopedic hospital floor. Following overnight stay, once evaluated by the orthopedic team with similar criteria met, patients were discharged home.
In addition to the regional anesthetic, the postoperative pain medication protocol included oral immediate-release oxycodone for moderate pain and intravenous morphine for severe breakthrough pain, if the patient was admitted. Every patient was also started on a 2-week course of gabapentin and a 3-day course of meloxicam. Alternative medications were substituted for allergies. Standard postoperative instructions for all patients included nonweightbearing to the operative extremity, elevation of the extremity, and anticoagulation with a baby aspirin or alternative, if risk factors were present for venous thromboembolism.
Standard statistical analysis was performed with SPSS 23 (IBM, Armonk, NY). One-way analysis of variance and Fisher’s exact test contingency tables were used to compare continuous and categorical variables, respectively. P < .05 was considered significant.
Results
Over a 42-month period, 81 patients who underwent TAA met inclusion criteria. No statistical differences were found among outpatient, overnight observation, and inpatient admission groups with regard to age, preoperative ASA score, sex, laterality, operative indication, medical comorbidities, operative time, additional number of procedures, or association of major procedures. Other than the Infinity implant (P = .03), which was more common in the outpatient group, there were no significant differences in the frequency of implant used among groups (Table 1). Patient characteristics grouped by implant choice are seen in Table 2. There was a significant difference in operative time among groups (P < .01), with the Inbone II and Zimmer TM prostheses requiring more time for implantation.
Patient Characteristics, by Admission Status. a
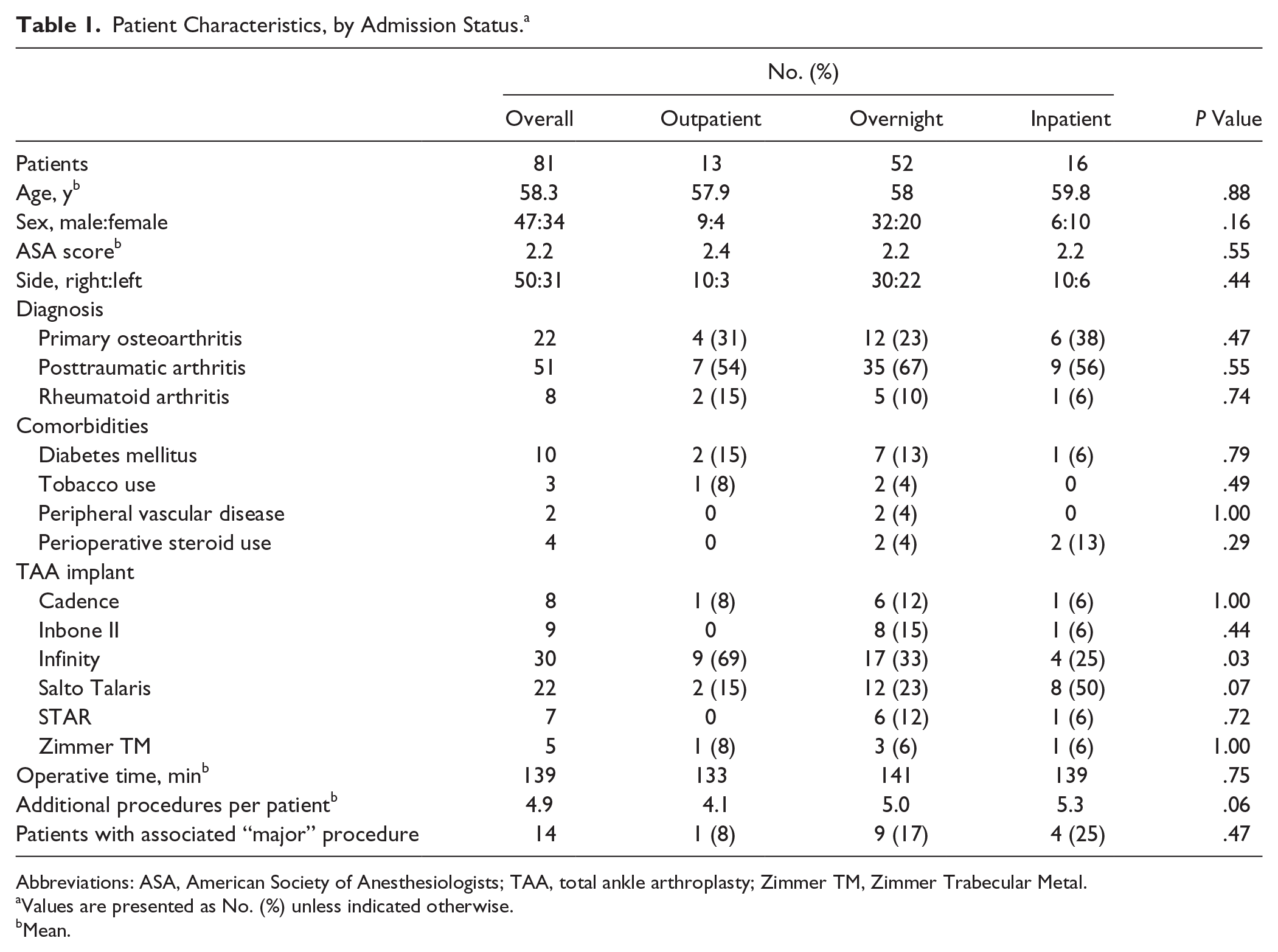
Abbreviations: ASA, American Society of Anesthesiologists; TAA, total ankle arthroplasty; Zimmer TM, Zimmer Trabecular Metal.
Values are presented as No. (%) unless indicated otherwise.
Mean.
Patient Characteristics, by Implant. a
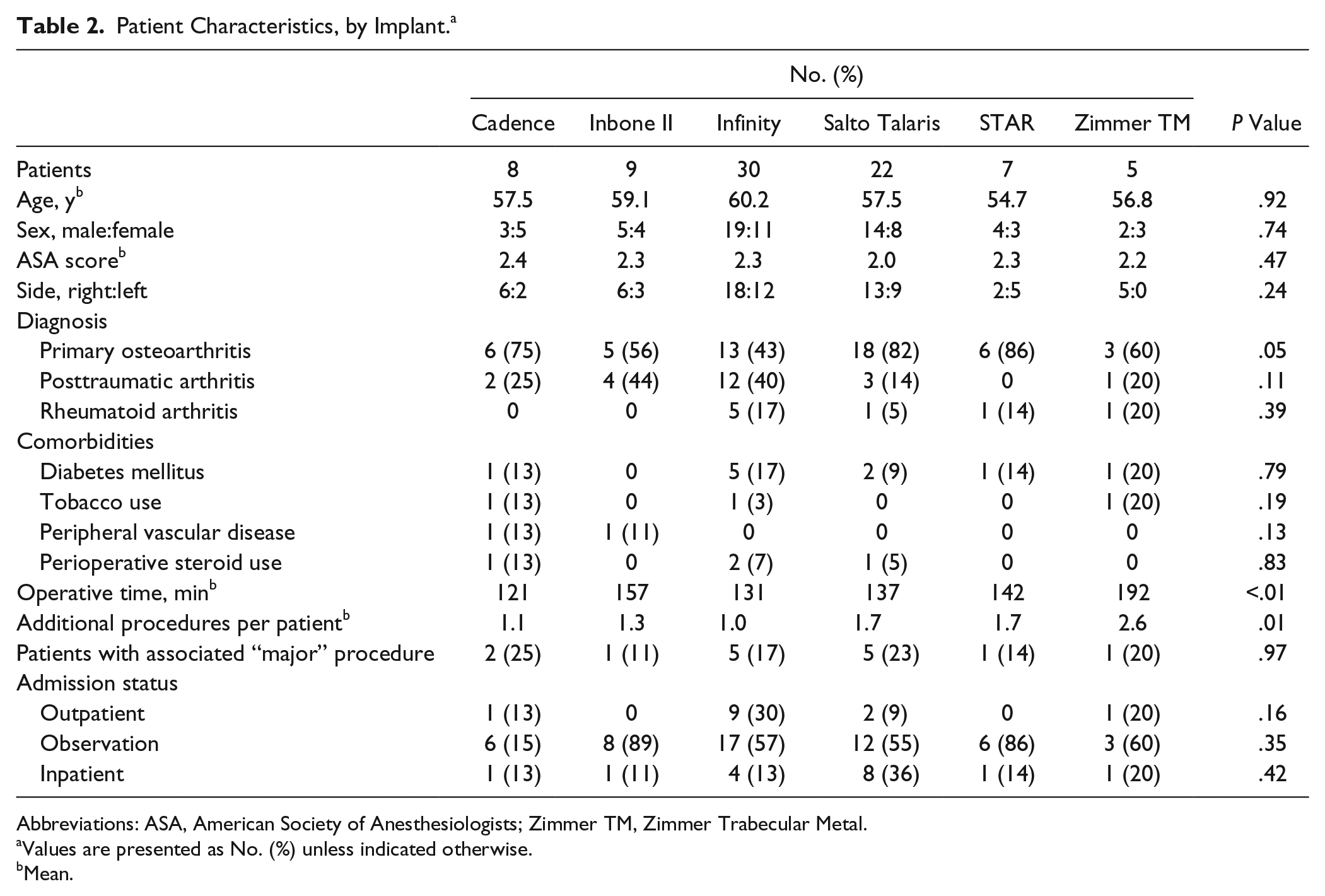
Abbreviations: ASA, American Society of Anesthesiologists; Zimmer TM, Zimmer Trabecular Metal.
Values are presented as No. (%) unless indicated otherwise.
Mean.
Of the 81 patients, 9 (10%) had a complication following surgery. A significant difference in complication rate was seen among groups (P = .01) but not rate of readmission or reoperation (Table 3). There were no additional emergency room visits beyond the readmissions. Of 16 patients admitted for 2 or more nights following surgery, 5 had a complication within 90 days of the procedure, which was significantly more common than the other groups in post hoc analysis (31% vs 5%, P = .01). All 5 complications in this group were superficial anterior wound breakdown with delayed healing, involving a small portion of the wound. All were initially treated with oral antibiotics, local wound care, and dressing changes. One required subsequent split-thickness skin grafting more than 90 days after surgery (therefore not considered a reoperation). The outpatient group had 1 superficial wound complication treated initially in a similar manner and later required split-thickness skin grafting more than 90 days after surgery. There were 2 superficial wound breakdowns in the overnight observation group. There was 1 patient readmitted 4 days after surgery for placement in a rehabilitation facility because of an inability to care for oneself following discharge home. No other adverse events were observed, including pulmonary complication, cardiac event, or death.
Results, by Admission Status. a
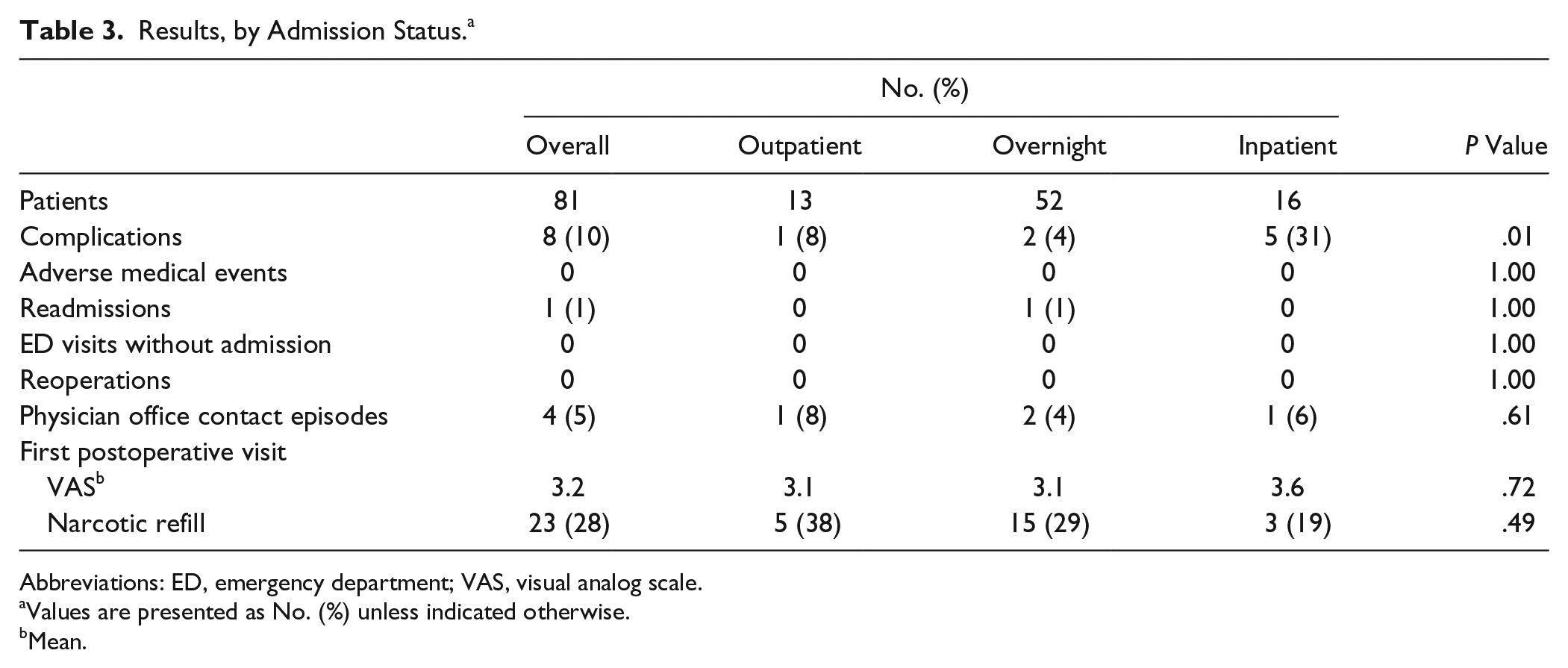
Abbreviations: ED, emergency department; VAS, visual analog scale.
Values are presented as No. (%) unless indicated otherwise.
Mean.
Contact with the surgeon’s office prior to first postoperative visit was infrequent (4 of 81 patients, 5%), and no difference was found among groups. There were also no differences seen in first postoperative VAS pain score or need of narcotic pain medication refill at the first visit (Table 3). There were no statistically significant differences in results when compared by implant used (Table 4).
Results, by Implant. a
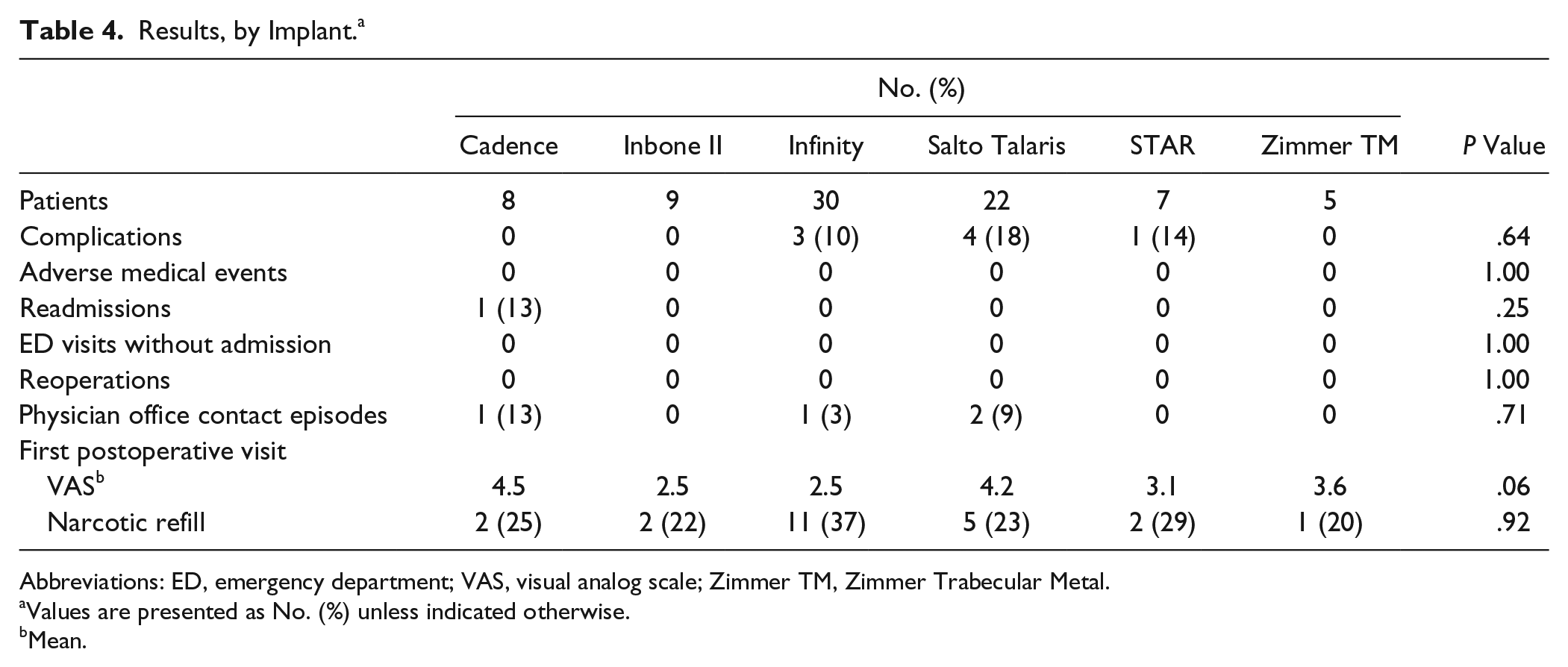
Abbreviations: ED, emergency department; VAS, visual analog scale; Zimmer TM, Zimmer Trabecular Metal.
Values are presented as No. (%) unless indicated otherwise.
Mean.
Discussion
Providing efficient delivery of health care without compromising patient safety is a common goal among surgeons and health care policy makers. Recent literature suggests that a transition of common orthopedic procedures, such as joint replacement, from an inpatient setting with postoperative hospital admission to outpatient facilities and same-day discharge is safe and potentially cost-effective.1,4,5,7,9,11,12,15,16 This study is the first to evaluate ankle arthroplasty in an outpatient setting, and, consistent with findings in other joint replacement procedures, it was a safe and effective alternative to hospital admission among similar patient cohorts.
In the knee literature, Berger et al found 94% of 111 knee arthroplasty patients able to be discharged home the day of surgery. 4 There were 4 readmissions and 1 emergency room visit the first week following surgery and 4 other subsequent readmissions and 1 other emergency room visit in the 90-day postoperative period. Perhaps more important, there were no deaths, cardiac events, or pulmonary complications in the group. Kolisek et al matched 2 cohorts of 64 patients undergoing total knee arthroplasty in an inpatient and outpatient setting. 15 There were no perioperative complications in either cohort, and none returned to the hospital for any reason. Similarly, Cross and Berger performed unicompartmental knee arthroplasty on 105 consecutive patients, and all were discharged home the same day, with only 1 readmission for deep infection. 9
In a prospective study, Goyal et al found no difference in reoperation, readmission, emergency department visit, or physician office contact following randomized inpatient or outpatient total hip arthroplasty in a defined patient population. 12 There were, however, slightly increased VAS pain scores in the outpatient group, 3.7 vs 2.9 (P < .01). Berger et al followed 150 consecutive outpatient total hip arthroplasties and observed only 1 readmission and 9 emergency department visits in the 90-day postoperative period. 5 Similarly, Dorr et al found no hospital readmissions and 96% satisfaction following outpatient total hip arthroplasty. 11
Shoulder surgeons have more recently transitioned to outpatient total shoulder arthroplasty. Brolin et al compared matched cohorts of inpatient and outpatient total shoulder arthroplasty and reported no readmissions, no reoperations, and similarly low rates of complication within 90 days of surgery. 7 A US population database was reviewed by Leroux et al, who found no difference in 30-day adverse event or readmission rates. 16
In our study, 8 of 81 patients (10%) had a wound complication. The anterior approach utilized in those patients who subsequently had wound complication is a well-known risk, reported to occur in 2% to 40% of patients.19,21 Five patients had a Zimmer TM ankle replacement implanted through a lateral approach, and there were no wound complications. We observed a significantly higher rate of wound complications in the group of patients admitted for 2 or more nights. This is likely due to risk factors not captured by demographic data collected or ASA score for medical comorbidities.
Evaluation of our results based on implant used was performed secondarily to better understand our results and possibly correlate with better or worse outcomes. Operative time was the only significant variable among implants. The Inbone II and Zimmer TM required extra time for placement in an external frame to determine proper alignment. The Inbone II also required extra steps for drilling and placement of the tibial component, and the Zimmer TM required a fibular osteotomy with subsequent fixation. There was no difference among the implants in complication rate or any other outcome measure. Note that the senior author is on the design team for the Cadence total ankle device. Since this study was performed, the Cadence total ankle device was reviewed by the Food and Drug Administration for a series of posterior malleolus fractures, and a change in the technique guide was made, one not seen in any patient in our series.
There are limitations to this study, including its retrospective design and inability to randomly assign patient’s length of stay. Despite similar demographic profiles, comorbidity scores, and operative details, there were likely other uncaptured factors that contributed to admission status and outcomes. We also recognize that the relatively small cohort and single surgeon experience allow for less generalizability but did allow for a more standardized operative technique and postoperative protocol. Cost comparison data were not available for this study but are an important future direction for this topic.
We also recognize that the senior author has some unique features to his ankle arthroplasty protocol. Early in this series, a transition was made to liposomal bupivacaine (Exparel; Pacira Pharmaceuticals, Parsippany, NJ) for regional anesthesia. Despite good results in hip, knee, and shoulder arthroplasty, enthusiasm for its use in the ankle has yet to occur.2,8,10,20,23 We are currently comparing liposomal bupivacaine to other regional anesthetic techniques to better understand its efficacy. It should be noted that all outpatient ankle arthroplasty patients in this series received liposomal bupivacaine.
The DermaClose device and negative pressure wound therapy have shown some benefit in tenuous wounds about the ankle. 13 Despite a 10% wound complication rate, many of these were small areas of dehiscence or superficial necrosis that resolved with local treatment and antibiotics and no operative intervention. There was no correlation with medical comorbidities. Although a 10% wound complication rate may be considered relatively high, we had a very low threshold to report wound issues, and most were minor. The literature varies greatly in reported incidence of wound complications following TAA, ranging from 2% to 40%, and this is most likely due to definition and inclusion of minor wound complications.19,21 It is worth noting that there were no wound complications with the Zimmer TM implant when utilizing the lateral approach. While the anterior approach has its limitations, the lateral approach to the ankle has a long track record of minimal wound-healing issues, presuming proper soft tissue handling. Finally, while there is no evidence to support the use of meloxicam and gabapentin following ankle arthroplasty, the intention is to reduce opioid use in the postoperative period and block pain at multiple pathways. Although controversial, it may be beneficial to those planning earlier discharge home.
In conclusion, as the landscape of US health care continues to change, recognizing more efficient practices without compromising care and outcomes is critical. Our results demonstrate that outpatient, same-day discharge of TAA patients was a safe and viable alternative to traditional inpatient admission or overnight observation. Future studies should assess patient satisfaction and cost-effectiveness of this change in practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Selene G. Parekh, MD, MBA, reports as a consultant for Pacira.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.