
Abstract
Background:
The visual analog scale (VAS) is considered a reliable and validated measure of patient-reported acute pain. Patient-reported outcome measures are becoming the standard of care throughout the orthopedic community, but interpretation and clinical applications are still under investigation. The aim of the current study was to compare preoperative patient-reported VAS scores reported at the same visit to nursing staff and the treating surgeon. Our hypothesis was that there would be no difference in the scores reported.
Methods:
This study is a retrospective cohort of 201 consecutive foot and ankle patients treated by a single surgeon. The patients were asked to rate their pain intensity by the nursing staff and then by the surgeon using a standard horizontal VAS 0 to 10, from “no pain” to the “worst pain.” Differences in reported pain values were analyzed.
Results:
The results demonstrate that patients reported higher pain scores to the surgeon in 81% of the encounters, nursing staff 8%, and equal 11%. On average, the VAS score reported to the surgeon was significantly (P < .05) higher than that reported to the nursing staff.
Conclusion:
The current study found a statistically significant higher patient-reported pain score to the treating surgeon compared to the nursing staff. While the exact cause is unclear, the discrepant pain scores call into question the validity of the VAS, considered a fifth vital sign and standard outcome measure in an outpatient clinic setting.
Level of Evidence:
Level III, comparative study.
Introduction
As reimbursements and billing continue to evolve toward a value-based system, patient-reported outcome measures (PROMs) are used to stratify quality of care, physician performance, and value. 1 The visual analog scale (VAS) is a well-known PROM used in orthopedic surgery and is commonly used as a measurement to gauge a treatment’s efficacy in decreasing pain. As PROMs potentially become synonymous with the standard of care in orthopedic surgery, it is important to balance high-quality care with patient expectations for pain reduction.
The VAS has been shown to be valid in assessing pain in foot and ankle patients. 7 While the VAS maintains its effectiveness as a tool to rate acute pain, the efficacy with use in chronic and postoperative pain has not been validated in an outpatient clinical setting. Regardless of the lack of validation, the Joint Commission on Accreditation of Healthcare Organization (JCAHO) continues to include the VAS as a required assessment (pain considered as the fifth vital sign) in all patients. 6 The VAS is also used as a quality measure contributing to providers’ total care metric, which can be used for accreditation and reimbursement.
The aim of the current study was to evaluate whether the VAS provided preoperatively to 2 different health care personnel, a nurse and physician, respectively, was the same or different during a single encounter in the orthopedic outpatient clinic. We hypothesized that there would be no difference in scores reported to either of the health care professionals.
Methods
The current study was a retrospective cohort of 201 consecutive operative foot and ankle patients treated by a single orthopedic surgeon. The cohort consisted of elective and subacute trauma. All urgent and emergent cases were excluded, as were non–foot and ankle cases. In our facility, new referrals were seen within 30 days, but pain chronicity was difficult to assess and outside the scope of the current study. The patients were taken to their patient room and asked by the nursing staff to rate their pain intensity using a standard horizontal VAS 0 to 10, from “no pain” being a “0” labeled with a “smiley face” to the “worst possible pain” being a “10” labeled with a “sad face.” At the same office visit, within 1 to 5 minutes, the patients were asked by the treating surgeon to rate their pain using the same VAS. The patients were asked to rate their pain in the outpatient setting on the first encounter and prior to any nonoperative or operative treatment being discussed. Patients were first interviewed by the nursing staff and then by the physician. When interviewed by the physician, the VAS pain scale was performed prior to the physical examination.
In total, 201 consecutive patients presenting to the orthopedic clinic with foot and ankle pain participated in this study, providing 402 VAS scores, with 2 reported scores per patient per visit. Participants reported 1 score to the nurse and then, within 1 to 5 minutes, reported to the treating surgeon during the same office visit. Of these 201 patients, 33% (66) were females and 67% (135) were males of varying ages.
Dependent t tests were calculated to evaluate mean differences in VAS pain reported by each patient to 2 different health care professionals during a single outpatient clinic encounter. All data were analyzed using STATA version 10.1 (StataCorp LP, College Station, TX) with an α level of P < .05.
Results
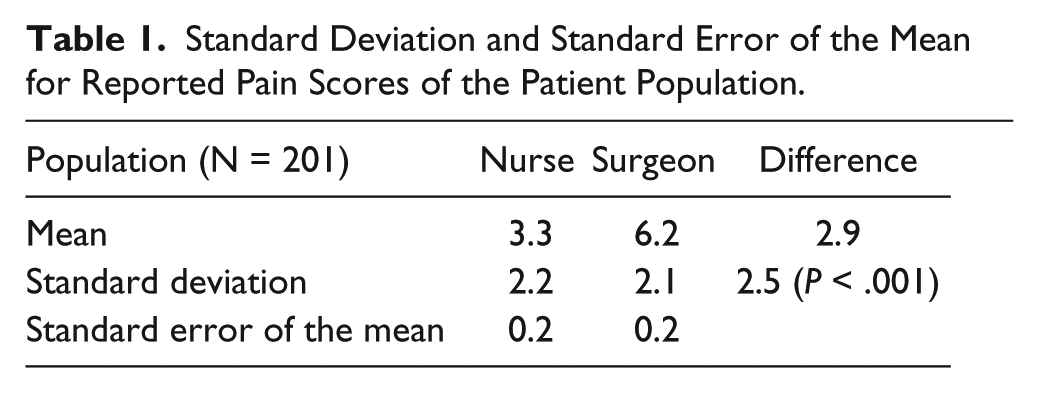
The results demonstrate that patients reported higher pain scores to the surgeon in 81% of the encounters; higher pain scores were reported to the nursing staff in 8% of the encounters and scores reported as equal between the nurse and surgeon in 11% of the encounters. On average, the VAS score reported to the surgeon (6.2 ± 2.1) was significantly higher than that reported to the nursing staff (3.3 ± 2.2), respectively (Table 1). The mean difference between the scores was 2.9 ± 2.5 (P < .001). Table 1 and Figure 1 illustrate the frequency with which each pain score was reported to the nurse (solid) compared to the surgeon (diamond), showing patients reported higher pain scores to the surgeon.
Standard Deviation and Standard Error of the Mean for Reported Pain Scores of the Patient Population.
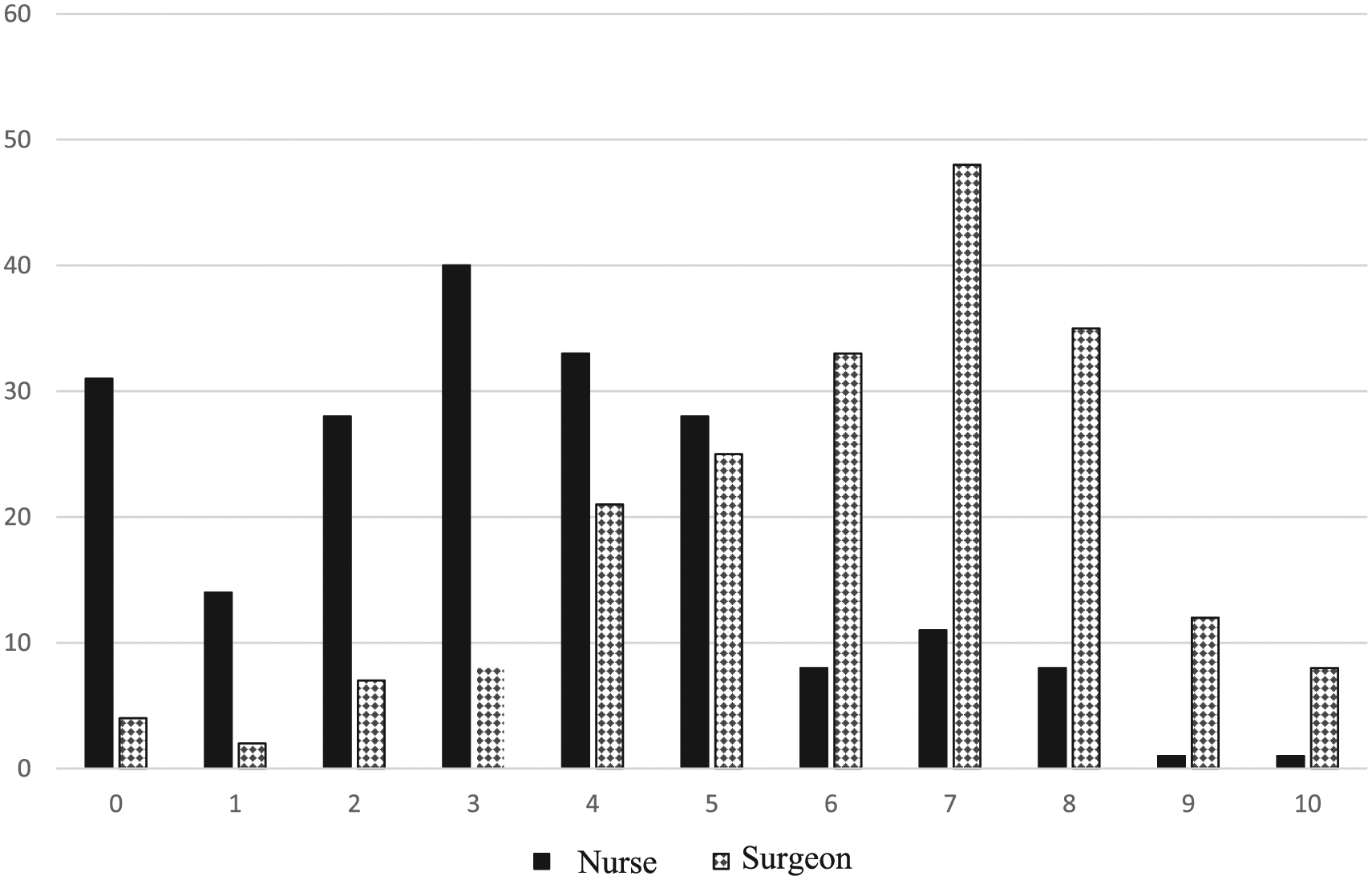
Reported pain scores to nursing staff vs treating surgeon in aggregate. Pain reported is on the x-axis and number of total patients reporting each score is on the y-axis. Reports to nurses are represented by solid black while the diamond lines represent reports to the surgeon.
Discussion
In this study, we found that first-encounter patients in the foot and ankle outpatient orthopedic surgery setting frequently report a statistically higher VAS to the surgeon compared to the nursing staff. Patients rated their pain higher to the surgeon 81% of the time, with the mean difference in scores reported to the surgeon vs the nursing staff being close to 3 raw points on the 11-point scale, from 0 to 10. With an average reported pain score of 6.2 (physician) and 3.3 (nurses), the physician’s average scores were 1.9 times higher than the average nursing score. This represents a significant increase in scores reported to the physician vs the nurse. These results are in direct contrast to our hypothesis that patients would report the same subjective pain score to the nursing staff and treating surgeon.
Upon review of the literature, to our knowledge, there is no previous study comparing VAS pain scores reported to 2 different providers at the same clinical visit. Most studies in foot and ankle research use pain VAS to focus on evaluating interventions and their effect on pain.3,8 However, prior studies have investigated the temporal relationship of the VAS and its test-retest reliability but not in the same visit. One study measured anxiety scores on a VAS, obtained 6 months apart, without mention as to whether the same provider obtained both scores. 5 Another study used anxiety and pain VAS in a pediatric population in the perioperative setting after elective surgeries. 2 While pain scores were not directly compared to each other over time, a positive correlation was found between anxiety and pain, but it is unclear if the instrument was implemented by the same type of provider (ie, nurse vs physician). Test-retest has also been used in pain VAS. Patients with acute abdominal pain were evaluated using a pain VAS in the emergency department at 0 and 1 minutes and then at 30-minute increments for 2 hours. 4 While it is unclear if the scales were administered by the same type of health care provider, this study found that there was significant correlation in VAS pain scores reported by the patients during the 2-hour period.
As a study using VAS, the strengths and limitations lie within the scale. Its strengths are its ease of use, low cost, good reliability, validation for pain, and the metric nature of the responses that allow for easy statistical analysis. Limitations lie in the difficulty of transforming a subjective feeling such as pain into a single number as well as using a single item to represent suffering related to pain intensity. Overall, the VAS is the scale of choice for pain, and its strengths far outweigh its weaknesses. Other limitations of the study relate to the personnel who administer the scale. One male orthopedic surgeon administered the testing to all patients, while all nursing testing was performed by female nurses. However, the same female nurse did not administer every test. The implications of sex and its effect on the results are not known. An additional limitation of this study is the unknown chronicity of the subacute patients and the role that this plays in patient VAS pain scores.
To our knowledge, no studies have explored a patient’s current subjective pain reported to different providers in the same visit; therefore, it is difficult to compare our results to similar designs. Our research identified that patients reported statistically significant higher VAS pain scores to the physician. VAS pain scales are considered the standard of care for assessing pain in orthopedic surgery and are being used to determine efficacy of treatment. If a patient under- or overstates his or her pain in the preoperative or postoperative setting, it becomes difficult to trust these measures as a means for assessing the efficacy of surgery at reducing pain. The potential of incorrect pain scores calls into question using these methods as a reliable measure not only for pain but also for other aspects of treatment in the postoperative setting. Tracking the patient’s recovery from surgery, the ability to start and continue physical therapy, and going back to work are areas of the treatment plan that could be affected by unreliable pain scores. While it is clear that patient-reported outcomes preoperatively vary depending on whether the surgeon or nurse asks, future studies could explore whether the same trend is observed in the patients who did not go on to have surgery.
Conclusion
This study demonstrates a clear difference in patient-reported pain scores between those given to nursing staff vs the treating surgeon. While the exact cause is unclear, the discrepant pain scores to the nursing staff and surgeon call into question the validity of the VAS as a reflection of pain as the fifth vital sign in an outpatient clinic setting. These results also further support that patients with varying degrees of acute and chronic pain may have difficulty applying a single numeric value for an extended time period. All surgeons should be aware of the discrepancy as the VAS is often used to assess quality of care and if a particular surgery was successful. Standard measures such as the VAS can be used by insurance companies and regulatory bodies to measure if a provider should be accredited or included in health plans and networks. The VAS has a place evaluating acute pain, but in the outpatient clinical setting, other patient-reported outcome measures might more accurately represent the patient and operative outcomes.
Supplemental Material
FAI740584_-_ICMJE – Supplemental material for Comparison of Visual Analog Pain Score Reported to Physician vs Nurse
Supplemental material, FAI740584_-_ICMJE for Comparison of Visual Analog Pain Score Reported to Physician vs Nurse by Kevin D. Martin, J. Preston Van Buren, Jeffrey Wake, and Laura Dawson, in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.