
Abstract
Background:
Identifying preoperative risk factors that may portend poorer operative outcomes remains a topic of current interest. In hip and knee arthroplasty patients, the presence of patient-reported allergies (PRAs) has been associated with worse pain and function after joint replacement. However, these results have not been replicated across studies, including in shoulder arthroplasty cases. The impact of PRAs on foot and ankle outcomes has yet to be studied. The purpose of our study was to evaluate whether PRAs influence patient-reported outcome in foot and ankle surgery.
Methods:
To determine if PRAs are linked to poorer operative outcomes, we retrospectively identified 159 patients who underwent elective foot and ankle surgery. PRA data were obtained via chart review, and patient-reported outcomes were assessed preoperatively and postoperatively via multiple domains, including Patient Reported Outcome Measurement Information System (PROMIS) physical function, pain interference, and depression measures. Consistent with prior methodology, we compared outcome measures (preoperative, postoperative, and the change in outcome scores) between patients without self-reported allergies to patients with at least 1 PRA.
Results:
There were 159 patients studied; 79 patients had no allergies listed, and 80 patients had at least 1 PRA. Of the 80 patients with at least 1 PRA, there were a total of 170 possible allergies. There were no differences in preoperative, postoperative, or the change in outcome scores for all PROMIS measures (physical function, pain interference, and depression; P > .05) between patients with at least 1 PRA and those patients without any listed PRAs.
Conclusions:
We were unable to prove our hypothesis that PRAs were linked to poorer patient-reported outcomes following foot and ankle surgery. Closer review of the published reports linking PRAs to worse total joint arthroplasty outcomes revealed data that, while statistically significant, are likely not clinically relevant. Our negative findings, then, may in fact parallel prior studies on hip, knee, and shoulder arthroplasty patients. The presence of PRAs does not appear to be a risk factor for suboptimal outcomes in foot and ankle surgery.
Level of Evidence:
Level III, comparative series.
Identifying patient-specific factors that may portend suboptimal outcomes following foot and ankle surgery is a topic of current interest.2,6 In other orthopedic specialties, several lines of evidence have suggested that patient-reported allergies (PRAs) are associated with poorer hip and knee arthroplasty outcomes.3,5,9,12 However, the data on PRAs as a risk factor for worse outcomes is conflicting as a similar study of patients undergoing shoulder arthroplasty failed to link PRAs to poorer outcomes or shoulder motion after total shoulder arthroplasty. 15 In addition, none of the aforementioned studies on PRAs in orthopedics used modern outcomes tools such as the Patient Reported Outcome Measurement Information System (PROMIS) that can efficiently capture outcome data from various domains without the obstacles inherent to traditional outcomes instruments such as responder burden and incomplete questionnaires. 1 Further, no study to our knowledge has assessed the role of PRAs in foot and ankle patients to determine if PRAs may represent an identifiable risk factor in foot and ankle surgery. Our hypothesis in this study was that patients with PRAs would have less function, greater pain, and more psychological impairment (i.e., depression) than patients with no self-reported allergies after foot and ankle surgery. The purpose was to compare PROMIS scores (physical functional, pain interference and depression) between patients with or without PRAs before and after surgery to assess for statistically significant differences.
Methods
Following Institutional Review Board (IRB) approval, we retrospectively reviewed charts of all patients who underwent foot and ankle surgery from June 2015 to December 2016 by the senior author. All operative procedure codes were included and captured through billing codes. Exclusion criteria included patients younger than 18 years as well as patients with incomplete or missing allergy information from intake questionnaires. Patients who underwent surgery for trauma, infection, or hardware removal were also excluded. Demographic data were gathered via intake questionnaires completed by patients at or prior to the day of their initial clinic appointment. PROMIS data—specifically, physical function, pain interference, and depression scores—were captured at every clinic appointment electronically using previously defined and validated criteria. 10 To briefly review, a PROMIS score of 50 represents a population average, and 10-point changes represent a standard deviation from that average. Higher scores in negatively worded questions like PROMIS pain interference and depression represent more disability (ie, greater pain and more depression), whereas larger PROMIS physical function scores indicate greater function. PROMIS measures from the clinic date closest to surgery were used for preoperative assessment, and PROMIS scores furthest from the date of surgery were used as the postoperative comparison. PRAs were identified from chart review, specifically from the intake questionnaires patients complete during their new patient clinic visits.
Mirroring prior methodology,5,12 we separated our study population into 2 groups, comparing PROMIS scores between those patients without self-reported allergies to patients with at least 1 PRA. Student t tests were used to compare baseline demographics as well as preoperative and postoperative PROMIS outcomes between these 2 groups. We also studied the change in PROMIS scores (delta) preoperatively and postoperatively between groups. Statistical significance threshold was set at P < .05, and statistics were performed in SPSS. An a priori power analysis determined that 116 patients would be needed to detect significant group differences at 80% power with alpha less than .05.
During the study time frame, 452 patients underwent surgery, and 159 met inclusion criteria and had complete PROMIS and self-reported allergy data. Of those 159 patients, 79 had no self-reported allergies, and 80 patients had at least 1 PRA. Of those 80 patients with at least 1 PRA, there were a total of 170 possible allergies (average of 2.1 allergies per patient with a maximum number of 6 PRAs in 1 patient; Figure 1). The breakdown of the number of allergies included 37 patients with 1 PRA (46%), 22 patients with 2 PRAs (28%), 11 patients with 3 PRAs (14%), and 10 patients with ≥4 PRAs (8%).
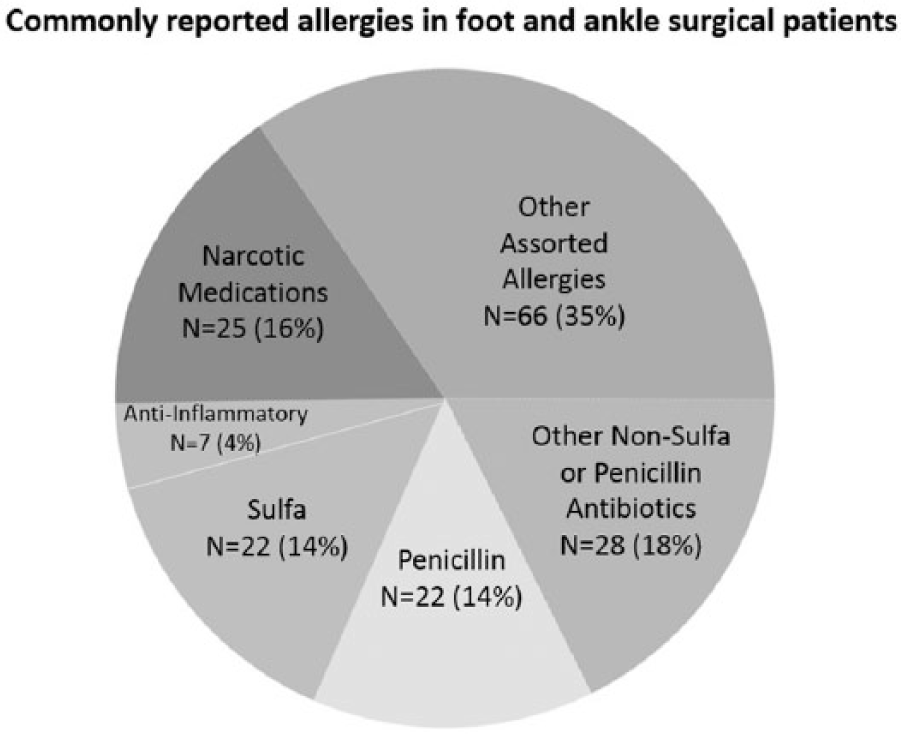
Diagram detailing the most common patient-reported allergies in foot and ankle operative patients.
Our cohort was predominantly female (118 women, 74% of the total study population). Comparing patients with and without PRAs, there were no differences in age at surgery or follow-up duration from surgery (Table 1). There were similar proportions of patients based on operative location (forefoot:midfoot:hindfoot:ankle) between patients with or without PRAs (n = 21:16:13:30 versus n = 22:18:13:26, respectively; Fisher exact test P = .93). Women were more likely to report PRAs than men (no allergies [n = 79]: 29 men, 50 women versus ≥1 PRA [n = 80]: 12 men, 68 women; χ2 P = .002).
Comparison of Outcomes Between Patients With No Reported Allergies and Patients With At Least 1 Self-reported Allergy.
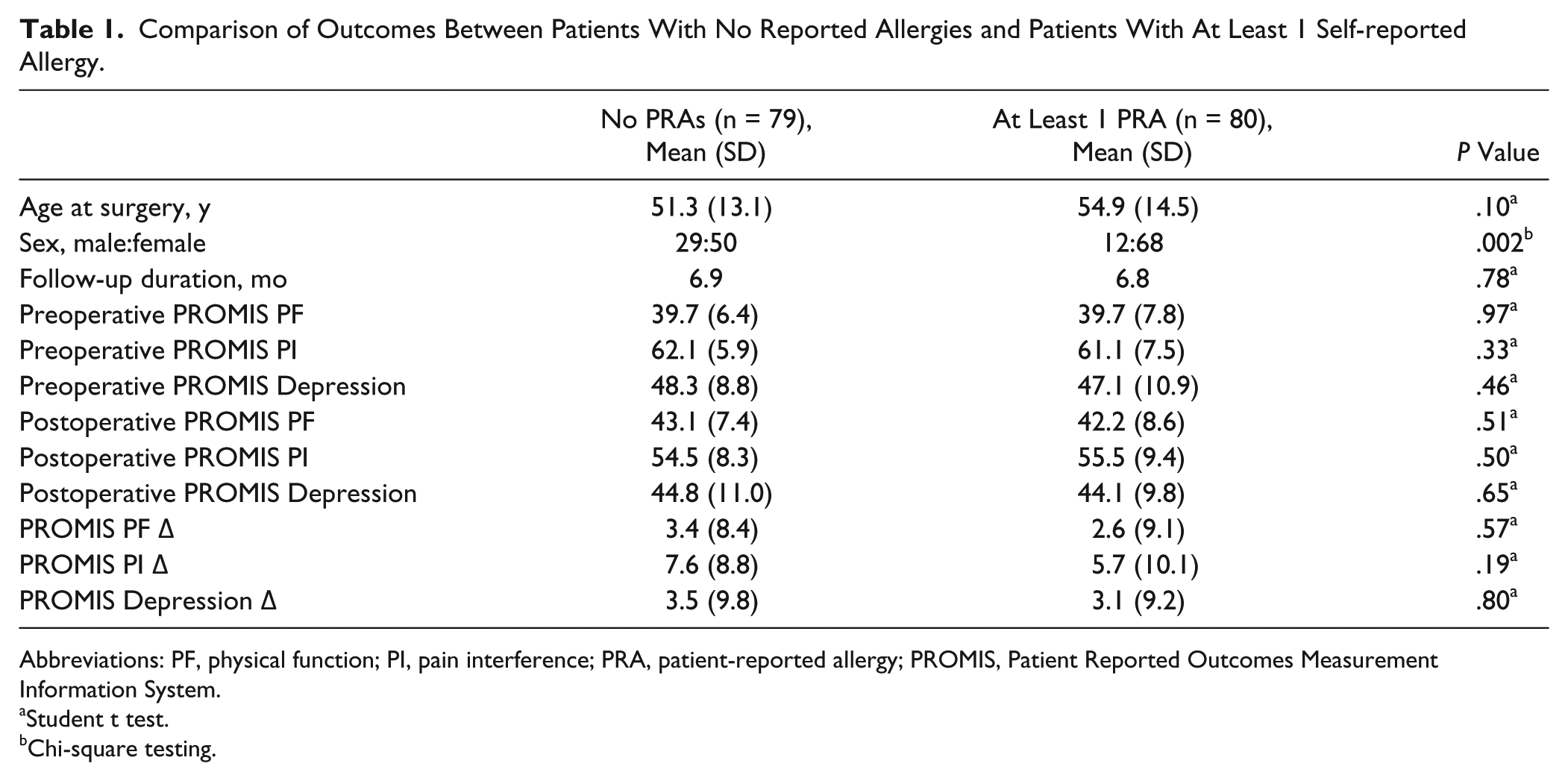
Abbreviations: PF, physical function; PI, pain interference; PRA, patient-reported allergy; PROMIS, Patient Reported Outcomes Measurement Information System.
Student t test.
Chi-square testing.
In our sample, the 5 most common procedures performed were hallux valgus corrections (n = 20), ankle arthrodesis (n = 12), first metatarsophalangeal arthrodesis (n = 12), triple arthrodesis (n = 12), and ankle arthroscopy (n = 9).
Results
There were no differences in preoperative, postoperative, or the change in outcome scores (delta) for all PROMIS measures (physical function, pain interference, and depression) between patients with no self-reported allergies and patients with at least 1 PRA (P > .05; Table 1).
Discussion
Earlier studies on hip and knee arthroplasty patients suggested that multiple PRAs were an apparent risk factor for poorer operative outcomes.3,5,9,12 However, a similarly designed study on shoulder replacement patients found no difference in outcomes or clinical motion between patients with or without PRAs. 15 No study has probed whether PRAs affect foot and ankle patient-reported outcomes. Here, we did not find any differences in PROMIS physical function, pain interference, or depression scores following foot and ankle surgery in patients with or without PRAs. Therefore, we were unable to prove our original hypothesis. Consistent with prior reports, our study did show that women more commonly had self-reported allergies than men.11,15
On closer inspection of the published data, our inability to identify differences in foot and ankle outcomes based on PRAs may actually be more consistent with the commonly cited hip and knee arthroplasty studies on this topic. Comparing hip and knee arthroplasty patients without PRAs to patients with at least 1 PRA, Otero et al 12 did not show any differences in preoperative SF-36 Physical Component Summary (PCS), postoperative SF-16 Mental Component Summary (MCS), or postoperative Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. In this cohort, only MCS and PCS scores were available preoperatively and postoperatively; the mean change in MCS and PCS scores in patients without allergies was 5.09 and 16.73, respectively, whereas the mean changes in MCS and PCS was 6.79 and 15.72, respectively, in patients with at least 1 PRA. 12 To understand if the changes in MCS and PCS scores from Otero et al 12 were clinically relevant, we compared them to published data on the minimal clinically important difference (MCID) for the same outcome measures in hip arthroplasty patients. Quintana et al 14 demonstrated that the MCID for the MCS following hip replacement ranged from 8 to 10 points and the PCS varied from 10 to 20 points, depending on how the measures were calculated. 14 Applying these MCID thresholds, it appears then that the findings from Otero et al 12 likely achieved MCID for PCS but failed to reach MCID for MCS, regardless of the patient’s allergy status.
In addition, the findings from Otero et al 12 curiously did not replicate the results by Graves et al, 3 which was the original pilot study on PRAs from the same institution. Otero et al 12 showed equivalent postoperative WOMAC scores between PRA groups, whereas Graves et al, 3 in fact, showed worse WOMAC pain, stiffness, and function scores in patients with fewer allergies, rather than more allergies. Taken together, the presence of PRAs as a marker for poorer operative outcomes may not be as convincing on closer review. Our failure to identify group differences in foot and ankle outcomes based on PRAs, then, may be more consistent with the arthroplasty literature.
Similar criticisms can be leveled at the data presented in other reports that concluded PRAs were a risk factor for poorer outcomes following total knee arthroplasty. Hinarejos et al 5 compared outcomes following total knee arthroplasty between patients with and without PRAs and found no differences in WOMAC and Knee Society Score (KSS) measures preoperatively and only statistically significant differences in WOMAC, WOMAC function, and KSS knee scores postoperatively. Just as with Otero et al 12 and Graves et al, 3 the between-group differences for the WOMAC (3.2), WOMAC function (2.3), and KSS knee subscale scores (3.5) from Hinajeros et al 5 all failed to meet the published MCID thresholds for each outcome measure.7,16 For example, SooHoo et al 16 defined the MCID for the WOMAC at 10.21 in total joint arthroplasty patients, whereas Lee et al 7 described the MCID for KSS knee scores between 5.4 and 5.9 in knee arthroplasty patients, depending on the statistical methods used. Careful assessment, then, of the data from the reports concluding that PRAs are a risk factor for poor operative outcomes highlights the fundamental difference between statistically significant results (P values) versus clinically relevant findings (MCID) in orthopedic research.
It has been suggested in nonorthopedic work that PRAs may be related to underlying psychological function.4,8,11,13 By using the PROMIS depression tool in this study—which surveys self-reported negative mood, views of self, and social cognition—we attempted to assess for any link between psychological dysfunction and PRAs. We did not find differences in PROMIS depression scores between patients with or without PRAs. This may be the result of several factors. In our data, the PROMIS depression tool exhibited the narrowest delta from before and after surgery of the 3 PROMIS tools used (Table 1). In addition, mean preoperative PROMIS depression scores in our study were 47.7, making them only 2.3 points away from the US population average of 50. Ho et al 6 found similar results with mean preoperative PROMIS depressions scores of 47.8. Perhaps another PROMIS instrument, such as the PROMIS anxiety score rather than PROMIS depression, might be better equipped to survey emotional distress and identify foot and ankle patients at risk for poor operative outcomes.
Our study has limitations. We pooled all foot and ankle surgeries performed during the selected time frame, leading to heterogeneity among the outcomes data. There may be select foot and ankle surgeries in which PRAs may affect outcomes (ie, hallux valgus correction); however, we were underpowered to perform such surgery-specific subanalyses. We analyzed only modern outcome data using PROMIS measures and did not include a traditional, validated foot and ankle–specific outcome tool such as the Foot and Ankle Ability Measure (FAAM). While PROMIS measures are generalized scores of function and pain not specific to the lower extremity, there is recent evidence suggesting that PROMIS and FAAM scores are related, indicating that we would likely have encountered similarly negative findings even if FAAM data were included for study. 10 Our average follow-up duration was only 6.9 months, but this is similar to the 7.3 months from Ho et al. 6 It is possible that differences in outcomes scores based on PRAs may not reveal themselves until later in the postoperative phase. However, unlike hip and knee arthroplasty patients in whom annual surveillance is routine, there may be selection bias for those foot and ankle patients presenting to clinics a year beyond surgery (ie, likely with continued disability compared with those patients without issue and may not require further care). Lastly, we did not assess postoperative patient satisfaction, which McLawhorn et al 9 suggested was particularly influenced by PRAs in lower extremity arthroplasty cases.
Conclusion
In conclusion, we were unable to demonstrate that PRAs were associated with worse patient-reported outcomes following foot and ankle surgery. While PRAs may anecdotally appear to be a patient-specific risk factor for poor operative outcomes, our data do not appear to support this notion in foot and ankle patients.
Supplemental Material
FAI769667-ICMJE – Supplemental material for Patient-Reported Allergies Do Not Predict Poorer PROMIS Function, Pain, and Depression Scores Following Foot and Ankle Surgery
Supplemental material, FAI769667-ICMJE for Patient-Reported Allergies Do Not Predict Poorer PROMIS Function, Pain, and Depression Scores Following Foot and Ankle Surgery by Devon C. Nixon, Brian M. Cusworth, Jeremy J. McCormick, Jeffrey E. Johnson and Sandra E. Klein in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.