
Abstract
Background:
Conservative treatment or debridement is generally sufficient for Freiberg’s disease grades I and II but operative intervention for the late stages of the disease process (III-V) is more challenging. Debridement alone is not sufficient and various forms of arthroplasty have been put forward. We have evaluated the outcomes of patients treated with an interpositional arthroplasty technique using a pedicle graft of periosteum and fat made into a “Rollmop” spacer for severe Freiberg’s disease. No results have previously been reported for this technique.
Methods:
Twenty-five consecutive cases (23 patients) were performed from February 2009 to September 2016 (20 females, 5 males). Mean age at surgery was 52.6 years (range 19-70.5 years) with 92% affecting the second metatarsal. Twenty-three were primary cases and 2 were revision cases. Five cases were stage III, 12 were stage IV, and 8 were stage V. All patients underwent interpositional arthroplasty using a periosteum and fat pedicle graft from the affected metatarsal shaft as described by Myerson. Patients were evaluated using Manchester-Oxford Foot Questionnaire (MOXFQ) and American Orthopaedic Foot & Ankle Society Questionnaire (AOFAS). Mean follow-up was 3.5 years (0.6-7.6 years). Paired 2-tailed Student t tests were used to assess clinical significance.
Results:
Surgery allowed 8 patients to return to normal footwear, 10 patients returned to fashion footwear/heels, and 5 returned to sports. Nineteen cases (17 patients) were assessed with patient-reported outcome measures and all showed a clinically and statistically significant improvement in their scores. Mean pre- and postoperative VAS pain scores were 6.2 (range 4-9) and 1.8 (range 0-6) (P < .05). Mean perioperative AOFAS scores were 45.6 (range 15-73) and 82.7 (range 57-100) (P < .05). Mean perioperative MOXFQ scores were 60.0 (range 23-89) and 18.1 (range 0-80) (P < .05).
Conclusion:
This novel interpositional arthroplasty technique using a “rollmop” of periosteum and fat for severe Freiberg’s disease produced significant improvements in pain, functional outcome, and patient satisfaction without donor site morbidity. Furthermore, it allowed patients to return to desired footwear and sporting activities. The functional outcome and joint range of motion was superior after a K-wire was no longer placed across the joint, and we believe it is essential to avoid this to permit early range-of-motion exercises.
Level of Evidence:
Level IV, retrospective case series.
Introduction
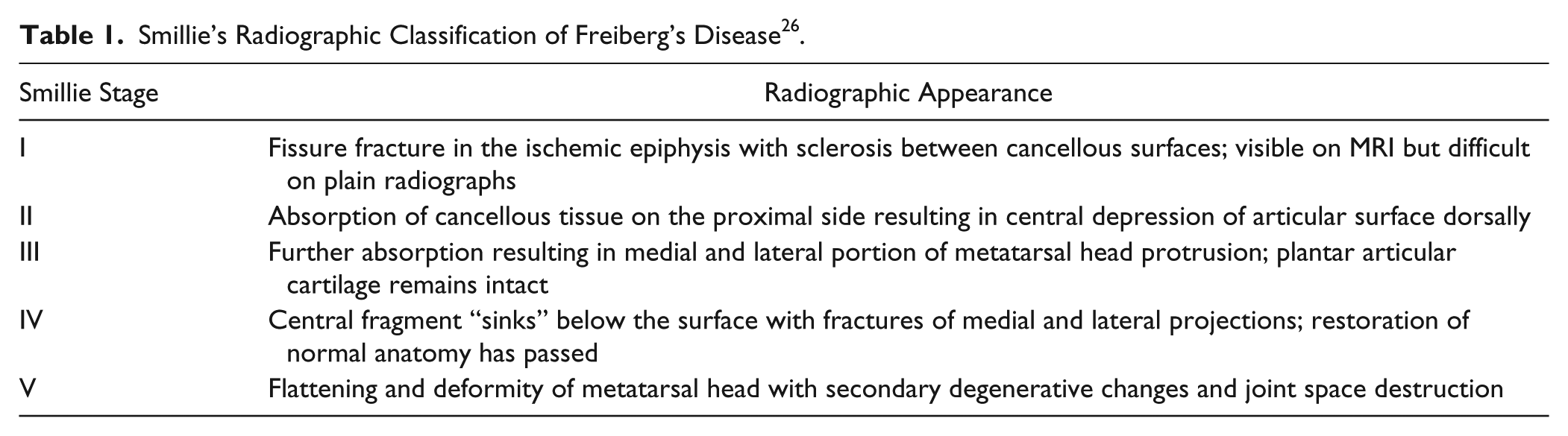
In 1967, Smillie classified the radiographic features of Freiberg’s disease into a commonly used classification system involving 5 stages. This classification system is the most referenced system and can guide management (Table 1). 26 Conservative methods are recommended as first-line treatment in the early stages (I and II) of Freiberg’s disease whereby the articular surface remains preserved. Operative intervention is usually reserved for late stages of the disease process (III-V) or when conservative management has proven to be unsuccessful. Various treatment options are available in the operative management of Freiberg’s disease. In the early stages of Freiberg’s disease (stages I-III), restoration of joint congruity can be attempted by joint debridement, elevation of depressed fragments, and metatarsal osteotomy.9,27 Even in these early stages, most authors have focused on osteotomy surgery, rotating the metatarsal head dorsally in order to take the dorsal diseased head out of the central arc of motion and instead bringing the plantar cartilage, which is generally intact, into this articulation.11,15 This is a challenging procedure and risks alteration of the normal loading biomechanics of the forefoot. This can be desirable when shortening of the metatarsal is feasible. 15
Smillie’s Radiographic Classification of Freiberg’s Disease 26 .
However, in the later stages of this disease process it can be difficult to restore joint congruity with debridement alone, and no current literature advocates the procedure. Even osteotomy alone may not restore joint congruity especially as the metatarsal head becomes affected more globally, and therefore joint arthroplasty should be considered. 29 Such as the intention of all arthroplasty, this has the theoretical intention of maintaining or even improving the range of motion but this has not been explored to the same extent as large joint arthroplasty. Several authors have performed interpositional arthroplasty using extensor digitorum longus (EDL), 4 extensor digitorum brevis (EDB),18,22 or palmaris longus tendon grafts, 17 with good reported clinical outcomes in small case series. Despite the various operative treatments described in the literature, no true consensus has been reached with respect to the most optimal treatment option for late-stage Freiberg’s disease. It is difficult to draw conclusions based on case reports and small case series.
We evaluated the outcomes of patients with Freiberg’s disease who were treated with a modified interpositional arthroplasty technique using a “rollmop” made up of a pedicle of both periosteum and fat to act as a spacer. This technique was first described by Myerson, 21 but as of this writing no clinical results for the procedure have been published.
Methods
The case series consisted of 25 feet (12 left, 13 right) in 23 patients who underwent interpositional arthroplasty using periosteum and fat for Freiberg’s disease unresponsive to conservative measures. All procedures were performed by a fellowship-trained senior surgeon between February 2009 and September 2016. There were 20 women (80%) and 5 men (20%), with 2 patients undergoing bilateral interpositional arthroplasty procedures during separate admission. There were 23 primary interpositional arthroplasty cases and 2 revision cases in this series.
The main presenting complaint in all our 25 cases was pain during daily activities including standing, walking, and running. Many patients also complained of painful restriction of motion depending on footwear type, in particular, the inability to wear high heels. All cases were initially managed conservatively with rest, anti-inflammatory medications, orthoses or footwear modifications, taping, and intra-articular steroids. Patients unresponsive to conservative measures for more than 3 months were offered this interpositional arthroplasty procedure.
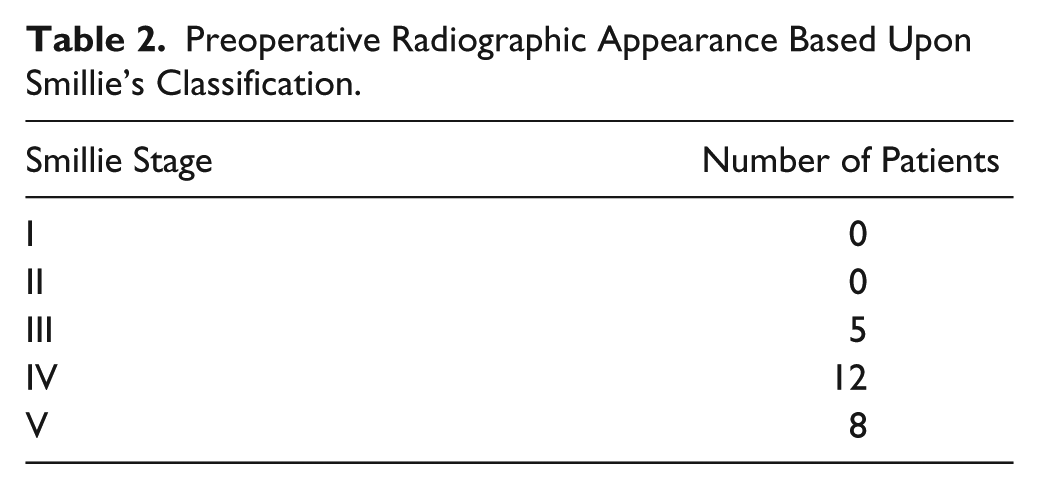
The mean age at the time of surgery was 52.6 years (range 19-70.5 years). The second metatarsal was affected in 23 (92%) cases, with only 2 cases affecting the third metatarsal. Radiological staging of the cases was based on the Smillie classification system (Table 1). According to the Smillie classification system, 5 feet were in stage III (21.7%), 12 were in stage IV (43.5%), and 8 were in stage V (34.8%). None of the feet were in stage I or II (Table 2).
Preoperative Radiographic Appearance Based Upon Smillie’s Classification.
Operative Technique
All procedures were performed by the senior author, with the patient in a supine position, under general anesthetia, and a tourniquet was applied. The dorsal aspect of the affected metatarsophalangeal (MTP) joint was approached with a longitudinal incision from the distal shaft of the metatarsal to the shaft of the proximal phalanx in line with the extensor tendon.
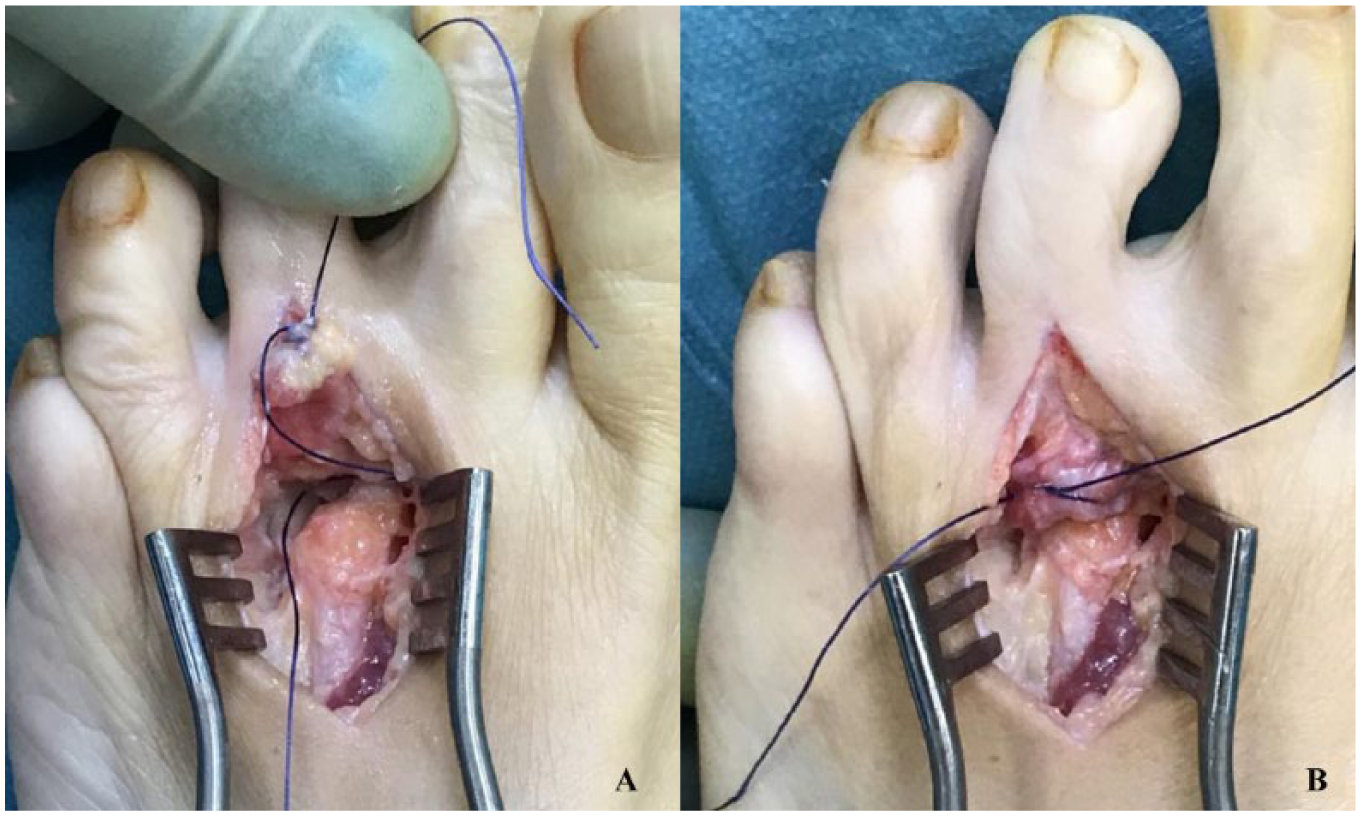
Following retraction of the extensor tendons, a transverse incision was made onto the dorsal aspect of the affected metatarsal approximately 3 cm proximal to the joint (Figure 1A). This was continued down both sides of the shaft to give a pedicle equal in width to the joint. The periosteum and fat was elevated subperiosteally en bloc from proximal to distal to expose the MTP joint (Figure 1B). Care was taken when approaching the joint as it was essential that the flap remains attached to the base of the proximal phalanx and it was easy to divide it at the joint level. If it was inadvertently cut, the tissues could be used as a free graft but it was preferable to retain it as a vascularized graft.

(A) The extensor hood is incised and the extensor mechanism is retracted. (B) A flap of periosteum and fat is elevated from the dorsum of the metatarsal; this may expose part of the interossei on either side. This must remain attached to the base of the proximal phalanx and care must be taken at joint level as the capsule is the weakest part of the flap.
Next, an excisional arthroplasty was performed on the affected metatarsal head clearing all osteophytes and affected cartilage (Figure 2). This was done to facilitate motion and it may be helpful to remove more bone from the dorsum of the affected metatarsal head and even the dorsum of the proximal phalanx. As with any cheilectomy, it was helpful to remove up to one-third of the dorsal head. The aim was to restore the ball-and-socket nature of the joint. We believe it was possible to preserve physiological loading through the metatarsal cascade even while removing bone and shortening the true length of the metatarsal because the plantar cartilage was invariably intact and its preservation would ensure maintenance of point of contact with the ground and therefore prevent alteration to the loading pattern.

(A) Joint is exposed but it is preferable to retain the collateral ligaments. (B) The metatarsal head is debrided to round it off and shorten it. The dorsal head can be reduced; the plantar cartilage does not require debridement. The dorsum of the proximal phalanx can also be debrided. Ensure that full range of motion is possible.
To create the “rollmop” graft, a nontoothed forcep was used to hold the proximal end of the pedicle, which was then rolled around the tips of the forceps (Figure 3A). Once this was complete, the tips were opened slightly and while still being held, the graft was sutured into a roll with 2-0 Vicryl by passing the needle between the tips of the slightly opened forcep (Figure 3B). The Vicryl was pulled through leaving the end attached to the needle long, and the free end approximately 4 to 5 cm long.

(A) The end of the flap is grasped loosely distally with forceps and then rolled into a “rollmop.” (B) This is sutured through the limbs of the forceps to create the “rollmop” graft. One limb of the suture should be long.
To position and stabilize the graft, it is sutured to the plantar plate (Figure 4A). The needle was taken through the plantar plate and the periosteum and fat graft was then pulled down into the joint space. It may be helpful to bend the needle to facilitate a smaller arc of rotation in order to pass it through a narrow space. Pulling on the needle drew the graft into the joint. This was done until the graft was sitting dorsocentrally and thus active in the dorsfilexion part of the arc of motion. The long end was then tied to the short end (Figure 4B).
(A) The longer limb is sutured through the plantar plate in order to stabilize the graft in the joint. (B) The long limb is pulled drawing the graft as far into the joint as required to create a cushion on the central and dorsal aspects of the joint, and this is then tied off.
At this stage, it was important to check the excursion of the FDL tendon to ensure that it had not been tethered by the suture. An absorbable suture was used as it was only there for temporary stability and this reduced the risk of FDL tether. Once this was secured, the range of motion was assessed. If the graft was unstable and was rolling up with dorsiflexion, a further suture was used to ensure that it was held between the articulating surfaces.
This series represents the development of this technique. At the beginning of this case series, a K-wire was used across the MTP joint to stabilize the graft. However, the senior author noted poor outcomes for range of motion in the first 8 patients and therefore modified the technique to suturing the graft to the plantar plate, thus avoiding fixing the K-wire across the MTP joint. Patients were then encouraged to start immediate range of motion.
Finally, the capsule was repaired with interrupted Vicryl sutures and the skin closed in maximal plantarflexion with running subcuticular Monocryl.
Postoperatively, the patients bore full weight in a flat postoperative shoe and were encouraged to commence immediate active range of motion exercises. If the procedure was an isolated case, patients were transitioned back into normal footwear at the 2-week follow-up; otherwise, they were rehabilitated according to the nature of any concomitant first ray surgery. Physiotherapy was generally not required as gait and range of motion recovered with normal function.
Follow-up
At final routine clinical follow-up, the patient’s functional outcome, return to footwear, and range of motion were recorded in the majority of patients. The movement was graded as excellent (equal to 66%-100% of the other side), moderate (equal to 66%-33% of the other side), and poor (less than 33% of the other side). These measurements were not routinely recorded preoperatively, and therefore assessment of range-of-motion change was based on the patient’s subjective response to a Likert-type scale question on his or her pre- and postoperative range of motion.
Patient assessment for this study was conducted via postal questionnaires by the primary author. The visual analog scale (VAS) for pain and 2 surveys were used to assess the subjective postoperative patient-reported outcome measures (PROMs). These included the validated Manchester-Oxford Foot Questionnaire (MOXFQ; total 64 points) and the American Orthopaedic Foot & Ankle Society Questionnaire (AOFAS; 100 points). The MOXFQ questionnaire assessed outcomes in 3 domains—walking or standing, pain, and social interactions—with a total score of 64 that was scaled to a score ranging from 0 to 100. Although the AOFAS questionnaire has not been validated, it was included in our study to provide comparison with similar studies. The AOFAS questionnaire included questions for pain, activity limitations, walking distance, footwear accommodations, and range of movement with a maximum score of 100. Furthermore, each patient was asked to scale the level of pain experienced at the affected metatarsal (VAS 0-10), footwear accommodation, and activity levels before and after surgery. The mean follow-up was 3.5 years, with a range between 0.6 and 7.6 years.
Statistical Analysis
Paired 2-tailed Student t tests were used to compare the clinical evaluations of the MOXFQ and AOFAS questionnaires and VAS prior to and following surgery. The threshold of significance was set at P <.05.
Results
Subjective Results
Of the 25 cases, 6 did not have PROMs scoring as they were symptomatic with either an unrelated ipsilateral lower limb or spinal pathology. Although this was significantly limiting their function, all cases subjectively reported good or excellent improvements in pain following surgery. Three of the 6 cases were awaiting further unrelated surgery, whereas the remaining 3 cases were undergoing investigations for lower limb or spinal pathology. They were included for analysis of complications, pathology, and return to footwear and sports but not for functional outcome scoring as it was not possible to determine the outcome of the interpositional arthroplasty independent of the unrelated lower limb or spinal pathology.
Prior to surgery, 18 of the 23 patients were unable to wear desired footwear. Following surgery, 10 patients were able to wear either fashion shoes, heels, or narrow shoes; 8 patients were able to wear normal footwear; and 5 patients were able to wear dress shoes or working boots.
Of the 5 patients who were unable to participate in athletic activities prior to surgery, all 5 were able to return to full sporting activities following surgery, which had not been previously possible because of pain. This included running, horse riding, and elite-level netball. No patients who were able to wear desired footwear or play sports prior to the surgery indicated any hindrance to wearing the aforementioned footwear or performing sporting activities as a result of the interpositional arthroplasty. Table 3 displays clinical results of all the 19 cases that had PROMs analysis (Table 3).
Demographics and PROMS Scores of the 19 Cases With Freiberg’s Disease and Follow-up Results.
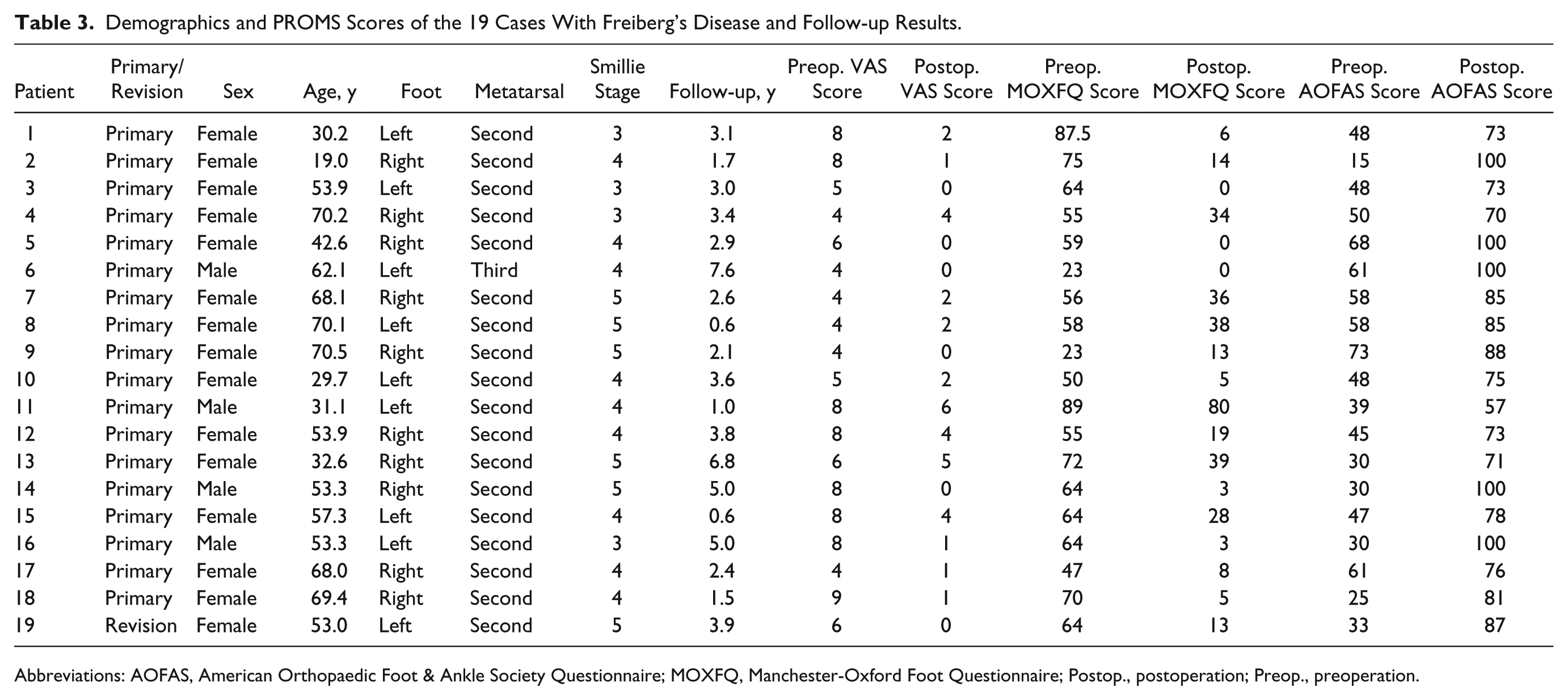
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Questionnaire; MOXFQ, Manchester-Oxford Foot Questionnaire; Postop., postoperation; Preop., preoperation.
The average preoperative VAS score was 6.2 (range 4-9) whereas the postoperative VAS score was 1.8 (range 0-6) demonstrating a significant improvement in pain experience (P < .05). All patients except one reported an improvement in VAS scores with a maximum improvement of 8 points. Only 1 patient had experienced no improvement or worsening in pain following the surgery (Figure 5).
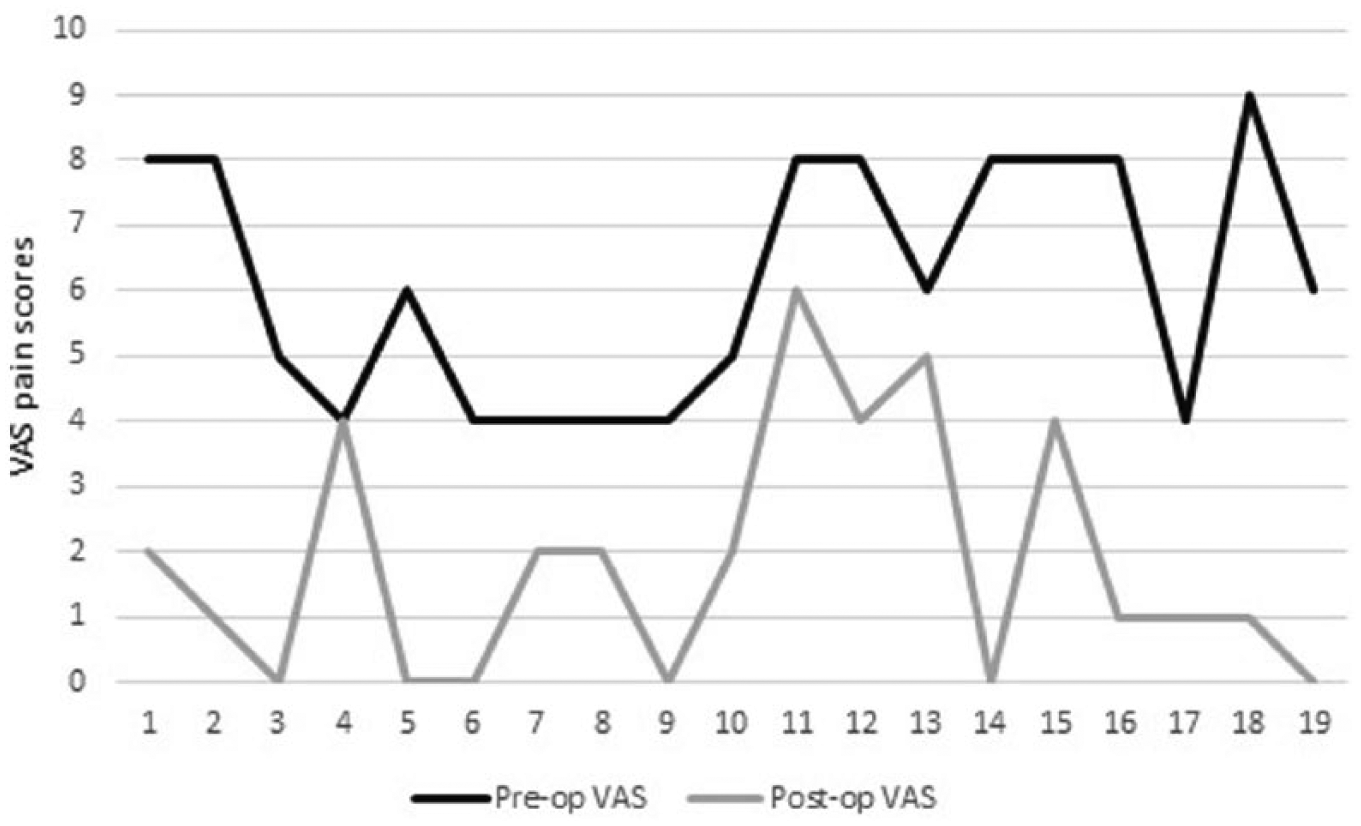
Mean preoperative and postoperative VAS pain scores.
The mean preoperative AOFAS scores were 45.6 (range 15-73) and postoperative AOFAS scores were 82.7 (range 57-100). The postoperative AOFAS scores demonstrated a significant improvement (P < .05), with a maximum improvement of 85 points observed (Figure 6).

Mean preoperative and postoperative AOFAS scores. AOFAS, American Orthopaedic Foot & Ankle Society Questionnaire.
The average preoperative and postoperative MOXFQ scores were 60.0 (range 23-89) and 18.1 (range 0-80), respectively. All cases reported significant improvements in postoperative MOXFQ scores compared with preoperative MOXFQ scores, with the maximum recorded improvement of 82 points (P < .05) (Figure 7).
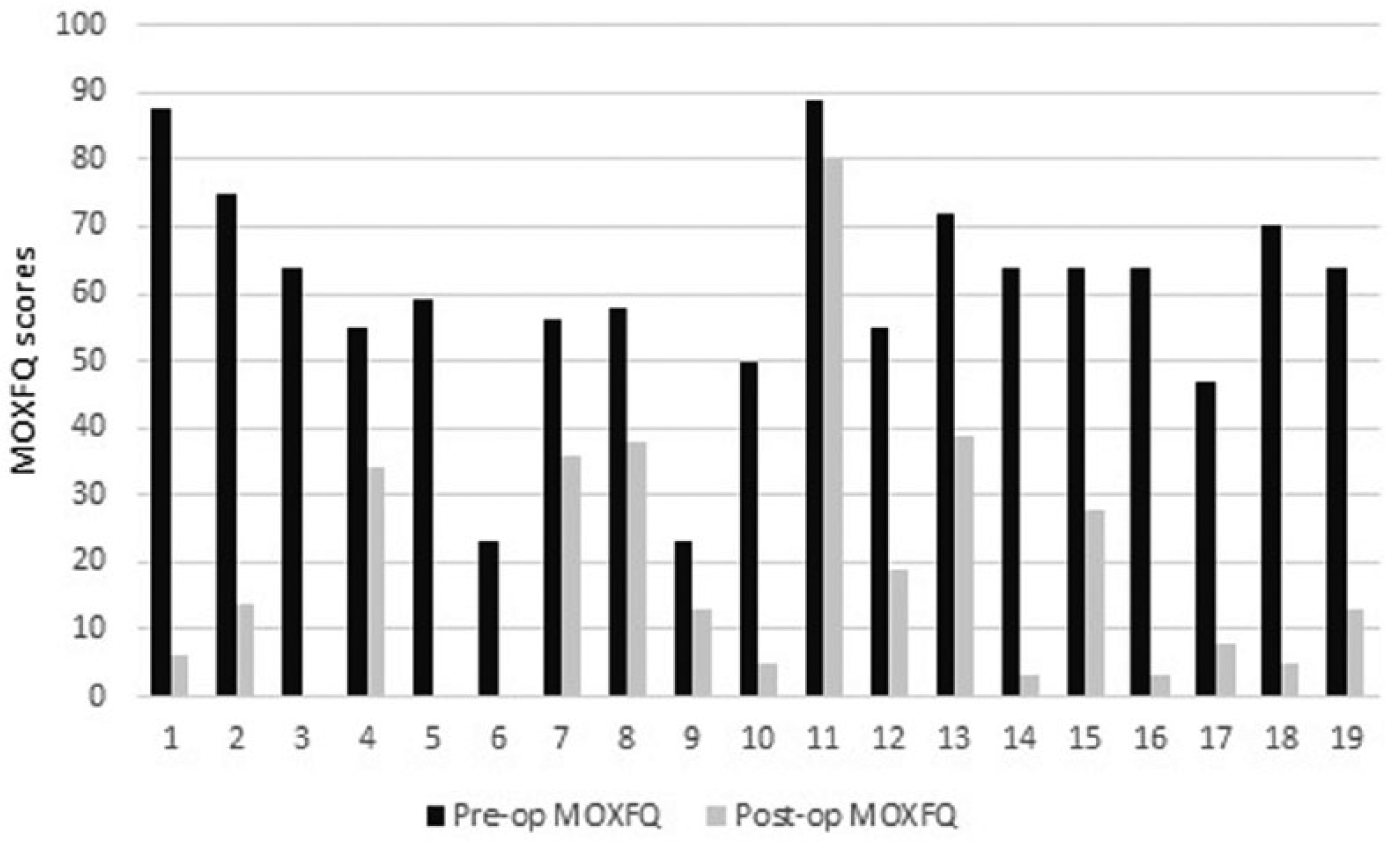
Mean preoperative and postoperative MOXFQ scores. MOXFQ, Manchester-Oxford Foot Questionnaire.
A scatter diagram demonstrated a positive correlation between postoperative differences in MOXFQ and AOFAS scores (r 2 = 0.277) (Figure 8). Table 4 displays the results of Student t tests between mean preoperative and postoperative scores for VAS, MOXFQ, and AOFAS scores (Table 4). In our study, functional outcome was assessed at the final clinical follow-up and then again at the time of study data collection. No patients reported a deterioration in function over time, and good final scores existed throughout the postoperative period. In the lead author’s experience with these patients, clinical function optimized at approximately 4 months. After this point, poor results could be expected to improve very little, but equally good results were maintained in the long term.
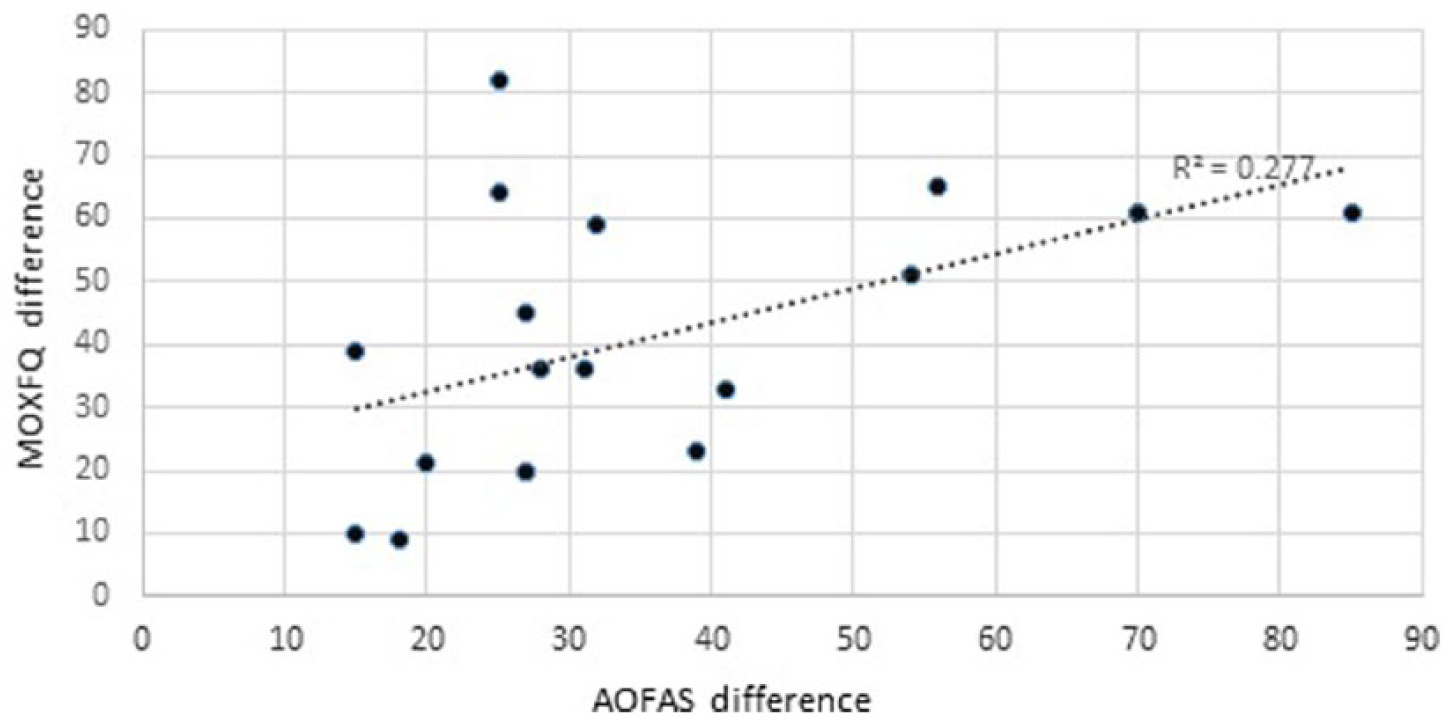
Scatter diagram demonstrating a positive correlative between postoperative MOXFQ and AOFAS scores. Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Questionnaire; MOXFQ, Manchester-Oxford Foot Questionnaire.
Results of Student t Tests.
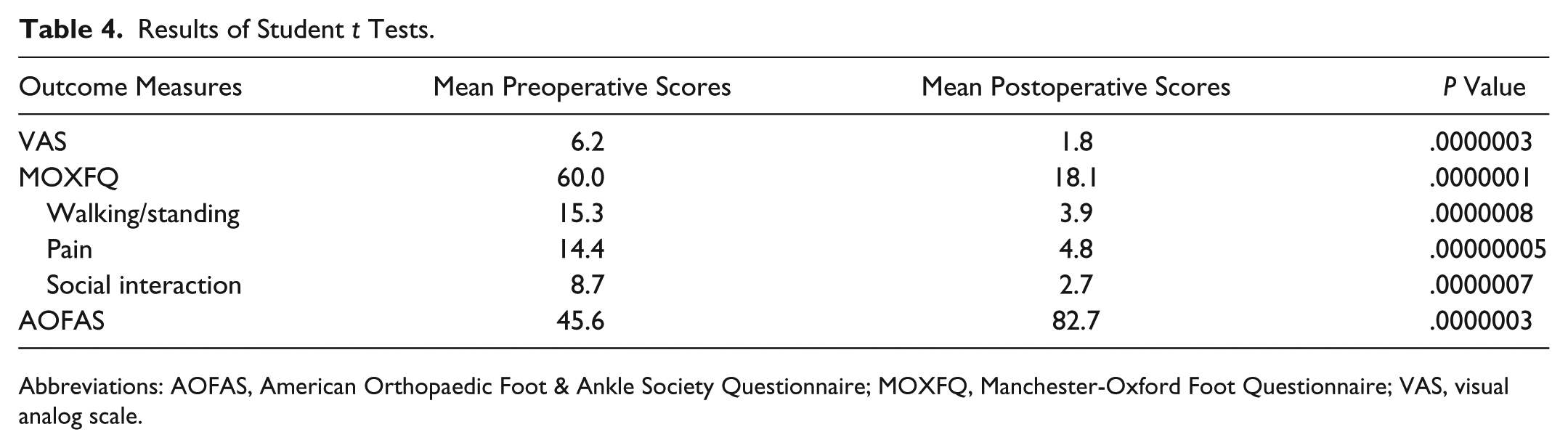
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society Questionnaire; MOXFQ, Manchester-Oxford Foot Questionnaire; VAS, visual analog scale.
Complications
There was only 1 postoperative superficial wound infection, but no cases of transfer metatarsalgia was observed. At the time of final clinical follow-up patients were assessed for joint stability from their history, MTP joint position on standing, MTP shuck test, and tip-toe function and there were no toes with unstable joints.
Discussion
Freiberg’s disease, avascular necrosis of the metatarsal heads, was first described in 1914 by Albert Freiberg when 6 patients complained of forefoot pain during activity. Radiographs subsequently revealed a flattened metatarsal head with sclerosis. 5 Freiberg’s disease, also coined Freiberg’s infraction, is the fourth most common intra-articular osteonecrosis in the body. 25 The etiology of Freiberg’s disease remains unclear but injury, repeated stress from microtrauma, vascular insufficiency, and possible genetic association with conditions including multiple epiphyseal dysplasia have been suggested as possible contributory factors.19,25 Freiberg’s disease is 5 times more common among females than males and commonly affects people aged between 10 and 45 years.12,24 Patients often present with localized tenderness both dorsally and plantarly over the affected MTP joint with tenderness exacerbated by range of motion. Occasionally joint effusion may be present. In late stages of Freiberg’s disease, crepitus, palpable bony prominences, and limited range of motion is observed. 2
Freiberg’s disease classically affects the second metatarsal head in two-thirds of cases, whereas the third metatarsal head is only affected in 27% of cases. The fourth and fifth metatarsals are rarely affected by this disease process. 8 As the second metatarsal is frequently the longest and least mobile, repetitive weight bearing creates excessive pressure on the metatarsal head. This can lead to microfractures, reduced blood supply to the subchondral bone, cartilage deformation, and synovitis. If this persists, range of motion is affected usually with loss of extension of the MTP joint, with abnormal biomechanical stress getting applied to the metatarsal shaft. Finally, metatarsal shaft widening and osteochondral fragmentation at the metatarsal head can occur. 1
Based on macroscopic appearance, Smillie radiographically classified the natural history of Freiberg’s disease into 5 stages, and this is the most referenced system to date. The first stage involves fissuring of the cartilage and is therefore not visible on radiographs. In the second stage, central resorption of the affected metatarsal head occurs. As this progresses, medial and lateral projections are formed at the metatarsal heads, which are seen in stage III. In stage IV, these projections fracture and form loose bodies. Finally, in stage V, the metatarsal head flattens. 26
There are various operative treatments available in the surgical management of Freiberg’s disease. These include core decompression, 6 debridement, 7 metatarsal osteotomies,3,8,10,13,14,16,27 and arthroplasty.20,22 In early the stages of Freiberg’s disease (stages I-III), restoration of joint congruity can be attempted by joint debridement, elevation of depressed fragments, and metatarsal osteotomy.8,9,27 Two recent case series reported good outcomes for osteotomy procedures. Helix-Giordanino and colleagues performed the first osteotomy described for Freiberg’s disease, Gauthier Osteotomy, in 30 consecutive cases and reported good patient satisfaction and AOFAS scores postoperatively. 11 Lee and coworkers reported significant improvements in postoperative VAS and AOFAS scores among patients undergoing Weil and Dorsal closing wedge osteotomy for Freiberg’s disease of the second metatarsal head. 15 In the later stages of this disease process (stage IV and V), it is difficult to restore joint congruity, and therefore joint arthroplasty has been recommended. 29 Despite the various operative treatments described in the literature, no true consensus has been reached with respect to the most optimal surgical management.
Several papers have reported the use of interpositional arthroplasty for Freiberg’s disease using autogenous, allogenic, and synthetic materials. Allografts have the potential for bacterial infection, degradation and activation of the host’s immunologic reaction. 23 Use of autogenous grafts including EDL, 4 EDB,8,22 or palmaris longus 17 can provide good pain relief from metatarsalgia. However, a separate incision is required to harvest the palmaris tendon autograft, which can potentially cause infection, hypertrophic and hypersensitive scar causing shoe irritation and discomfort. 23
To minimize the risk of infection and patient morbidity from separate skin incisions, we modified the interpositional arthroplasty technique using a pedicle of periosteum and fat graft to act as a spacer. We report excellent results amongst our patients who underwent this modified interpositional arthroplasty technique. Twenty-five cases (23 patients) underwent surgery in the study period—23 primary cases and 2 revision cases.
Of the 19 cases undergoing this procedure with complete PROMs, all cases except 1 reported reduction in pain following the surgery. The differences observed between preoperative and postoperative VAS scores were statistically significant (P < .05). All patients reported significant improvement in AOFAS and MOXFQ scores following surgery (P < .05).
This study represents the entire case series of the learning curve. At the beginning of this series, the senior author routinely used a K-wire across the MTP joint in order to stabilize the graft and to hold the toe in position. However in the first 8 patients, stiffness was observed and it was also noted that elevation with movement was much better tolerated than a straight but stiff toe, and so this practice was ceased. The original technique was modified to stabilize the graft by suturing it to the plantar plate and using dressings to hold the toe position for 2 weeks. No cases of joint instability were seen. We have presented the results for all patients including those early patients with transarticular K-wires, even with the inclusion of these patients their results are still favorable.
We did not measure the range of motion preoperatively for all patients. However, we note that the postoperative range of motion was subjectively reported as good with many patients able to wear heels that had been unable to do this preoperatively. Our technique is the only reported interpositional arthroplasty using local tissue that does not disrupt the extensor mechanism by sacrificing one of the tendons. Although we do not have final follow-up data on the specific range of motion, it is our belief that it is in line with the principles of foot surgery to aim to maintain the kinematics by avoiding damage to this mechanism.
El-Tayeby and colleagues treated 13 adolescents (9 females, 4 males) with Freiberg’s disease using interpositional athroplasty with EDL tendon of the affected metatarsal head. Of the 13 cases, 11 involved the second metatarsal with 2 involving the third metatarsal. Prior to surgery, 12 patients complained of either constant severe pain or severe pain with activity whereas 10 patients complained of restriction on walking. Following surgery, the above symptoms resolved, with 10 patients reporting excellent outcomes whereas 11 patients reported pain-free range of motion with no cases of transfer metatarsalgia. However, the authors reported no improvement in range of motion following surgery, with weak extension of the second toe observed in 8 patients following removal of splint. Furthermore, 2 patients complained of hypoesthesia over the skin incision while wearing footwear. 4 As we used periosteum and fat as a spacer instead of EDL, we encountered no cases of weak toe extension or hypoesthesia secondary to skin incision.
Ozkan and coworkers evaluated 10 patients with Freiberg’s disease of the second MTP joint undergoing interpositional arthroplasty using the EDB tendon over 3 years. These patients were followed up between 12 and 36 months postoperatively. The mean AOFAS scores increased by 22.1 points from 58.3 to 80.4 following surgery, whereas 9 of the patients reported good to excellent results. 22 The mean increase in AOFAS scores following surgery was similar to our results whereby an increase of 28 points was observed (43.8-71.8). These results demonstrate that our modified technique can yield similar clinical outcomes without the use of EDB graft. With the “rollmop” graft there was a very generous volume of material that was sufficient to be sutured down to the plantar plate. We have found that the use of EDB limits the graft size.
Another study reported a case of interpositional arthroplasty using palmaris longus tendon grafting for stage V Freiberg’s disease with complete resolution of pain and no metatarsal shortening. Unfortunately, the patient noted a 5° decrease in plantarflexion at 3 months following surgery. 17 Although the range of motion was not formally measured in our study, the use of periosteum and fat as a spacer for the MTP joint instead of palmaris longus avoids the requirement of a separate incision for palmaris longus tendon grafting and thus minimizes donor site morbidity. Furthermore, this modified technique yielded similar results to studies using EDL and EDB and thereby preventing weak toe extension.
Our results demonstrate significant improvements in pain and clinical outcome measures using MOXFQ and AOFAS questionnaires following the use of this modified technique. Furthermore, the results demonstrate that this technique was safe and could produce clinically reliable outcomes. Finally, our study represents the largest cohort of patients with Freiberg’s disease treated with interpositional arthroplasty.
The MOXFQ PROMs questionnaire was validated for use. Although the AOFAS questionnaire was not validated, it was included to allow for comparison with other similar published studies. A limitation of our study is that the final study follow-up was conducted via postal questionnaires, and therefore the final range of motion could not be examined. We therefore only have a patient-reported outcomes in range of motion assessed using a Likert-type scale perioperatively, and as a result we cannot comment on the joint movement. However, this study is not presented as a study on range of motion but an assessment of functional outcomes, specifically with reference to a return to fashion footwear and sports.
Conclusion
This novel technique of interpositional arthroplasty with the use of a “rollmop” local pedicle graft for late-stage Freiberg’s disease produces significant improvements in pain, functional outcomes, and patient satisfaction. Furthermore, it avoided donor site morbidity and allowed patients to return to desired footwear and sporting activities. We believe it is essential to avoid K-wire placement across the MTP joint in order to prevent stiffness, poor clinical outcomes, and joint instability.
Supplemental Material
FAI786494-ICMJE – Supplemental material for Functional Outcomes of Local Pedicle Graft Interpositional Arthroplasty in Adults With Severe Freiberg Disease
Supplemental material, FAI786494-ICMJE for Functional Outcomes of Local Pedicle Graft Interpositional Arthroplasty in Adults With Severe Freiberg Disease by Wahid Abdul, Ben Hickey and Anthony Perera in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.