
Abstract
Background:
Osteochondral allograft (OCA) transplantation is a useful alternative for treatment of posttraumatic ankle arthritis in young patients but has a relatively high failure rate and further procedures are often required. The purpose of this study was to evaluate outcomes of patients who underwent revision OCA transplantation of the ankle after failed primary OCA transplantation.
Methods:
Twenty patients underwent revision OCA transplantation of the ankle between 1988 and 2015. Mean age was 44 years, 55% (11 of 20) were female. The mean time from primary to revision OCA was 3.0 ± 1.7 years. All patients had a minimum follow-up of 2 years. Outcomes included the American Academy of Orthopaedic Surgeons Foot and Ankle Module (AAOS-FAM) and questionnaires evaluating pain and satisfaction. Failure of the revision OCA was defined as a conversion to arthroplasty, arthrodesis, or amputation.
Results:
Ten of 20 ankles required further surgery, of which 30% (6 of 20) were considered OCA revision failures (4 arthrodeses, 1 arthroplasty, and 1 amputation). The mean time to failure was 6.7 (range, 0.6-13.1) years. Survivorship of the revision OCA was 84% at 5 years and 65% at 10 years. The 14 patients with grafts remaining in situ had an average follow-up of 10.3 years; mean AAOS-FAM Core Score was 70.5 (range, 42.3-99). Of the patients who answered the follow-up questions, 4 of 7 reported moderate to severe pain, and 5 of 12 were satisfied with the results of the procedure.
Conclusion:
Although the results of revision ankle OCA transplantation are not inferior to primary OCA transplantation, the high rates of persistent pain, further surgery, and graft failure suggest that the indications for OCA as a revision procedure should be carefully evaluated, with proper patient selection. Considering the treatment alternatives, revising a failed OCA transplantation can be a useful treatment option, especially for young and active patients who wish to avoid arthrodesis or arthroplasty.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
The treatment of posttraumatic arthritis and large osteochondral lesions of the ankle is difficult and remains a challenge for every orthopedic surgeon especially if it affects young and active patients. Several treatment options have been described with different advantages and disadvantages as well as clinical outcomes, ranging from marrow stimulation techniques and autologous chondrocyte implantation (ACI) or osteochondral autograft transfer (OATS)/mosaicplasty for focal lesions to arthroplasty and arthrodesis for severe end-stage osteoarthritis.
Another treatment option is using fresh osteochondral allograft (OCA) transplantation, which represents a biological repair and has been used in a wide variety of indications and different joints. If compared with the abundant clinical data of the knee joint, OCA transplantations of the ankle are less frequent and have generally a higher failure rate and therefore often require further surgery.2,21,25 If a primary ankle allograft fails, options remaining for salvage procedure are limited to arthroplasty, arthrodesis, or revision OCA transplantation. However, the available literature regarding these procedures is extremely rare, when most current publications are focused either on arthrodesis as a salvage procedure after primary failed ankle arthroplasty or after non-union of primary arthrodesis.5,16,20,22 The only currently existing publication regarding outcome data after osteochondral allografting as a revision procedure was done analyzing the knee joint. 11 This study of 33 patients with a mean follow-up of 10 years showed a revision OCA failure rate of 39%, a mean time to failure of 5.5 years, and a graft survival of 61% at 10 years.
Although the general clinical outcome data after osteochondral allograft of the ankle is limited and most publications are focused on primary procedures, the purpose of our study was to evaluate the outcomes of patients who underwent revision osteochondral allograft transplantation of the ankle after primary failed OCA transplantation.
Methods
Between July 1986 and June 2008, our institutional review board–approved osteochondral allograft transplantation outcomes program collected data of 175 patients who underwent primary OCA transplantation of the ankle (130 bipolar OCA, 31 partial talus, 14 partial bipolar or unipolar). All patients gave informed consent to participate in the outcomes database. We identified allograft failures in 56 cases, of which 52 patients underwent a salvage procedure. Between June 1988 and January 2015, 22 of these patients (22 ankles) had a revision OCA transplantation. Two patients were excluded from our analysis because 1 had a follow-up duration less than 2 years and 1 patient refused to participate. Indications for revision OCA included allograft failure, avascular necrosis, or traumatic arthritis. Of the 20 patients included in our analysis, the mean time from primary OCA transplantation to revision surgery was 3 ± 1.8 (range, 1-6.6) years. The mean age at the time of the revision was 44 ± 15 (range, 20-70) years, the mean BMI was 30 (range, 27-36) and 11 of 20 patients (55%) were female (Table 1). Of the 20 patients, 16 (80%) received a bipolar allograft at the time of revision, 2 (10%) received a unipolar tibia allograft, 1 (5%) received a unipolar talus allograft, and 1 (5%) received a partial talus allograft (Figure 1).
Patient Characteristics of 20 Revision Ankle OCA. a
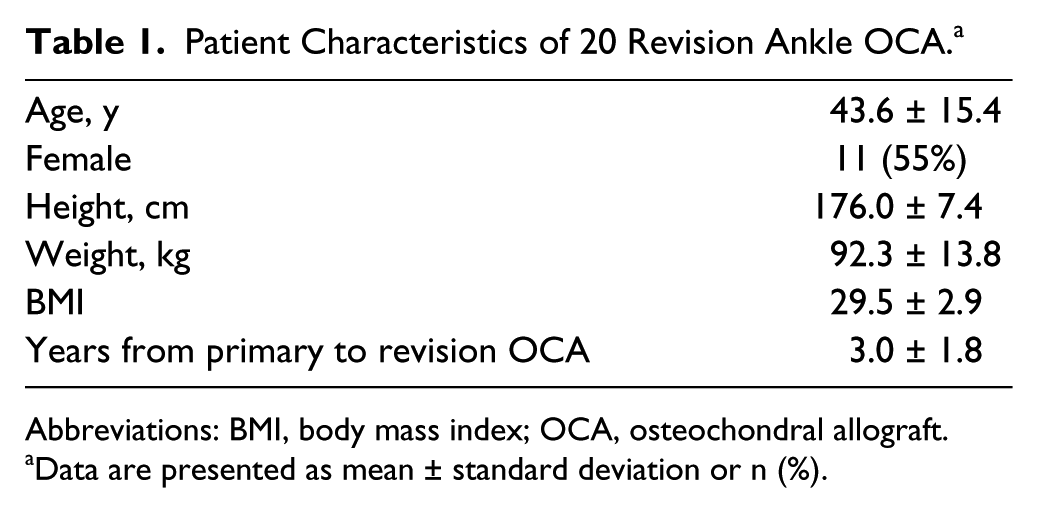
Abbreviations: BMI, body mass index; OCA, osteochondral allograft.
Data are presented as mean ± standard deviation or n (%).
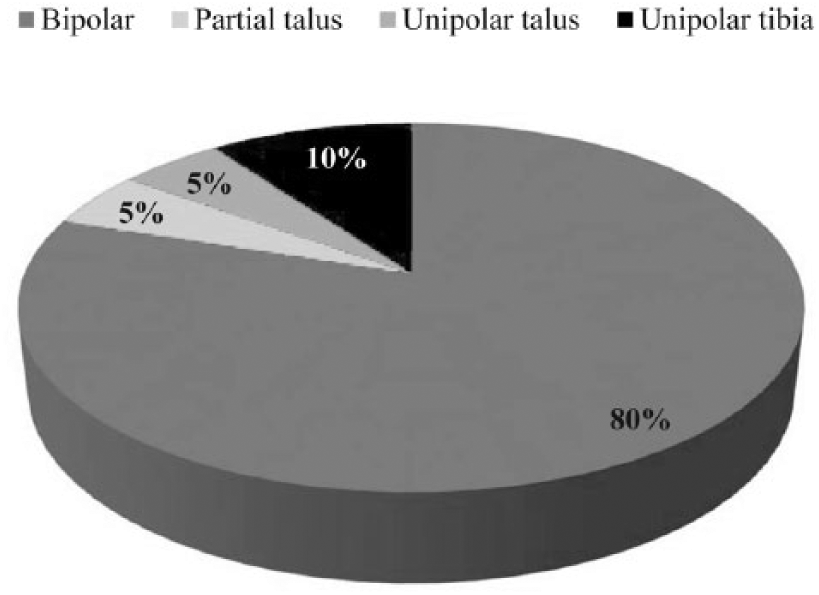
Graft types used for 20 revision ankle osteochondral allograft transplantations.
All patients were contacted via telephone or mail and asked to complete a questionnaire evaluating the level of pain (numeric rating scale, NRS), satisfaction, and whether or not they had undergone further surgery on their ankle following the revision allograft transplantation. Revision OCA failure was defined as a further surgery that involved removal of the allograft, such as conversion to arthrodesis, total ankle arthroplasty, or below-knee amputation. Patients were also given the Foot and Ankle Module (AAOS-FAM) outcome questionnaire developed by the American Academy of Orthopaedic Surgeons (AAOS). 14 This patient-reported assessment outcome tool consists of 5 subscales: pain (9 questions), function (6 questions), stiffness and swelling (2 questions), giving way (3 questions), and shoe comfort (5 questions). In our study, we only used the Core Scale which excludes the shoe comfort scale. The final standardized score ranged from 0 to 100 points, with the lower the score, the greater the disability. Furthermore, based on a general reference population of the United States, the AAOS normative scores were calculated from the standardized values using the online available worksheet provided by the AAOS (www.aaos.org/research/outcomes/Foot_AnkleScoring.xls). If a patient scored above 50 points, it meant he or she was above the general, healthy population’s average score (and vice versa).
Surgical Procedure
All fresh osteochondral allografts were obtained from a bone bank that was certified by the American Association of Tissue-Banks. Prior to implantation, no human leukocyte antigen (HLA) matching was performed. The graft was recovered within 1 day after the donor death, was never frozen, and was stored at 4°C until transplantation. As described previously, all patients were operated under temporary distraction using a direct anterior approach through the interval between the extensor hallucis longus and the tibialis anterior. 9 After assessing the tibiotalar joint, the affected area of the talar dome and distal tibia were marked and resected using an oscillating saw. Most revisions involved placement of both tibial and talus grafts utilizing the primary bipolar ankle allograft technique that has been previously described.4,9 As much native bone stock as possible was preserved to minimize the amount of transplanted allograft bone. In case of cystic lesions extending beyond the depth of a resection level, curettage and autologous bone grafting was performed. Sclerotic bone was drilled to enhance integration of the graft. Based on measurements of the resected talar dome, the allograft was prepared using a free hand technique with an oscillating saw. Prior to implantation, the graft underwent pulse lavage with normal saline to remove debris and marrow elements. The correct position of the graft and the exact restoration of the talar dome was confirmed fluoroscopically in both planes. Before removing the external distractor, the graft was fixated with absorbable pins, a cannulated screw, or a combination of both (Figure 2).
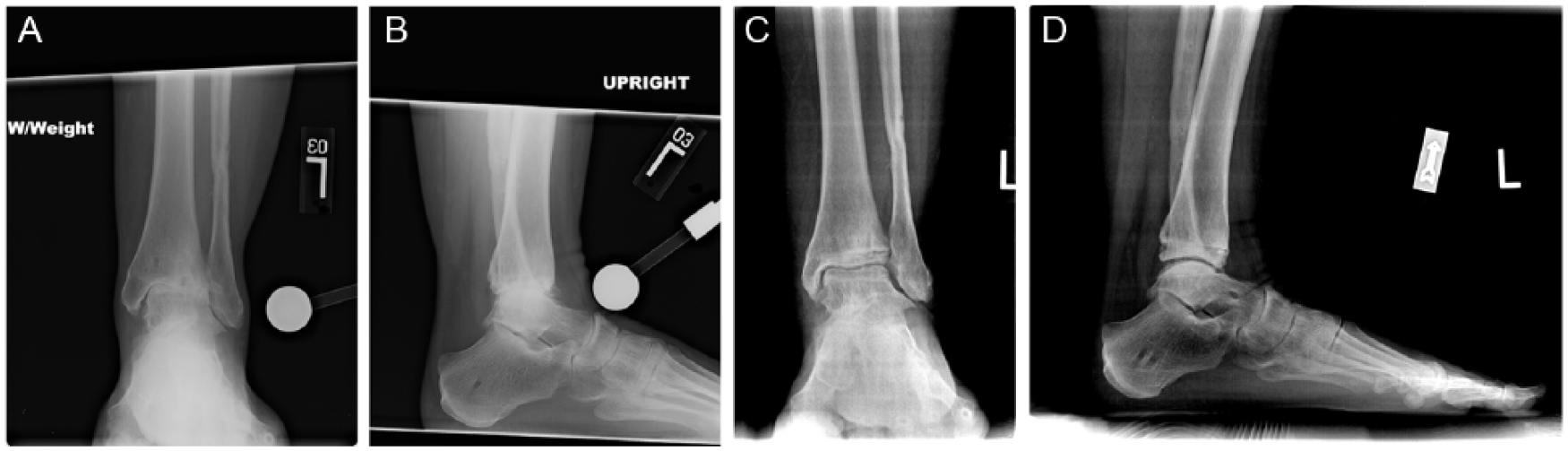
(A) Preoperative anteroposterior ankle radiograph of a 35-year-old woman showing complete joint space loss. (B) Preoperative lateral radiograph of same ankle. (C) Postoperative (1 year) anteroposterior ankle radiograph of the same patient after revision bipolar ankle allograft transplantation. Note the osseous incorporation of allografts and re-creation of joint space. (D) Postoperative lateral radiograph of same ankle.
Postoperative Care and Rehabilitation
All ankles were protected in a splint until removal of the sutures at 2 weeks, followed by transition to a controlled ankle motion (CAM) walker to permit early ankle motion exercises. Patients were strictly non-weight-bearing for 6 to 8 weeks and then progressed to partial weight bearing (25% to 50% of body weight) in the CAM walker, with functional rehabilitation for a period of at least 6 weeks. A gradual return to full weight bearing was permitted once graft incorporation was confirmed radiographically, usually at 12 weeks.
Statistical Analysis
All statistical analyses were performed using SPSS version 13.0 (SPSS Inc, Chicago, IL). Means and frequencies were calculated to summarize patient characteristics (age, sex, body mass index, and number of previous surgeries on operated ankle), allograft details (time from primary to revision allograft, type of allograft, and size), and data regarding number and type of further surgeries following the revision OCA transplantation. The Kaplan-Meier method was used to compute survivorship with failure of the revision OCA (further surgery that involved removal of the allograft) as the endpoint. Among patients whose grafts remained in situ at latest follow-up, means and frequencies were used to summarize follow-up data (NRS for pain, satisfaction, AAOS-FAM core and normative scores). A subgroup analysis was performed among bipolar grafts only, which represented the majority of cases (80%; 16 of 20 knees).
Results
Among the 20 patients undergoing revision OCA transplantation, further surgeries were required in 10 ankles (50%) (Table 2). Failure of the revision OCA occurred in 6 of 20 ankles (30%), which included conversion to arthrodesis (4 ankles), total ankle arthroplasty (1 ankle), and below-knee amputation (1 ankle). The mean time to failure of the revision allograft was 6.7 (range, 0.6-13.1) years. Survivorship of the revision OCA transplantation was 84% at 5 years (95% CI: 0.598, 0.954) and 65% at 10 years (95% CI: 0.411, 0.838) (Figure 3).
Reoperations Following Revision Ankle OCA.
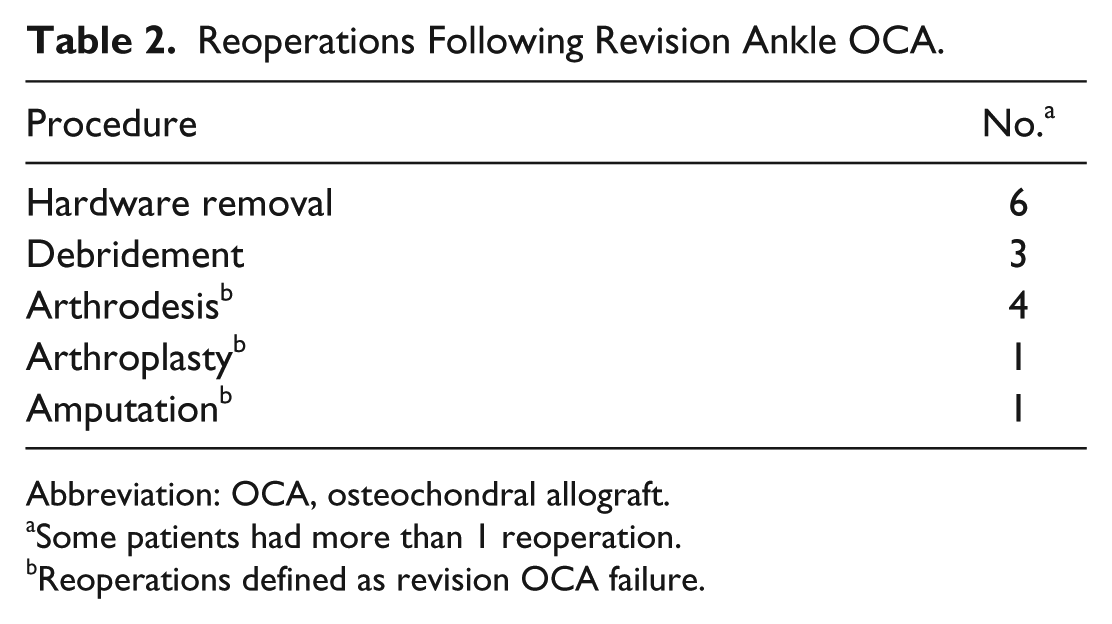
Abbreviation: OCA, osteochondral allograft.
Some patients had more than 1 reoperation.
Reoperations defined as revision OCA failure.
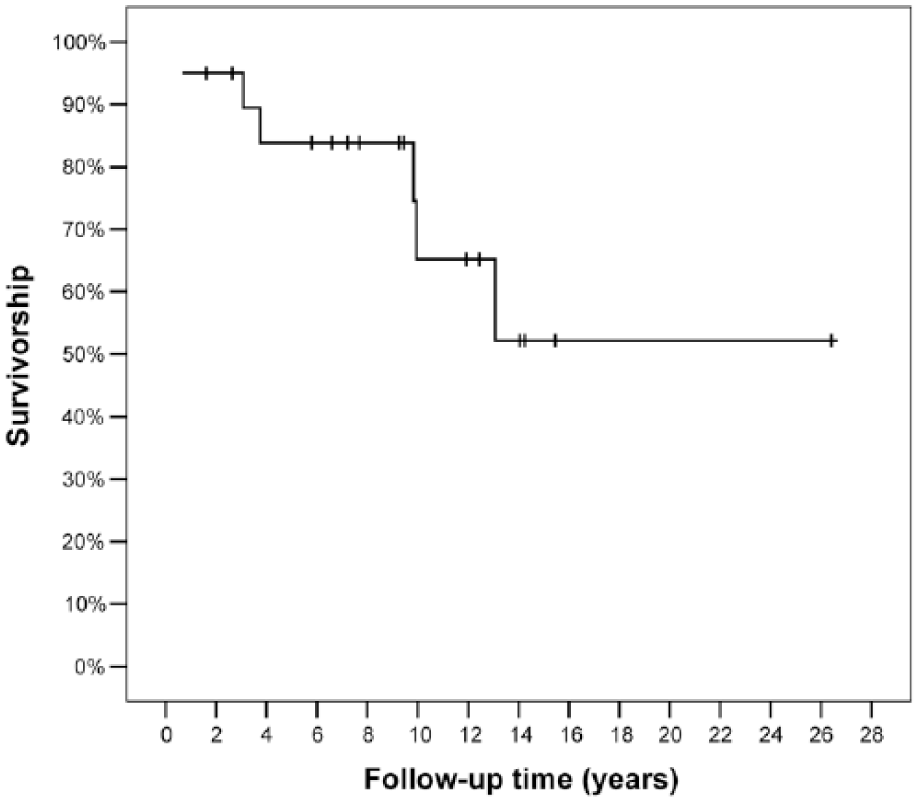
Survivorship of revision osteochondral allograft transplantation was 84% at 5 years (95% confidence interval [CI]: 0.598, 0.954) and 65% at 10 years (95% CI: 0.411, 0.838).
The mean follow-up duration among the nonfailed OCA transplantations (n = 14) was 10.3 ± 6.3 (range, 1.6-26.4) years. Half of the patients (7 of 14) answered the question regarding their level of pain on the NRS at the time of the latest follow-up: 1 patient reported no pain (NRS 0), 2 patients reported mild pain (NRS 1-3), 3 patients reported moderate pain (NRS 4-6), and 1 patient reported severe pain (NRS 7). The mean level of pain was 3.7 on the NRS. Of the 12 patients who answered the question regarding their satisfaction at the time of the latest follow-up, 7 patients were satisfied with the results of their revision ankle OCA transplantation (responding either satisfied or extremely satisfied). Of the 8 patients who answered the question regarding problems with their ankle, 5 patients reported experiencing a problem since the revision OCA (eg, pain, swelling, stiffness, or loss of range of motion). Among the 10 patients who completed the questionnaire at the latest follow-up, the mean standardized AAOS-FAM Core Score was 70.5 ± 17 (range, 42.3-99) and the mean normative score was 31.6 ± 13.8 (range, 8.8-54.7). Data for all 20 patients are presented in Table 3.
Demographic, Surgical, and Outcome Data Among 20 Revision Ankle OCA Transplantations. a
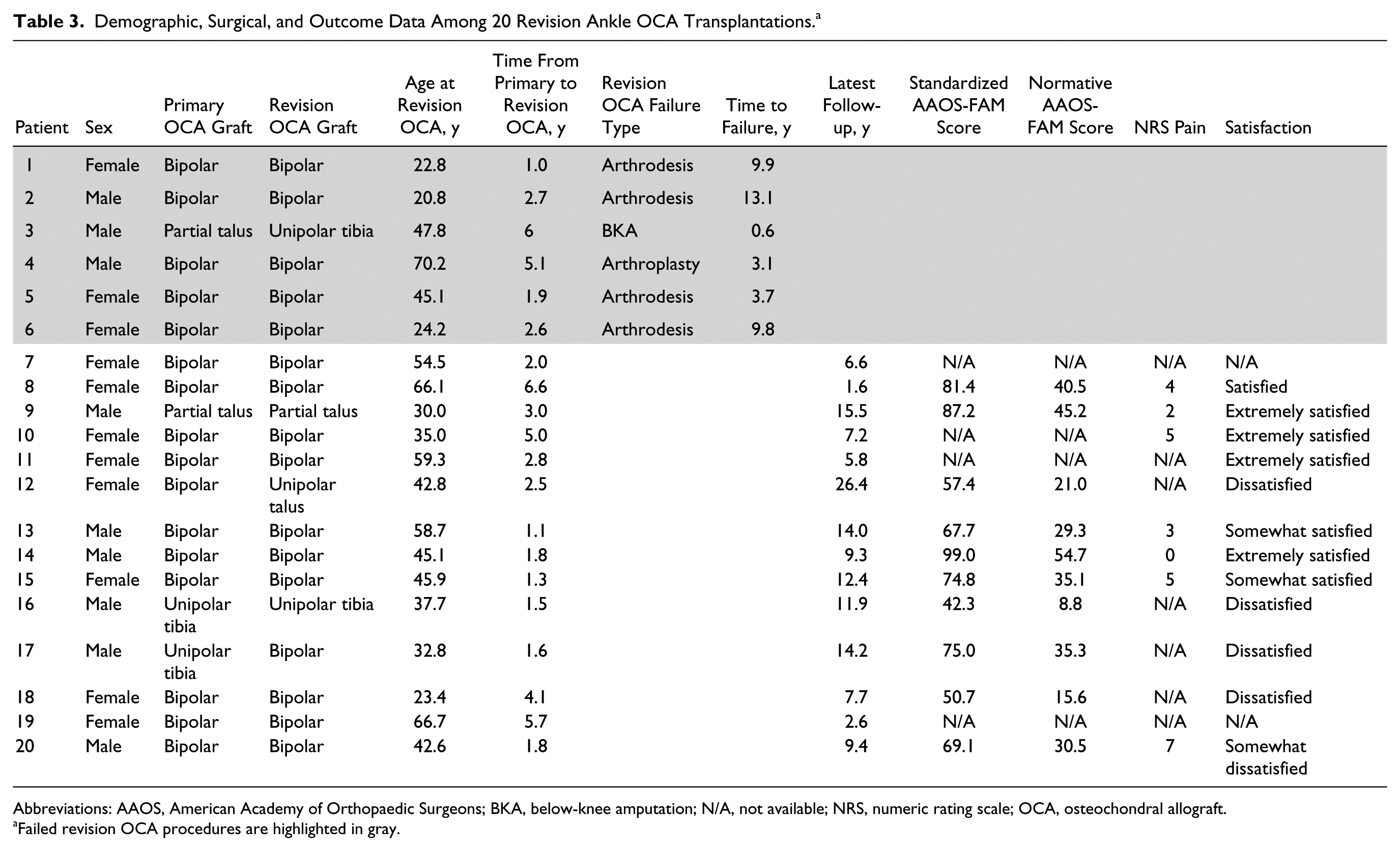
Abbreviations: AAOS, American Academy of Orthopaedic Surgeons; BKA, below-knee amputation; N/A, not available; NRS, numeric rating scale; OCA, osteochondral allograft.
Failed revision OCA procedures are highlighted in gray.
A subgroup analysis of the 16 bipolar revision allografts was performed. The average age of the 10 females and 6 males was 44.6 ± 16.9 (range, 20-70) years. The average BMI was 29.6 ± 3.1 (range, 26.6-36). The mean time from primary OCA transplantation to revision surgery was 2.9 ± 1.8 (range, 1-6.6) years. Seven of 16 ankles had further surgery following the revision OCA. Failure of the bipolar revision allograft occurred in 5 of 16 ankles (4 arthrodeses and 1 total ankle arthroplasty) at a median of 9.8 (range, 3.1-13.1) years. Survivorship of the bipolar revision allografts was 85.7% at 5 years and 57.1% at 10 years. Among the 11 ankles with the bipolar revision allograft remaining in situ, the mean follow-up duration was 8.3 ± 4.2 (range, 1.6-14.2) years. Subjective data regarding pain, problems with ankle, and satisfaction among patients are listed in Table 3.
Discussion
To our knowledge, this is the first study of patients who underwent revision OCA transplantation of the ankle after primary failed OCA. Only 1 publication could be found regarding outcome data after revision OCA performed by Horton et al, but that study was done analyzing the knee joint. 11 The authors reported on a case series of 33 patients with a mean follow-up of 10 years. They observed a failure rate of 39% (13 patients), a mean time to failure of 5.5 years, and an allograft survivorship of 61% at 10 years, all of which are similar to our findings. Even though the authors concluded that revision OCA transplantation is a useful tool for revision surgery, the results are inferior to a primary allograft in the knee. As the results of our study show, this is not the case with revision OCA transplantation of the ankle. With an overall failure rate of 30%, a mean time to failure of 6.7 years, and a survivorship of 65% at 10 years, the outcome data we presented is not inferior to a primary allograft of the ankle.
Because of the lack of publications regarding the use of OCA transplantation as a revision procedure, we had to compare our results to studies of primary OCA transplantations of the ankle joint. As recent reviews have shown, unipolar allograft procedures generally have a better outcome, fewer complications, and a clearly lower failure rate in comparison to bipolar allograft transplantation of the ankle.15,25 However, our study population was mixed and mainly included bipolar OCA transplantation for the revision procedure (80%) and should therefore rather be compared to results of primary bipolar OCA procedures.
The most recent study by Giannini and colleagues showed short-term outcome data after fresh bipolar OCA transplantation of 26 patients (69.2% male) with the use of specifically designed jigs at a mean follow-up of 40.9 ± 14.1 months. 8 The survival rate of the allograft was 88.5% at the final follow-up with an improvement of the average American Orthopaedic Foot & Ankle (AOFAS) ankle-hindfoot score from 26.6 ± 6 preoperatively to 77.8 ± 8.7 postoperatively and good to excellent results in 76% of patients. Six of the 26 patients were considered an OCA failure, of which 3 patients underwent revision surgery. Radiographic analysis showed no statistical relationship with the grade of arthritis and clinical outcomes, but there was a significant correlation between better clinical outcomes and lower degrees of distal tibial slope.
Bugbee et al reported on the largest series of patients to date (88 ankles in 84 patients) undergoing primary fresh bipolar allograft transplantation of the tibiotalar joint with a mean follow-up duration of 5.3 years. 4 Forty-two percent of the patients required further surgery, of which 11 procedures (13%) were not related to the graft (eg, hardware removal, debridement, synovectomy). The overall failure rate was 29% (25 patients) with a mean time to failure of 3.7 ± 2.5 years. The graft survivorship was 76% at 5 years and 44% at 10 years. Based on an improved average Olerud-Molander Ankle Score from 27.7 points preoperatively to 61.1 points postoperatively, 62% of the patients were considered to have good to excellent outcomes. The vast majority (92%) of patients expressed satisfaction with the results of the OCA transplantation, 85% reported less pain, and 83% reported having improved postoperative function.
Jeng et al reviewed the results of 29 primary total ankle al-lograft transplantations for the treatment of ankle arthritis. 13 They defined OCA failure as a removal of the allograft and performing revision surgery; the failure rate was 51.7% at a mean follow-up of 2 years. Revision allograft transplantation was required in 5 patients, arthroplasty in 3 patients, and arthrodesis in 5 patients. However, they also found 6 radiographic failures with the allograft still implanted at the time of the final evaluation, which lead to an overall failure rate of 69% (20 patients). The 9 successfully treated patients had a mean AOFAS ankle-hindfoot score of 84 (range, 71-96) and 67% of the patients reported they would undergo the procedure again (11% responded no, 22% were unsure). Furthermore, the authors also reviewed the 5 patients who underwent revision allograft transplantation. Two patients had satisfactory radiographs and no clinical complaints. One patient had narrowing of the joint space as shown radiographically with some painful symptoms, but reported to have less pain in comparison to after the primary OCA transplantation. Two patients were considered OCA failures. Therefore, the overall revision failure rate of 33.3% is lower than the failure rate of primary OCA transplantation, and similar to the results of our current study.
Meehan et al reported a case series of 11 patients who had fresh OCA transplantations of the ankle joint. 19 In this mixed cohort with 81.8% bipolar allografts (9 patients), the overall failure rate was 45.5% (5 patients). Considering only the bipolar allografts, the failure rate was nearly the same (44.4%, 4 of 9 patients). Three of the patients who experienced an OCA failure underwent revision bipolar allograft transplantation with successful results at the latest evaluation (mean of 12.5 months), 1 patient required ankle arthroplasty, and 1 patient had no further surgery (radiographic failure). The mean AOFAS score of the 6 successfully treated patients improved from 55 to 73 postoperatively.
Kim et al examined the results after bipolar OCA transplantation for the treatment of post-traumatic ankle arthritis in 7 cases with a mean follow-up of 148 months. 17 The failure rate was 42% (3 of 7 cases), and 57% of the patients reported good to excellent results with improved mean ankle scores from 25 preoperatively to 43 at the latest evaluation.
It is also important to compare our results to the gold standard procedure of arthrodesis. Although studies show successful results after primary ankle arthrodesis with fusion rates up to 100%, the results after revision arthrodesis show clearly lower union rates, poorer satisfaction rates, and extended time to union.1,5,6,20 Furthermore, 2 recent studies show inferior results of revision arthrodesis of the ankle after failed ankle replacement.16,22 Although Kamrad et al showed a union rate after revision arthrodesis of 90%, less than 50% of the patients were satisfied. Rahmen et al reported reduced function, higher pain, and impaired quality of life after salvage arthrodesis in comparison to primary ankle fusion.
After a mean follow-up of 10.3 ± 6.3 years, the patients in our study whose allografts were in situ reported a mean standard AAOS-FAM Score of 70.5 ± 17 (range, 42.3-99) and a mean normative score of 31.6 ± 13.8 (range, 8.8-54.7). Unfortunately, most of the recent publications regarding ankle surgery in general, and specifically allograft procedures, used a wide spectrum of different evaluation tools, in most cases the AOFAS score.12,15 Therefore, it is difficult to compare our data with other publications in terms of subjective outcomes. However, a few publications could be found using the AAOS-FAM score as a clinical evaluation tool after ankle procedures.
Rammelt et al reported in a multicenter study including 38 patients undergoing retrograde tibiocalcaneal fusion using the Hindfoot Arthrodesis Nail. 23 Twenty-four percent of the patients had at least 1 postoperative complication and 6 patients (16%) had nonunion requiring further revision surgery. The authors considered this nonunion rate low for their group of patients, which included patients with previous nonunion, Charcot arthropathy, and other severe deformities. After an average follow-up of 2 years, the patients reported low pain levels with a mean NRS of 2.2 and a mean normative AAOS-FAM score of 38. Haene et al reviewed 16 patients (17 ankles) who underwent fresh unipolar allograft surgery for the treatment of large osteochondral lesions of the talus. 10 At an average follow-up of 4.1 years, 2 patients required further arthroscopic debridement as a result of ongoing pain, 35% of the patients had mild to moderate ongoing symptoms, and 29% of the patients were considered failures. The mean standard AAOS-FAM scores improved from 52.3 to 69.9 postoperatively. Aurich et al presented a case series of 18 patients who had arthroscopic matrix-associated chondrocyte implantation for the treatment of osteochondral lesions of the talus. 3 The authors showed that all assessed clinical scores improved after the procedure. The mean standardized AAOS-FAM score increased from 59.9 ± 16.0 preoperatively to 83.5 ± 13.2 postoperatively, and the normative score increased from 23.0 ± 13.0 to 42.2 ± 10.7. In comparison to these 3 selected publications, the patient outcomes regarding the AAOS-FAM scores in our study are similar and not clearly inferior to other primary ankle procedures.
Our study has several limitations. The first limitation of this study is the small patient population and that not all patients answered all the questions from the follow-up questionnaire. However, allograft transplantations of the ankle are generally rare, and publications regarding these operations often report outcome data only on a small case series. Another limitation is that the functional outcome data (measured by the AAOS-FAM score) used in this study is difficult to compare with the existing literature and that there was no functional assessment prior to revision surgery. As recently reviewed, most of the existing ankle-related outcome studies have used the AOFAS scales. 12 However, Madeley et al concluded in their outcome measure instrument validation study that the AOFAS score may not be sufficient to truly compare or quantify patient outcomes because of its objective components. 18 Furthermore, there is still a need for a more consistent use of valid and reliable outcome measure instruments in foot and ankle related research. 12 We chose the self-administered AAOS-FAM score because it is one of the few foot and ankle scores that has internal and external reliability measures, 24 it met 3 of the 4 validity criteria (with the exception of responsiveness), 12 it is easy to fill out, 7 and it does not require a follow-up clinical examination, for which our patients were not available. Third, there was no radiographic follow-up that theoretically could have diagnosed more (clinically asymptomatic) revision allograft failures.
Conclusion
In this study, we present for the first time outcome data of OCA transplantation of the ankle as a revision procedure. The high rates of persistent pain, further reoperations, and allograft failure (30%) suggest that the indications for an OCA as a revision/salvage procedure should be carefully evaluated. However, the failure rate is similar to primary OCA transplantation, with a survivorship of 65% at 10 years. Considering the treatment alternatives (arthrodesis and arthroplasty), we think OCA transplantation as a revision procedure after primary failed OCA transplantation can be a useful treatment option, especially for young and active patients. Further studies with larger cohorts are needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.