
Abstract
Background:
A variety of operative approaches and fixation techniques have been described for tibiotalocalcaneal (TTC) arthrodesis. The intramedullary (IM) nail and lateral, fixed-angle plating are commonly used because of ease of use and favorable biomechanical properties. A lateral, transfibular (LTF) approach allows for direct access to the tibiotalar and subtalar joints, but the posterior, Achilles tendon–splitting (PATS) approach offers a robust soft tissue envelope. The purpose of this study was to compare the results of TTC arthrodesis with either a PATS approach with IM nailing or LTF approach with fixed-angle plating.
Methods:
A retrospective review was performed on all patients who underwent simultaneous TTC arthrodesis with minimum 1 year clinical and radiographic follow up. Patients were excluded if they underwent TTC arthrodesis through an approach other than PATS or LTF, and received fixation without an IM nail or fixed-angle plate. Primary outcomes examined were union rate, revisions, and complications. Thirty-eight patients underwent TTC arthrodesis with a PATS approach and IM nailing, and 28 with a LTF approach and lateral plating.
Results:
The overall union rate was 71%; 76% (29 of 38 patients) for the PATS/IM nail group, and 64% (18 of 28) for LTF/plating group (P = .41). Symptomatic nonunion requiring revision arthrodesis occurred in 16% (6 of 38) of the PATS/IM nail group versus 7% (2 of 28) in the LTF/lateral plating group (P = .45). There were no significant differences in individual tibiotalar or subtalar union rates, superficial wound problems, infection, symptomatic hardware, stress fractures, or nerve irritations.
Conclusion:
Union, revision, and complication rates were similar for TTC arthrodesis performed with a PATS approach and IM nail compared with an LTF approach and fixed-angle plate in a complex patient population. Both techniques were adequate, especially when prior incisions, preexisting hardware, or deformity preclude options.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Tibiotalocalcaneal (TTC) arthrodesis is a complex operation, often utilized as a salvage procedure for a wide variety of indications. Patients present with symptomatic, end-stage arthritis of the tibiotalar and subtalar joints due to posttraumatic arthritis, inflammatory arthropathy, Charcot neuroarthropathy, acquired or neuromuscular deformity, avascular necrosis of the talus, nonunion of attempted tibiotalar and/or subtalar fusion, and failed total ankle arthroplasty (TAA).7,14,19,23,24,40,45,46
A number of operative approaches, techniques, and fixation strategies have been described to perform TTC arthrodesis. The most common approaches include lateral transfibular, posterior, and dual anterior/sinus tarsi; however, others have been described as well.17,24,33,41 A lateral approach allows for direct access to the tibiotalar and subtalar joints, but necessitates osteotomy of the lateral fibular strut. A potentially safer alternative is the posterior, Achilles tendon–splitting approach, which allows for preservation of bloody supply to the skin with similar outcomes.4,17,20,38,43,48 A midline incision over the Achilles tendon divides the peroneal angiosome from the posterior tibial angiosome. 4 The soft tissue envelope afforded by the posterior approach is also typically more substantial than the anterior or lateral ankle, and less likely to have issues with wound closure in cases of severe deformity correction. 33
The literature has multiple fixation strategies for TTC arthrodesis. Published biomechanical studies comparing intramedullary nailing and fixed-angle plating conflict in their conclusions regarding superiority.3,10,11,18,28,29,35-37 The transfibular approach is conducive to plating with either a blade plate or anatomic locking plate, whereas the posterior approach and prone position allow easy insertion of a durable, load-sharing intramedullary nail. To our knowledge, the comparative clinical results have not been reported.
The purpose of this study was to compare the results of TTC arthrodesis between the posterior, Achilles tendon–splitting approach (PATS) and intramedullary (IM) nailing versus the lateral, transfibular (LTF) approach and lateral, fixed-angle plating. Our hypothesis was that TTC arthrodesis with the PATS approach and IM nailing would result in less wound healing problems, and osteotomy of the fibula in the LTF/plating technique would be detrimental to results, including union rate.
Methods
Following institutional review board approval, a retrospective chart review from 2005 to 2013 was performed on the patients of 4 fellowship-trained orthopedic foot and ankle surgeons at a single, academic center (S.B.A., M.E.E., J.K.D., J.A.N.). A review of the medical records including all clinic notes, operative reports, and radiographic imaging was performed by a fellowship-trained orthopedic foot and ankle surgeon without any involvement in the patient’s care. To be included in the review, patients had undergone simultaneous tibiotalar (TT) and subtalar (ST) arthrodesis through either a PATS approach with IM nailing or LTF approach with fixed-angle plating. All other operative approach and fixation combinations for TTC arthrodesis were excluded. Patients included were those undergoing primary TTC arthrodesis, although in some instances they had already undergone prior TT or ST arthrodesis with subsequent nonunion. All patients were older than 18 years at the time of their operation and had a minimum of 1 year clinical and radiographic follow-up.
All procedures were performed at the discretion of the treating surgeon. Prior to surgery, patients had failed an extended trial of conservative measures including pain medication, ankle-foot orthoses, corticosteroid injections, and physical therapy. TTC arthrodesis was indicated for a variety of diagnoses, including, but not limited to, combined degenerative changes to the tibiotalar and subtalar joints, talus avascular necrosis with collapse and joint involvement, failed prior arthrodesis and subsequent adjacent joint degeneration, failed prior ankle arthroplasty, neuropathic arthritis with or without deformity, and end-stage flat foot deformity (Figure 1).
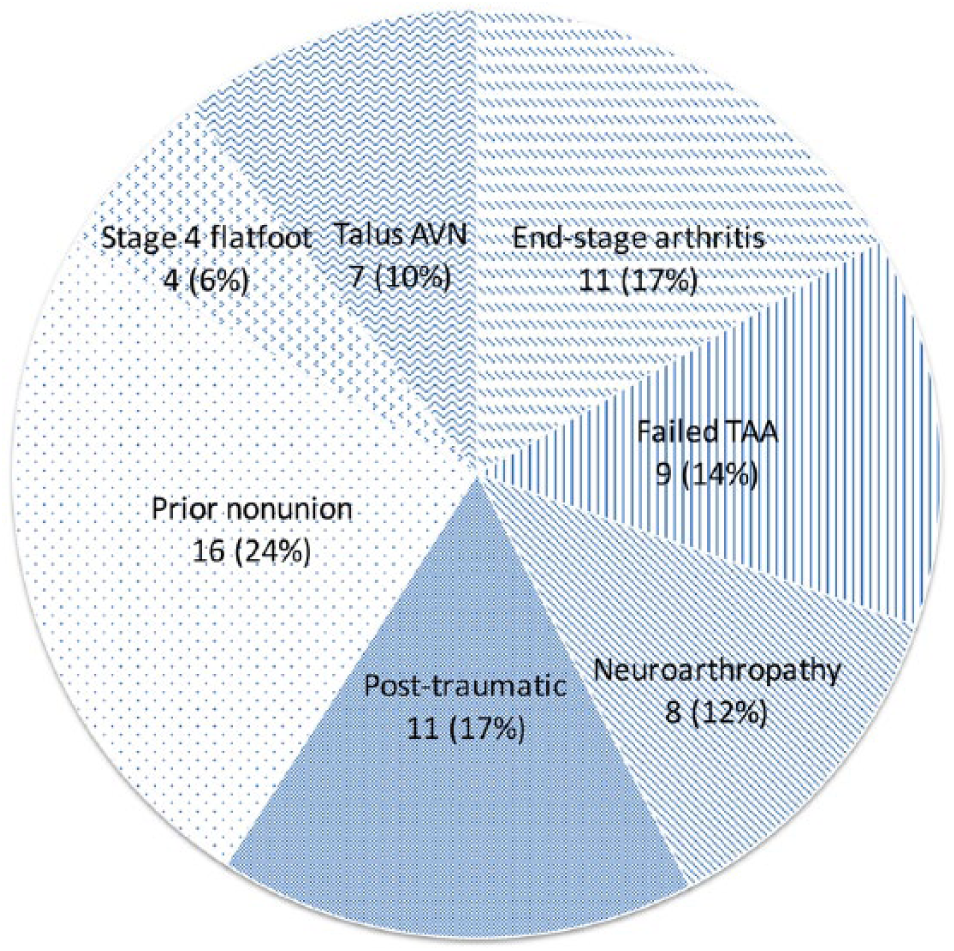
Distribution of indications for tibiotalocalcaneal (TTC) arthrodesis (overall).
Chart review was performed to determine patient demographics, indications, comorbidities, approach utilized, fixation techniques used including supplementary screw or plate fixation, and use of bone graft or orthobiologic products. Primary outcome measures included rate of union, need for revision arthrodesis, and any other complication. Radiographic union was defined as bridging bone seen on 3 of 4 cortices on orthogonal images. Computed tomographic (CT) scans were obtained based on either surgeon preference or evaluation of nonunion. Union on the CT scan was defined as bridging trabecular bone on more than 50% of the surface area of the site of arthrodesis. 16 Twenty-nine of 66 (44%) had a postoperative CT scan available.
Sixty-six patients were identified who met inclusion criteria. Thirty-eight underwent TTC arthrodesis through a PATS approach with IM nailing and 28 underwent the same procedure through an LTF approach and fixed-ankle plating. In total, there were 29 males and 37 females, and average age at the time of surgery was 58.9 years. Mean follow-up was 73 months, with a range of 12 to 123 months. A comparison of patient characteristics between treatment groups can be seen in Table 1. The LTF group did have a significantly higher body mass index (P = .04) and average follow-up (P = .01) when compared with the PATS group. Diabetes was also more prevalent in the LTF group (11 of 28, P = .02).
Patient Characteristics.
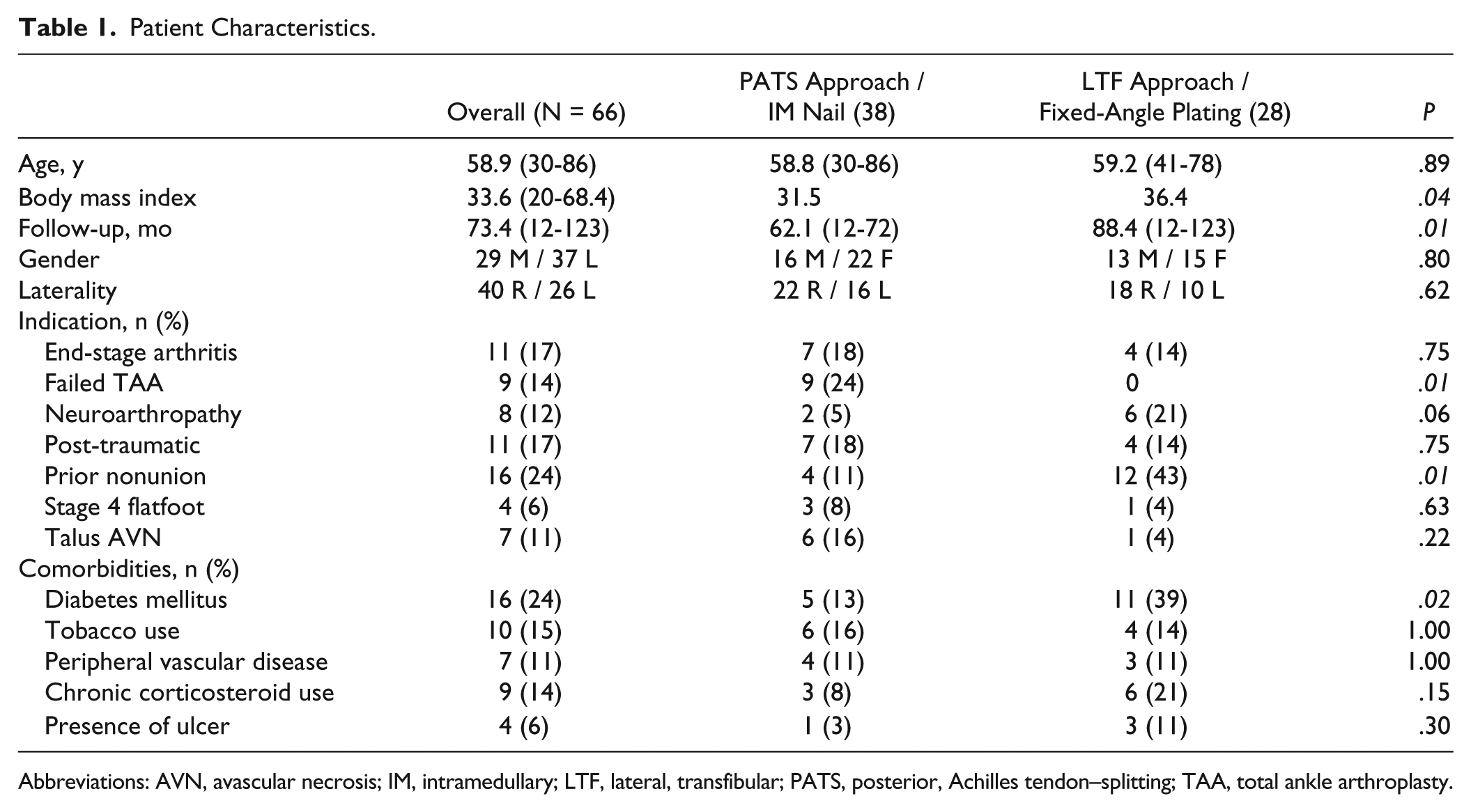
Abbreviations: AVN, avascular necrosis; IM, intramedullary; LTF, lateral, transfibular; PATS, posterior, Achilles tendon–splitting; TAA, total ankle arthroplasty.
Statistical analysis was performed with Student t test for continuous data and chi-square test for categorical variables. P values less than .05 were considered significant.
Operative Technique
For the PATS/IM nailing group, the patient was positioned prone. A straight, midline, full-thickness incision was made and the Achilles tendon split longitudinally with care to not undermine the paratenon or subcutaneous tissue. A Gelpi self-retaining retractor was placed within the Achilles tendon split and the flexor hallucis longus muscle was retracted medially to expose the posterior tibia, talus, and calcaneus. In some instances, the posterior lip of the tibia was resected with an oscillating saw to increase visualization of the TT and ST joints (Figure 2). With the assistance of a pin distractor or lamina spreader, the articular surfaces of both joints were prepared using osteotomes, curettes, or a burr to remove any cartilage and debris. Care was taken to remove any nonviable bone, especially in cases of avascular necrosis of the talus when a large amount of talar body may be excised. In some instances, a large void remained. The remaining subchondral bone was then prepared by making multiple drill holes. At the surgeon’s discretion, depending on the defect size, deformity, risk of nonunion, and quality of bone in the prepared surfaces, cancellous allograft cancellous bone chips, a complete or contoured femoral head, and/or orthobiologic products including recombinant bone morphogenetic protein–2 (Infuse, Wright Medical, Memphis, TN) was placed (Table 2).
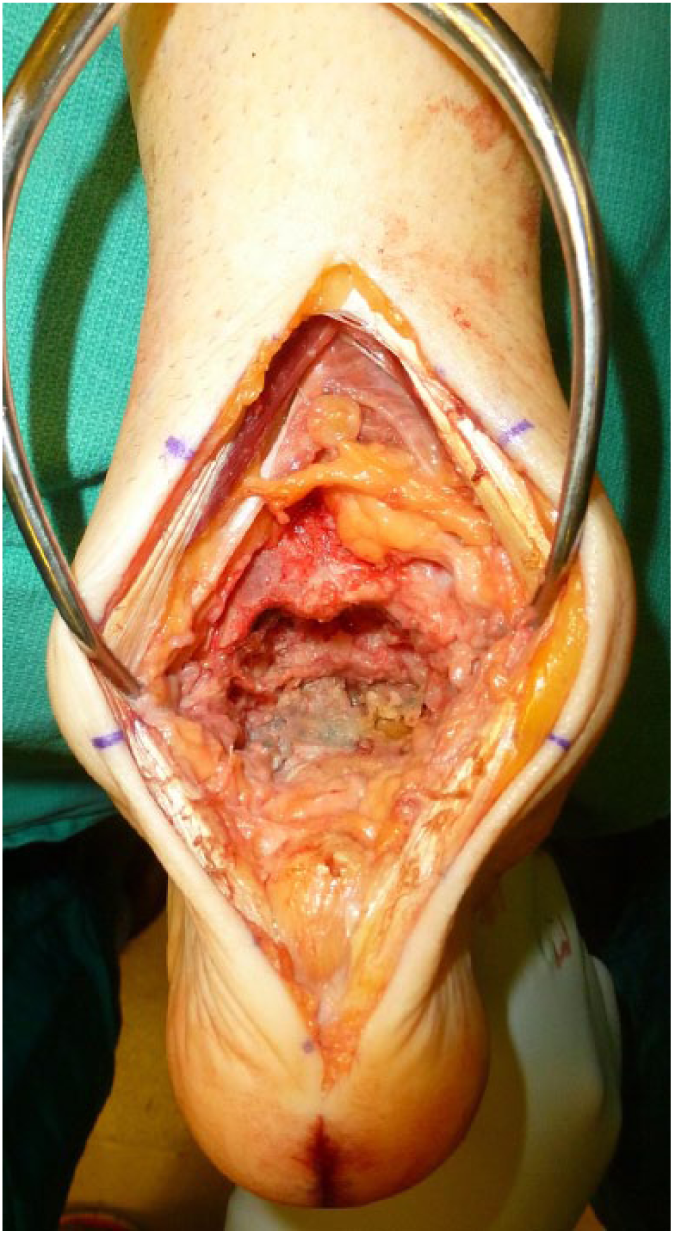
Posterior, Achilles tendon–splitting (PATS) approach: Visualization of the ankle and subtalar joints following removal of a total ankle prosthesis from the PATS approach.
Operative Details. a
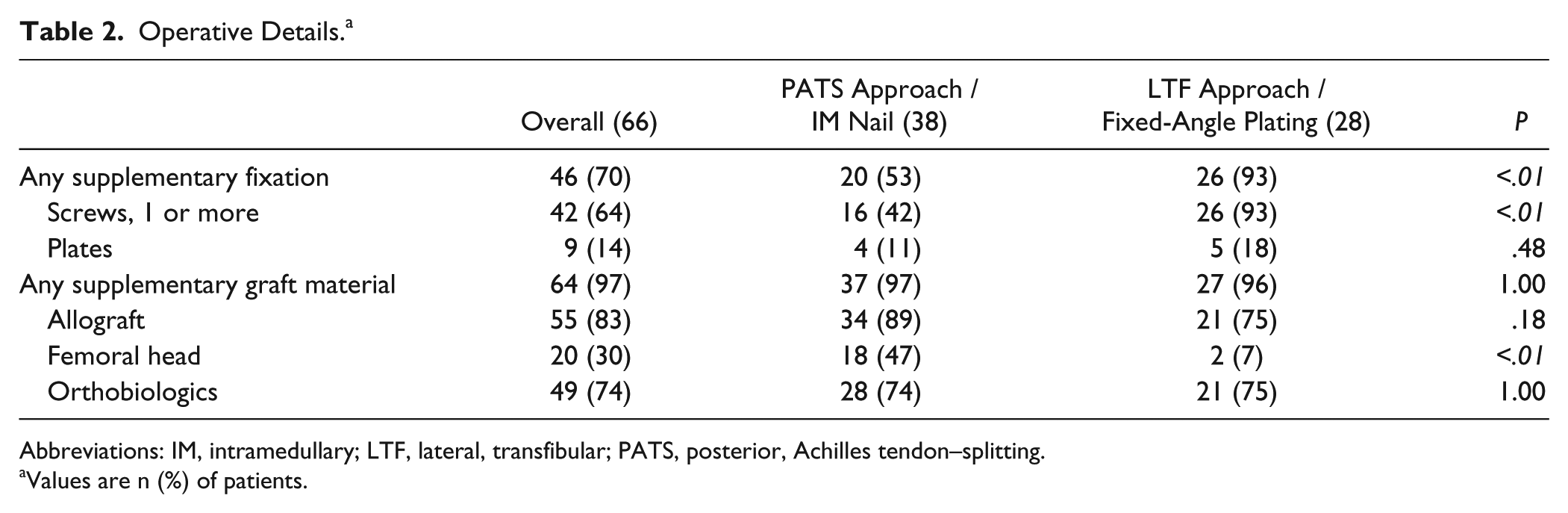
Abbreviations: IM, intramedullary; LTF, lateral, transfibular; PATS, posterior, Achilles tendon–splitting.
Values are n (%) of patients.
The foot was then positioned appropriately, with a goal of 5 degrees hindfoot valgus, neutral to slight external rotation, and neutral dorsiflexion. Steinmann pins were used to temporarily hold the position. A retrograde intramedullary nail was then placed according to the manufacturer’s guidelines. Choice of nail was left to the surgeon’s discretion, and compression was applied across the joint surfaces with nail placement. (Figure 3) The Panta nail (Integra Life Sciences, Plainsboro, NJ) was used in 34 patients (89%), the A3 Fusion nail (Small Bone Innovations/Stryker, Mahwah, NJ) in 2, and the Trigen Hindfoot Fusion nail (Smith & Nephew, Memphis, TN) and Dynanail (Medshape, Atlanta, GA) in 1 each. In some instances supplementary fixation was applied at the surgeon’s discretion, but was unrelated to quality of nail fixation and purely due to surgeon preference (Table 1).

Intramedullary nail with supplementary fixation. Final postoperative lateral radiograph with fused tibiotalar and subtalar joints using an intramedullary nail and additional screw fixation.
For the LTF approach, fixed-angle plating group, the patient was positioned lateral with a bean bag. A curvilinear incision was made approximately 10 cm above the ankle joint in line with the fibula extending distally toward the cuboid. A more straight incision was made in those with significant deformity and potential for wound healing problems. The fibula was exposed entirely and osteotomized in an oblique fashion 6 to 8 centimeters above the ankle joint (Figure 4). In most cases, the bone was morselized for cancellous autograft, but in 2 instances was fixed laterally as an additional strut support at the end of the case. The TT and ST joints were exposed, prepared, grafted, and temporarily fixed in a similar manner as described previously.

Lateral, transfibular approach. Visualization of the ankle and subtalar joints following a lateral approach and fibular osteotomy.
A lateral, fixed-angle plate was then applied according to the manufacturer’s guidelines. Twenty-one (75%) patients received an Integra Advansys plate (Integra Life Sciences, Plainsboro, NJ) and 7 (25%) received a Synthes 90-degree blade plate (DePuy Synthes, West Chester, PA). Compression across the joint surfaces was applied both manually and with screw placement eccentrically in the oblong holes of the plate. Locking screws were placed after compression if possible on the implant. Similar to the other group, supplementary fixation was performed at the surgeon’s discretion (Figure 5).

Lateral, fixed-angle plate with supplementary fixation. Final postoperative lateral radiograph with fused tibiotalar and subtalar joints using a lateral, fixed-angle plate with locking screws and supplementary screw fixation.
In both groups, a deep drain was placed for 24 hours and the wound was closed in layers. The patient was immobilized in a well-padded, short-leg splint and remained nonweightbearing. At 3 weeks postoperatively, they were transitioned to a cast, remaining nonweightbearing. If simulated weightbearing images at 6 weeks revealed maintained alignment, intact hardware, and early bone healing, the patient was allowed to begin partial weightbearing in a removable boot. However, initiation of weightbearing and transition out of a cast was entirely based on surgeon preference, and varied between surgeons (mean 12 weeks; range 5-28 weeks). Extended periods of casting and nonweightbearing were present in those with delayed or nonunion. Follow-up continued at frequent intervals until 1 year after surgery, at which point patients followed up annually.
Results
Forty-seven of 66 patients went on to union after an initial attempt at arthrodesis, an overall rate of 71%. Union rate in the PATS group was 76% compared with 64% for the LTF group (P = .41). Seven isolated TT nonunions and 2 combined TT and ST nonunions were seen in the PATS group. Six TT and 1 ST nonunion were present in the LTF group, but there were 3 tibiocalcaneal (TC) nonunions in patients, with most of the talar body resected in the LTF group as well. The other 6 patients who had a TC arthrodesis in this group went on to union. There were 2 patients in PATS group with TC arthrodesis and both went on to union as well (P = 1.00).
Symptomatic nonunion that required revision arthrodesis was present in 6 patients in the PATS group (2 combined TT/ST and 4 TT) and 2 patients in the LTF group (both TT) (P = .45). In all cases, the nonunion was debrided, additional grafting was performed, and the hardware revised. Seven of 8 symptomatic nonunions that underwent subsequent revision went on to union, with 1 electing for amputation, discussed below. Elective hardware removal was performed for painful, prominent screws or plates in 3 of the PATS group and 5 of the LTF group (P = .27). There were 2 tibial stress fractures at the proximal end of the nail or plate in each group (P = 1.00), and all went on to heal without operative intervention.
Each group had 4 episodes of superficial wound breakdown and cellulitis treated with local wound care and oral antibiotics (P = .71). There were 2 episodes of deep hardware infection, both in the LTF/plating group (P = .19). One patient dehisced the lateral wound and was treated with irrigation and debridement and intravenous antibiotics. Subsequently, the hardware was removed and free tissue flap was placed, but the arthrodesis sites went on to union. The other patient developed an infected TT nonunion that was treated with irrigation and debridement, hardware removal, intravenous antibiotics, and subsequent revision arthrodesis that went on to complete union. There was an amputation in each group as well. One patient in the PATS group had persistent nonunion of the tibiotalar and subtalar joints following revision and elected for below knee amputation. The other patient in the LTF group developed an infected heel ulcer over 1 year after surgery and complete union, but failed conservative operative measures and elected for a below-knee amputation. Finally, there was 1 instance of sural nerve irritation in the LTF group, but no nerve irritations in the PATS group (P = 1.00).
Twenty patients (30%) necessitated a femoral head structural allograft due to bone loss. This technique was utilized in 18 patients in the PATS/IM nailing group, significantly more often than the LTF, plating group (P < .01) (Table 1). Sixteen of the twenty (75%) went on to union, which was not significantly different from the remaining cohort (P = .77). Three nonunions occurred in the PATS/IM nail group, and 1 in the LTF/plate group (P = .37). At the most recent follow up, 54 of 66 patients (82%) had gone on to union including revision arthrodeses, 10 (15%) had a relatively painless, stable, braceable ankle despite nonunion, and 2 had an amputation.
Post hoc power analysis revealed an estimated power of 0.19, based on our available numbers, to detect a difference in union rate between the PATS/IM nailing and LTF/plating groups. In order to repeat the study with a power of 0.8, a cohort of more than 450 patients would be necessary.
Discussion
Comparison of TTC arthrodeses performed with different approaches and fixation strategies is a difficult task, but we sought to compare the most common methods utilized by our group to assist in decision making when either could be performed. On occasion, approach and implant choice may be dictated by prior incisions, preexisting hardware, and deformity, but increased complications with either technique may indicate a “preferred” method. Our study found both techniques to be adequate, but was underpowered to determine if a significant difference existed. To our knowledge, this is the first comparison of TTC arthrodesis techniques in the literature despite many case series evaluating each individually.*
The overall radiographic union rate in our cohort was 71%; 76% in the PATS group and 64% in the LTF group. Symptomatic nonunion requiring reoperation was less frequent in both groups; 16% in the PATS group and 7% in the LTF group. 82% went on to union when subsequent revisions were included. A wide range of union rates have been reported in the literature from 48% to 100%, but comparison to prior studies, even with similar operative technique, is difficult due to definition of union (radiographic or clinical), inclusion or exclusion of medical comorbidities and complexity of indication.† More than half of our cohort had a nonunion from previous attempt at TT or ST arthrodesis, had a large void filled with a femoral head allograft, or had avascular necrosis of the talus, which have been shown to increase complexity or have a significantly lower rate of union.7,9,13,23 Additionally, a number of our patients had diabetes, peripheral vascular disease, chronic steroid use, presence of ulcers, or were tobacco users. Despite numerous risk factors, our union rate is within range of those previously reported, and 64 of 66 (97%) patients had a stable, braceable ankle at final follow-up.
Although union may be considered the most important outcome, each method confers other potential benefits. The PATS approach allows for a robust soft tissue envelope, preservation of the natural angiosomes.43,48 Four of 38 patients had some mild superficial wound breakdown and cellulitis that cleared with wound care and antibiotics, which is within range of previously reported rates of 5% to 13.3% with the posterior approach.1,7,8,38,40 In our hypothesis we proposed the PATS approach would confer a lower wound complication rate than the LTF approach, but they turned out to be similar. In cases of severe deformity, wound healing issues are known to occur with the lateral approach. 33 There were only 4 episodes of minor wound complications and 2 deep infections in this group, which was not significantly more than the PATS group. Because nearly one-quarter (6 of 28 patients) in the LTF/plating group had an infection (superficial or deep), we continue to recommended alternate approaches in cases with prior lateral incision or significant deformity.
The TT and ST joints were easily accessed for preparation with the PATS approach, although the literature would suggest the talar joint surfaces are more accessible from a lateral, transfibular approach. 41 Additionally, the posterior approach allows for sparing of the fibula and disruption of blood supply critical to healing the arthrodesis sites. Preserving of the lateral strut may prevent valgus drift over time as well. We did not see any expected benefit, as stated in our hypothesis, by avoiding a fibular osteotomy. Future studies with pre and postoperative hindfoot alignment views may elicit benefits in short and long term coronal plane deformity correction.
The LTF approach similarly allows for easy access to the TT and ST joints, but requires osteotomy of the fibula. Fixed-angle plating for TTC arthrodesis is less described in the literature, but success has been reported with blade plating and a variety of locking plates.2,12,15,21,22,26 Although more exposure is required for application, this approach and fixation technique allow for quick, direct access and fixation. Although not examined in this study, this method may decrease the operative time. Cortical stress reactions or fractures at the proximal aspect of the nail and soft tissue or neurovascular injury at the nail insertion site are potential complications of IM TTC nails.46,47 Two stress fractures were seen in the PATS/IM group that went on to heal without operative intervention; however, 2 stress fractures were observed in the LTF group as well.
Although this study compares one approach and fixation strategy with an entirely different approach and fixation technique, these could certainly be interchanged after consideration of the biomechanical properties. A number of studies have compared the biomechanical properties of IM nails and fixed-angle plates for TTC arthrodesis.* In a cadaveric study, Chiodo et al noted biomechanical superiority with a blade plate and screw construct when compared to IM nail with high initial and final stiffness and less plastic deformation after cyclic loading of paired specimens. 10 In a similar cadaveric model, a locking plate construct was compared with an IM nail, and the IM nail final rigidity was inferior to that of the locking plate. 36 Others have been unable to reproduce these findings and found similar biomechanical properties between IM nails, blade plates, and locking plates.3,18,35 Additionally, in the setting of TC arthrodesis (with complete talectomy), Lee et al found the IM nail to be superior to blade plating in a cadaveric study. 25 Chodos et al compared locking plates to blade plates and suggested superiority of the locking plate with higher initial stiffness, and higher dorsiflexion and torsional load to failure. 11 Our study included 21 locking plates and 7 blade plates. Although the differences in biomechanical properties of IM nails are unclear compared to fixed-angle plates, addition of an augmentation screw 37 and use of posterior to anterior distal screws within the nail provide more stable fixation.28,29 Most nails in our series utilized 2 posterior-to-anterior distal screws and more than half received some form of supplementary fixation. Significantly more patients in the LTF/plating group received supplementary fixation, so this may affect a comparison of union rates.
Nearly every patient in our study received supplemental graft material in their arthrodesis. Most had allograft bone (cancellous chips or femoral head structural graft) and many received orthobiologic material (Infuse) that not only provided a matrix for bone healing but growth factors and stem cells. Although Infuse is not approved for TTC arthrodesis by the Food and Drug Administration, promising results have been reported in ankle and hindfoot surgery.5,14 Structural femoral head allograft and bulk allograft cancellous bone chips are commonly used in the setting of large defects, and despite lower reported union rates, they likely provide a chance at union that otherwise would not be possible.9,13,23 We had a union rate of 75% with femoral head allograft, higher than previously reported. Most (18 of 20) of the femoral head allografts were used in the PATS/IM nail group, so a benefit of the PATS approach and IM nailing may be increased union in patients requiring bulk structural allograft—a group previously found to have a nonunion rate greater than 50%. 23 Because most patients received at least 1 type of supplemental graft or in many cases a combination of graft materials, this study was not powered to elicit differences.
We acknowledge there are some limitations to this study. Despite their indication for TTC arthrodesis, the patient groups are not homogenous with regard to some patient characteristics that could increase risk for complications. Patients in the LTF group were heavier (body mass index 36.4 vs 31.5), and more likely to be diabetic. No patients in the LTF group had a large void to be filled from failed TAA versus 9 in the PATS group, and there were significantly more (12 vs 4) nonunions of prior arthrodeses in the LTF group. Additionally, this was a retrospective study, so operative techniques including implant choice, supplementary fixation, adjunctive grafting, and postoperative protocols were at the surgeon’s discretion. Radiographic imaging was used to assess union unless a CT scan was available, which was the case in only 44%. CT scan is particularly important when bulk allograft is used because a tight fit may be mistaken for union on plain radiographs. Because some did not have a CT scan available to reveal appropriate osseous bridging, our union rate may have been overestimated. However, our overall union rates are within range of those previously reported, which often only utilized radiographs. Many of these patients were treated prior to incorporation of a hindfoot alignment x-ray view as part of our standard ankle radiograph series with pre- and postoperative evaluation; therefore, we were unable to reliably assess any coronal plane malalignment on imaging. Our group now routinely uses a hindfoot alignment view, and CT scans are performed 6 to 12 months after surgery to assess for union.
Another limitation of our study was the inability to detect a significant difference in union rate based on a calculated power of 0.19. Although outcomes appeared similar, a sample size large enough to demonstrate a significant difference from a single institution was difficult to achieve despite the inclusion of 4 high-volume foot and ankle orthopedic surgeons. However, our results show successful outcomes in a large cohort, despite difficult patient and operative factors, with either treatment technique.
In conclusion, we demonstrated acceptable union rates, despite a complex patient mix, using 2 different TTC arthrodesis techniques. Although underpowered, no difference was seen with regard to union or complications, and one can feel confident with either technique, especially if prior incisions, preexisting hardware, or deformity preclude one or the other. Multicenter studies and additional comparison of functional outcomes and cost-effectiveness may further elicit the best answer to this problem.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.