
Abstract
Background:
Corticosteroid infiltration (CI) is commonly used for treatment of plantar fasciosis. In recent years, however, interest has grown in the use of intratissue percutaneous electrolysis (EPI) for the treatment of tendinopathies. The aim of our study was to compare the effectiveness of the above techniques in the treatment of plantar fasciosis.
Methods:
The results achieved over a period of 1 year following the use of these techniques to treat plantar fasciosis were examined. There were 64 patients; 32 of whom were treated with ultrasound-guided EPI and 32 with ultrasound-guided CI. A clinical examination was performed and ultrasound taken before treatment and at 3, 6, and 12 months. Clinical assessments were made using a visual analog scale (VAS) to record pain and the Foot and Ankle Disability Index (FADI) to evaluate function. Ultrasound was used to determine the thickness of the plantar fascia.
Results:
Both the ultrasound-guided EPI and CI techniques were associated with significant clinical and echographic improvements at 12 months post-treatment (P < .001).
Conclusion:
Both techniques were effective in the treatment of PF, providing excellent VAS pain and FADI results at 12 months. However, CI required fewer patient visits and appeared to provide somewhat better VAS and FADI results.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Plantar fasciosis (PF) is one of the most common causes of foot pain.31,34 Discomfort is usually felt first in the heel, especially when getting out of bed or after sitting for a prolonged period. After standing or walking it can become sufficiently intense to require patients to sit down.24,27 PF commonly becomes a chronic problem; indeed, some 10% of patients have symptoms that have lasted over a year. 15 Histologically, the condition appears as a degenerative process with necrosis of the collagen and microtears in the fascia with no inflammatory response. This has led to some authors to prefer the use of the term fasciosis over fasciitis. 25 The incidence of PF in the general population is around 10%. 34 It is more common in those aged 40-60 years, and frequently seen in athletes.10,13,39 Many factors have been implicated in the appearance of PF, including obesity, being flat footed, having a high instep, a reduction in the dorsiflexion angle of the ankle, having tight calf muscles (leading to an increase in the muscular tension of the leg), being of advanced age, using inappropriate footwear, and prolonged standing.9,20,42 The evidence for some of these factors, however, is weak, and the etiology of PF remains incompletely known.26,28,41
The diagnosis of PF is based on clinical examination. Among the imaging techniques available, ultrasound provides a well-tolerated, low-cost, noninvasive alternative to magnetic resonance imaging (which should be considered a second-line diagnostic technique). 17 The normal plantar fascia is hyperechoic, isoechoic with the adjacent fat, and has a thickness of some 2 to 4 mm. In PF, the thickening of the fascia is increased to over 4 mm, and hypoechoic areas are present, factors directly related to pain in the heel.6,12,23,35
Different treatments for PF are available, including surgery if symptoms persist for 6-12 months. However, conservative treatment is the first choice. This may include physiotherapy, the use of functional bandages and kinesiotape, gastrocnemius muscle stretching, plantar fascia-specific stretching, plantar orthoses, shock wave treatment, dexamethasone iontophoresis, hyaluronic acid injections, radiofrequency ablation, injection with botulinum toxin, treatment with NSAIDs, and the local injection of plasma rich in growth factors. Corticosteroid injections (CIs) into the proximal insertion of the plantar fascia are commonly given, although no consensus protocol exists.8,16,18,27,28,33
Recently, however, intratissue percutaneous electrolysis (EPI) has become of interest in the treatment of tendinopathies. This technique involves nonthermal, electrochemical ablation of the lesion via the use of a cathodic fluid. The inflammation provoked is very localized and healing is rapid.1,30 Although EPI has been widely employed lately, the literature contains few studies validating its use.1,7,30,40 The good results reported in those that have been published led to the undertaking of the present work, which compares the long-term effectiveness of EPI and CI—both ultrasound-guided—for the treatment of PF.
Methods
Study Design and Patients
This study was designed as a retrospective, analytical, quasi-experimental comparison of the effectiveness of EPI and CI, both ultrasound-guided, in the treatment of PF. The study subjects were 82 patients who came to our medical center between January 2010 and December 2014. All had a clinical and ultrasound diagnosis of PF (an ultrasound-recorded fascia thickness of >4 mm with hypoechoic areas), presented with pain in the base of the heel of minimum 3 months’ duration (most significant when getting out of bed and sometimes improving after a short period of walking), and reported pain of ≥5 on a visual analog scale (VAS) (where 0 represents no pain, and 10 maximum pain) during palpation of the medial insertion of the plantar fascia. All patients had received previous conservative treatment (activity modification, stretching, cross-friction massage, and ice massage) at our own or other centers, but without symptom remission, and were therefore candidates for EPI or CI.
The protocols for EPI and CI were explained to patients since 2010 and they were allowed to choose which treatment they preferred. To be included in the present analysis, patients had to meet the criteria for a diagnosis of PF, to provide informed consent (in agreement with the Declaration of Helsinki regarding research on human subjects), 43 to choose one of the 2 techniques offered, to have no allergies to the medications used, and to complete the treatment chosen. Those patients who had not previously undergone conservative treatment, who could not provide informed consent, who made no choice of procedure to undergo, had any form of fascia rupture (total or partial), or who were allergic to any medication used, were excluded.
The final number of patients eligible for inclusion was 64. Of these, 32 were treated with EPI, and 32 with CI, both ultrasound-guided (Figure 1). Prior to treatment, all had an examination of functionality using the Foot and Ankle Disability Index (FADI; 0 = 100% incapacity, 100 = no incapacity). The study was approved by the ethics committee of the Universidad Alfonso X el Sabio de Madrid (Madrid, Spain). The mean age of the patients was 46.4±8.5 years; 29 patients (45.3%) were women and 35 were men (54.7%). The mean thickness of the fascia before treatment was 6.37±1.3 mm, the mean VAS pain score was 6.6±1.5, and the mean FADI, 42.2±9.2. No significant differences were seen between the 2 procedure groups in terms of any of these variables.
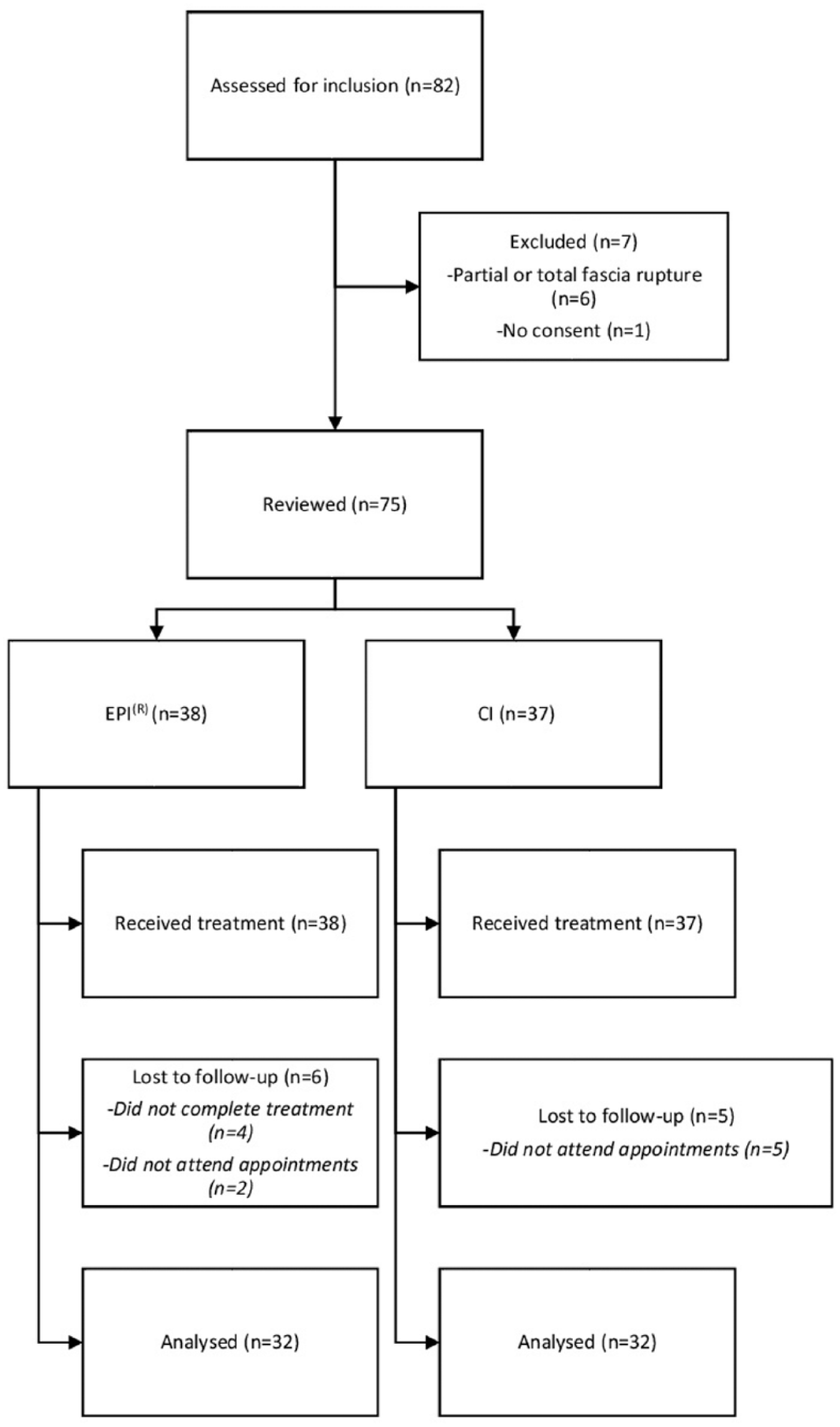
Flow diagram showing how the study population was selected.
Intervention Procedures
All interventions in both groups were performed by the present authors.
Corticosteroid injections
With the patient lying supine, the tibial nerve was localized by ultrasound and, following the cleansing of the foot with 2% alcohol-chlorhexidine, anesthetized using 2% mepivacaine. Ultrasound-guided intralesional infusion of the plantar fascia was then performed medially and perpendicularly (Figure 2), administering 1 mL of 2% mepivacaine and 1 mL betamethasone acetate + betamethasone sodium (Celestone Cronodose) together in a 20G-needle, 5-mL syringe. The same treatment was administered again 7 days later, and then once again in some patients as required (mean number of infiltrations 2.5).
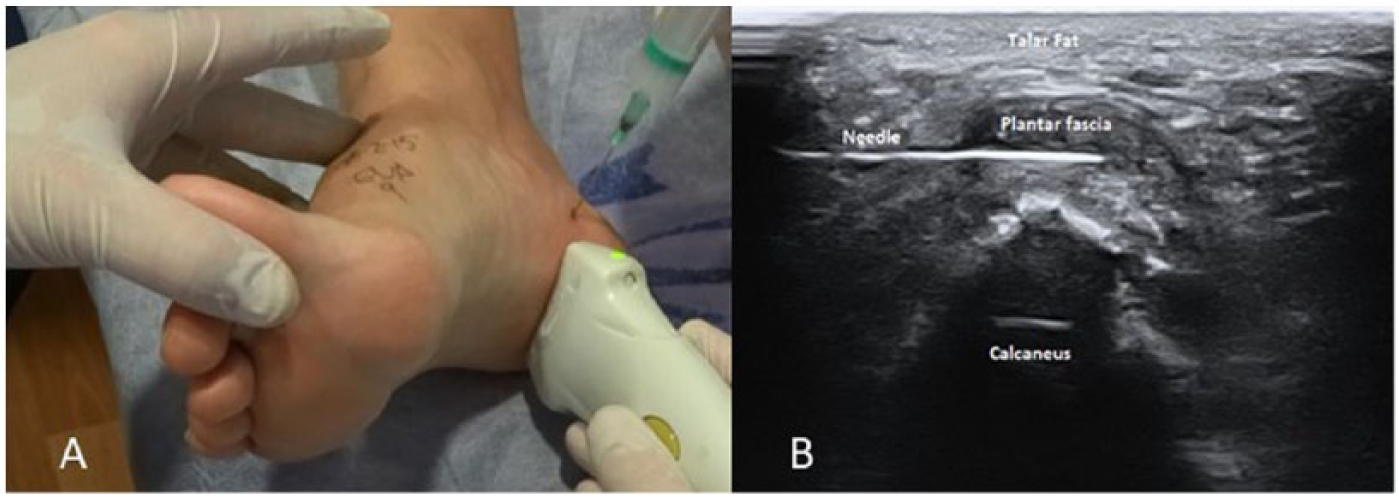
(A) Corticosteroid injection treatment. (B) Ultrasound imaging for needle guidance.
Intratissue percutaneous electrolysis
With the patient lying supine and after cleansing as above, a galvanic current was applied to the proximal insertion of the plantar fascia using a G32 needle as a cathodic flow electrode, employing a medically certified (Directive 93/42/EEC) device (EPI Advanced Medicine, Barcelona, Spain). Following a medial approach, the needle was guided to its target—the focus of the lesion—by ultrasonography (Figure 3). A 3-mA current was delivered for 5 seconds. The treatment was repeated 7 days later, and then again for up to 10 sessions at weekly intervals as required. Treatment was ended when the patients became asymptomatic (mean 5.2 sessions; one patient required only 3).
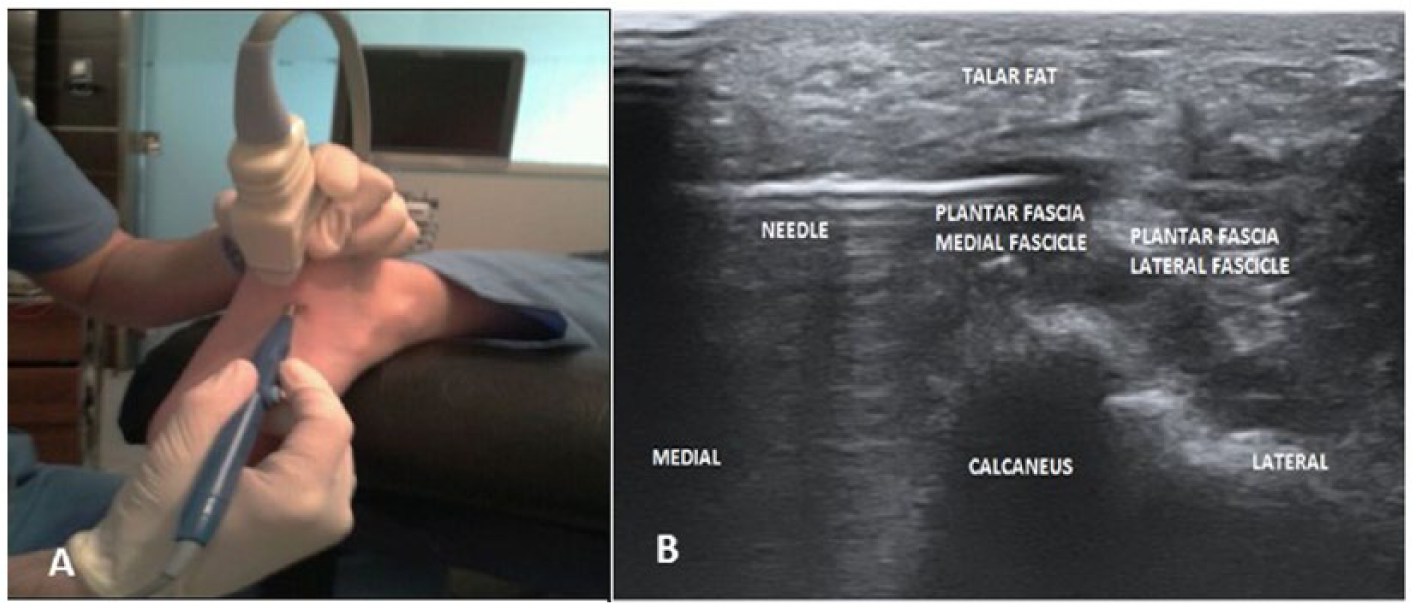
(A) EPI treatment. (B) Ultrasound imaging for needle guidance.
At 3, 6, and 12 months since the last treatment, all patients underwent ultrasound examinations and their VAS pain and FADI scores were recorded.
Ultrasound diagnoses, fascia measurements, and guiding for both treatments were performed using an Alpinion e-cube 15 device with a 50-mm linear probe (8-17 MHz).
Statistical Analysis
Descriptive analysis was performed for all quantitative and qualitative data. The Kolmogorov-Smirnov test was used to confirm that the quantitative variables were normally distributed, and the Student t test to analyze differences between the means. Contingency tables were used to explore the relationships between qualitative variables. The Fisher exact test or the χ2 test was used as required to analyze the influence exerted by one qualitative variable on another, and ANOVA for repeated measures was used to study behavior over time. The factor “between-subjects” was subjected to Greenhouse-Geisser (G-G) correction. Significance was set at P <.05. All calculations were performed using SPSS v.21.0 software for Windows.
Results
Both techniques (CI and EPI) provided similar results (P = .968) (Figure 4) with respect to reduction in the thickness of the fascia, and at all time points (3, 6, and 12 months) a significant reduction was compared to the starting size (G-G P < .001).
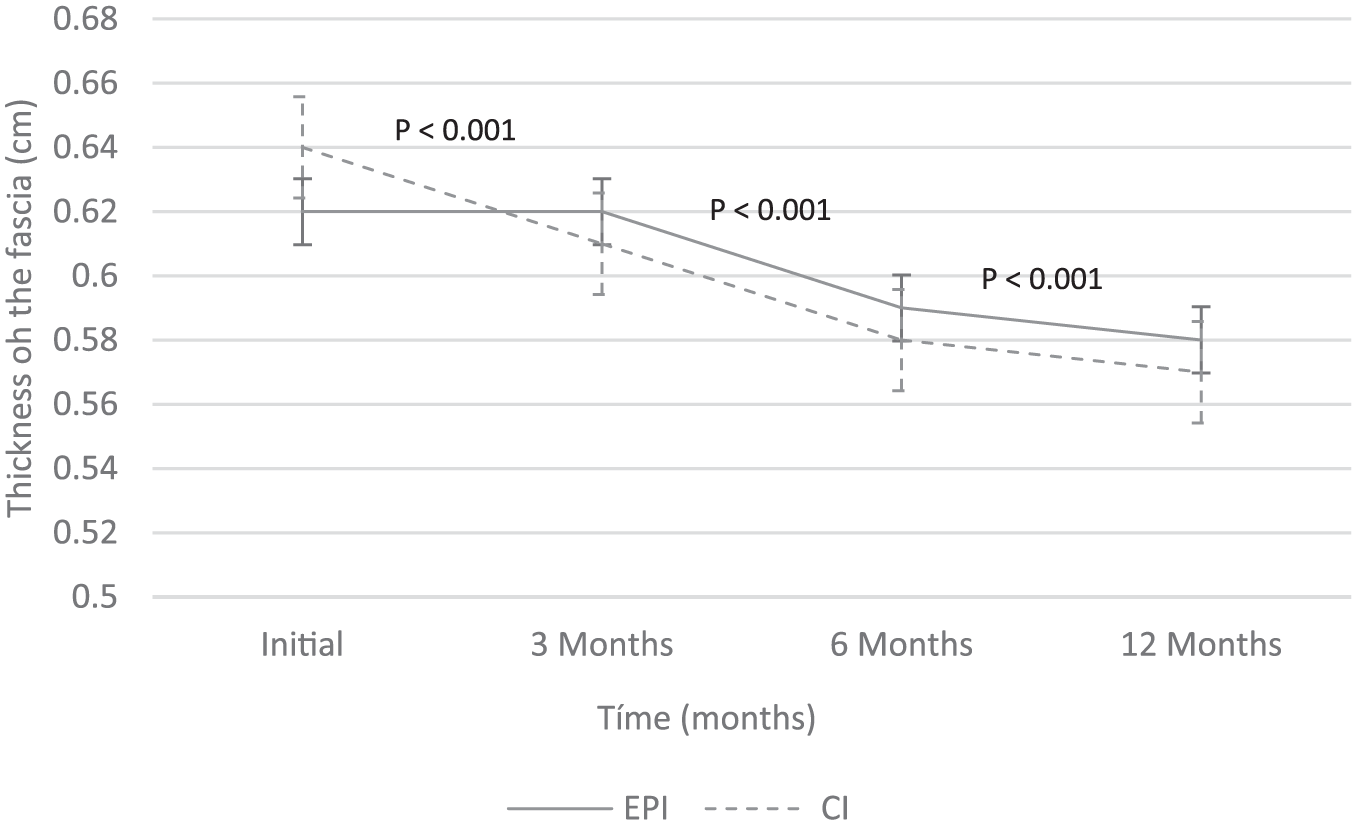
Post-treatment change in fascia thickness.
The 2 techniques had good but significantly different results in terms of the reduction in the VAS pain score (P = .002); in the mid- and long term, CI obtained a greater reduction in the VAS score than did EPI (Figure 5). At all time points (3, 6, and 12 months), a significant reduction was seen compared to the starting score for both techniques (G-G P < .001).
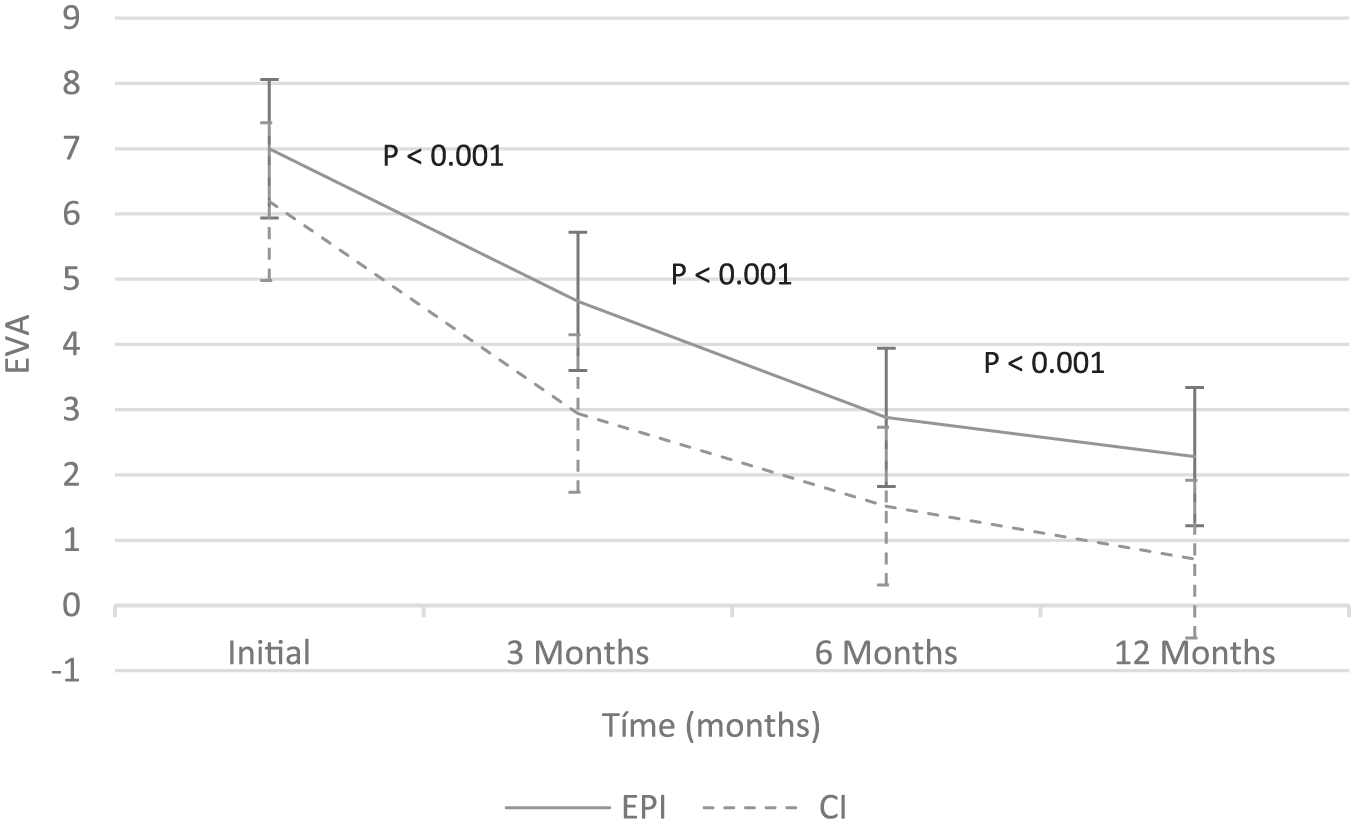
Post-treatment change in pain (as measured on a visual analog scale).
The 2 techniques had good but significantly different results in terms of the increase in the FADI score (P = .008); CI obtained a higher FADI score in the mid- and long term (Figure 6). At all time points (3, 6, and 12 months), a significant increase was seen in the FADI score for both techniques (G-G P < .001).
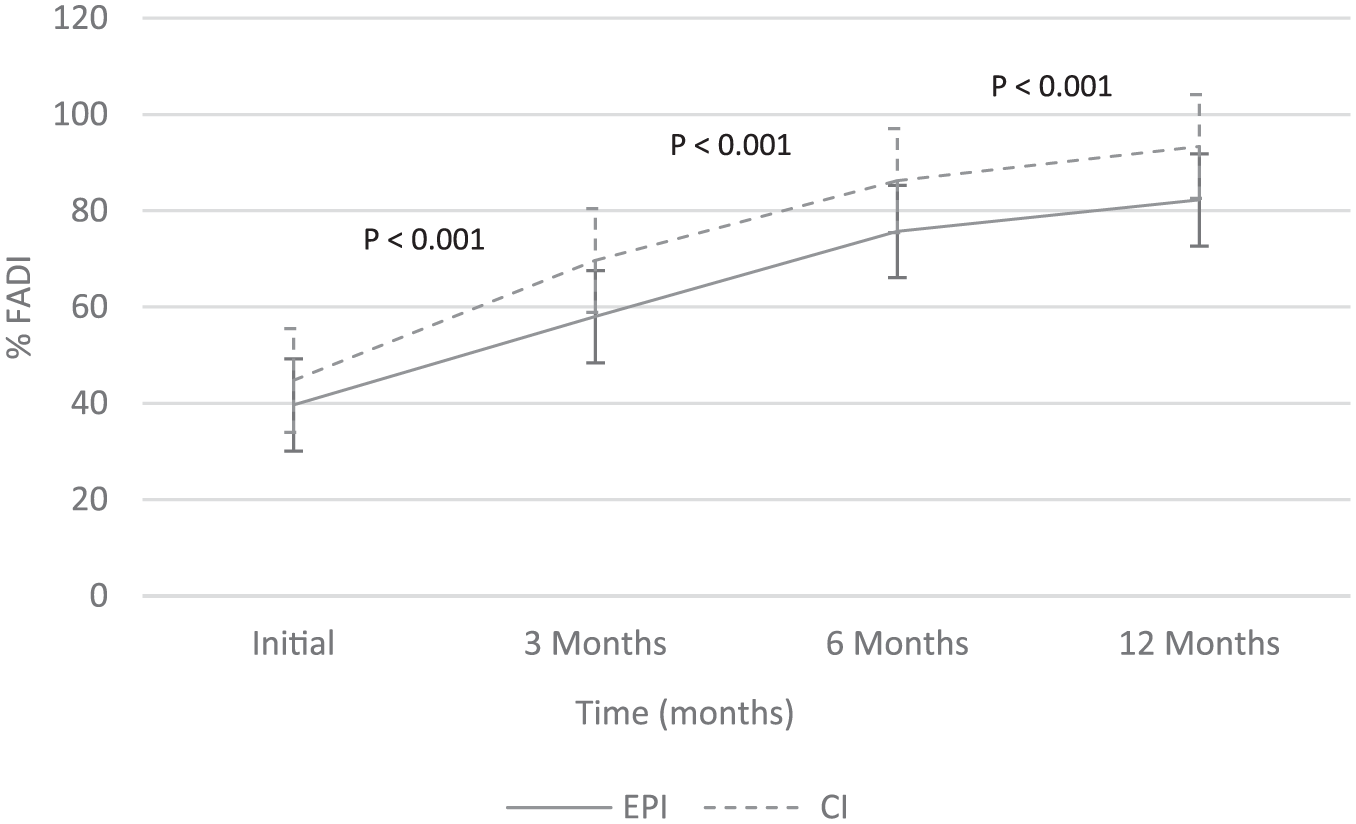
Post-treatment change in Foot and Ankle Disability Index.
Two patients (6.25%) had a vasovagal episode during the EPI procedure, whereas no patient who underwent CI experienced such an event. No patient needed analgesics irrespective of the treatment administered.
Discussion
Both CI and EPI were associated with significant improvements in pain (VAS score) and functionality (FADI score). Both significantly reduced the thickness of the plantar fascia (as measured by ultrasonography), but without normal values being reached. Thus, even though symptoms disappear, some thickening may remain. CI has been reported effective in the short term for the treatment of PF.21,26,29,37 In the present work, the improvement in pain and functionality seen early on was maintained at 12 months in most patients. Most patients treated by either technique showed improved FADI scores from 3 months onward. Other authors report no improvement in the very short term,3,22,38 but did not continue to monitor into the midterm.
In the present work, both treatments were guided by ultrasound. Although no evidence exists to suggest that CI is more effective when thus guided,5,26 ultrasonography has been routinely used in the authors’ clinic because it allows the accurate placement of the needle and thus minimizes possible harm to healthy tissue. 11 Indeed, a number of adverse effects have been reported for CI, including rupture of the fascia and atrophy of the plantar fat,4,19 that might be avoided with ultrasound guidance. In the present work, no patient treated with either technique had any adverse effect at 12 months.
The tibial nerve was anesthetized before beginning CI treatment in order to reduce the pain associated with the technique.14,29 Such anesthesia was considered unnecessary for the EPI treatment given the small gauge of the needle (32G). All patients reported some pain during this technique but in no case was it necessary to halt the treatment. It may, however, be wise to consider anesthesia for some patients, taking into account the experience and training of the person who is to provide the treatment (EPI can be provided by nurses, physiotherapists, etc, not just physicians in some locations).
EPI involves the use of a high-intensity galvanic current sent through an acupuncture needle that acts as a negative electrode. It has been shown experimentally to provoke an electrochemical reaction at the point of application, which causes a change in the extracellular pH. This leads to the destruction of the tissue and the induction of phagocytosis, and eventually biological repair.1,2,32,36 EPI has given good results in the treatment of tendinopathies.1,7,30,40 Its local inflammatory effect and its ability to induce local tissue regeneration could be of use in the treatment of PF—a degenerative process. 25 This is the first study to compare the use of EPI and CI for the treatment of PF. Previous studies on EPI involving patients with other tendinopathies, do not report the same number of sessions being required: from 4 to 6 sessions are recorded for the treatment of epicondylitis 40 and shoulder tendinopathy, 7 and up to a maximum of 10 in the treatment of patellar tendinopathy. 1 In the present work, the minimum number of sessions was three, the mean 5.2, and the maximum 10. The doses used ranged from 3 to 6 mA,1,7,30,40 although it is likely that 3 mA is sufficient to induce angiogenesis and tissue repair, 1 this being the dose used in the present study.
EPI and CI have a similar final cost. Although a mean 5.2 sessions were needed with EPI, and 2.5 with CI, the latter is more expensive per session since it must be performed by a physician.
Study Limitations
Because all the present patients had undergone conservative treatment for 3 months, the present work cannot show how effective either technique might be as a first-line treatment. It should be remembered that the choice of treatment by the patient did not allow the study to be blinded; blinded trials should be performed in the future. Finally, the present results should be understood with caution since all the patients went to the same center.
Conclusion
In conclusion, both techniques were effective in the treatment of PF, providing excellent VAS pain and FADI results at 12 months. However, CI required fewer patient visits and appeared to provide somewhat better VAS and FADI results in the long term.
Footnotes
Acknowledgements
The authors thank Adrian Burton for editing assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.