
Abstract
Background:
The epidemiology of midfoot injuries is poorly known. It has been estimated that the incidence of Lisfranc injuries (intra-articular injury in the tarsometatarsal joint) is 1/55 000 person-years and the incidence of Chopart injuries (intra-articular injury in the talonavicular and calcaneocuboidal joint) 4/100 000 person-years. The purpose of our study was to assess the computed tomography (CT) imaging–based incidence (per 100 000 person-years) and trauma mechanisms of midfoot injuries.
Methods:
All CT studies performed due to acute injury of the foot and ankle region between January 1, 2012, and December 31, 2016, at Tampere University Hospital were reviewed. Patients presenting with an injury in the midfoot region in the CT scan were included in this study, and their records were retrospectively evaluated to assess patient characteristics.
Results:
During the 5-year study period, 953 foot and ankle CT scans were obtained because of an acute injury of the foot and ankle. Altogether, 464 foot injuries were found. Of these, 307 affected the midfoot area: 233 (75.9%) the Lisfranc joint area, 56 (18.2%) the Chopart joint area, and 18 (5.9%) were combined injuries or miscellaneous injuries in the midfoot. The incidence of all midfoot injuries was 12.1/100 000 person-years. The incidence of Lisfranc injuries was 9.2/100 000 person-years. The incidence of Chopart injuries was 2.2/100 000 person-years.
Conclusions:
The incidence of Lisfranc injuries was higher and the incidence of Chopart injuries lower than previously estimated. More than two-thirds of the midfoot injuries in this study were nondisplaced (<2 mm displacement in fracture or joint) and were caused by low-energy trauma.
Level of Evidence:
Level III, epidemiologic study.
Lisfranc injury was originally described as a partial or complete dislocation of the tarsometatarsal (TMT) joints by Quenu and Kuss in 1909. 18 Nunley and Vertullo 16 described that the injury can also be subtle when there is no detectable dislocation in nonweightbearing radiographs. Recently, however, Chiodo and Myerson 2 introduced a new approach to these injuries where they suggested to divide the injuries in medial (TMT 1), central (TMT 2-3), and lateral (TMT 4-5) columns. Lau et al 10 completed the columnar approach with a classification where the prognosis of injury is related to number of affected columns and displacement (less or more than 2 mm) instead of the diastasis between I and II TMT joints. Main and Jowett 13 developed a classification for Chopart injuries, where they stated that these injuries vary from small avulsion fragments to severe subluxation of the whole joint. Diagnostics have become more precise as a result of the more common use of computed tomography (CT). It is unclear whether there is such a type of injury as “purely ligamentous injury,” or whether is it detectable from bony avulsion fragments.7,8,17 The definitions and classifications of these injuries has changed, and still, 100 years after the first classification there is no clear consensus on how these injuries should be defined. 20
The epidemiology of midfoot (Lisfranc and Chopart joint) injuries is poorly known.3,5 It has been estimated that Lisfranc injuries account for 0.2% of all fractures, and the annual incidence is reported to be 1/55 000 person-years.1,6 It has also been estimated that between 20% and 24% of midfoot injuries are undiagnosed during initial clinical examination.2,8,14,26,27 The 2 most cited studies of Lisfranc injury incidence were published in the early 1960s.1,6 In a study by Aitken and Poulson 1 published in 1963, 16 patients with Lisfranc injury were treated during a 15-year period in a hospital where 5500 fractures were treated annually. In a study by English 6 in 1964, there were 24 Lisfranc injuries among 11 000 fractures, which gives an incidence rate of 0.2% of all fractures. These 2 studies are often cited when the incidence rate of 1/55 000 person-years for Lisfranc injuries is presented. However, the authors who cite these studies fail to provide any basis or supporting data for how they achieved this figure. In a study by Court-Brown et al, 3 116 midfoot injuries (navicular, cuneiform and cuboid) were treated in 113 patients during a 5-year period in a catchment area of 650 000 residents. The resulting incidence rate for midfoot injuries diagnosed with plain radiographs was 3.6/100 000 person-years. A study by Richter et al 22 reported that the proportion of combined (Lisfranc-Chopart) injuries of the midfoot was 16.8% of all midfoot injuries, and such injuries are often caused by high-energy trauma. The incidence of these injuries is, however, still unknown. Because the International Statistical Classification of Diseases and Related Health Problems (ICD) offers no codes for midfoot injuries, it is impossible to conduct a register-wide epidemiological study.
Lisfranc injuries are traditionally divided into subtle and severe injuries based on the trauma mechanism.16,21,28 Subtle injuries are suggested to be the result of indirect low-energy trauma, such as twists and sprains that often occur during sports.15,16 Severe injuries are thought to result from high-energy trauma, such as traffic accidents, falling from height, or direct crush injuries. 15 Subtle injuries present a significant diagnostic challenge because it has been suggested that ligamentous injuries are impossible to detect without weightbearing. 16 The previous classification of Lisfranc injuries by Myerson 14 is based on plain radiographs and the classification by Nunley and Vertullo 16 is based on weightbearing radiographs. CT and magnetic resonance imaging (MRI) are now recommended to be used for defining midfoot injuries. There is, however, no consensus as to when these modalities should be used or how the findings should be interpreted.7,8,12,25 The aim of this study was to assess the CT-based incidence (per 100 000 person-years) and characteristics of midfoot injuries at a Level I trauma hospital, which was the only public hospital providing acute trauma care for the half-million residents of the region.
Methods
To assess the incidence of midfoot injuries, all CT studies (traditional CT or cone-beam CT) performed due to acute injury to the foot and ankle region during a 5-year period (January 1, 2012, to December 31, 2016) were reviewed. Patients presenting with an injury to the midfoot region in CT scans were included in the study. In accordance with hospital policy, CT was always performed when there was an intra-articular fracture or midfoot joint displacement in radiographs or a high suspicion of midfoot injury based on clinical examination. Patient records were retrospectively evaluated to assess patient characteristics, trauma mechanism, primary radiologic findings, associated injuries, and treatment. Patients with injuries older than 30 days, isolated fractures of the fifth metatarsal base, injuries only in the distal foot (simple metatarsal fractures or injuries only in the metatarsophalangeal joint or toe region), or patients residing outside the catchment area were excluded from the study.
To compute the incidence of injuries, the annual population of the Pirkanmaa region was obtained from Official Statistics of Finland, an electronic population register of the country. The injury incidence was calculated by the annual number of injuries with the population of the region, which was 509 279 residents in December 2016. The incidence is presented per 100 000 person-years.
Tumbling or slipping, tumbling on stairs and sports-related activities were considered to be low-energy trauma mechanisms. Falling from height, direct injury and traffic collisions were considered to be high-energy trauma mechanisms. Midfoot injuries were divided into Lisfranc (tarsometatarsal joint, TMT) and Chopart (talonavicular and calcaneocuboid joint) injuries. Intra-articular and avulsion fractures of the TMT were considered to be Lisfranc injuries (Figure 1). Extra-articular fracture of a metatarsal base was not defined as Lisfranc injury. Fractures and avulsions affecting the talonavicular and calcaneocuboid joints were considered to be Chopart injuries (Figure 2). Combined or miscellaneous injuries were injuries that affected both anatomic areas or injuries that could not be classified as pure Lisfranc or Chopart injuries.

(A-D) Computed tomographic findings of Lisfranc injury.

(A-D) Computed tomographic findings of Chopart injury.
The injuries were classified into 2 groups based on the displacement of the fracture or the dislocation of the affected joint measured from CT scans. Displacement of 2 mm or below was considered a nondisplaced injury, and over 2 mm a displaced injury. Lisfranc injuries were also classified based on the Myerson classification for Lisfranc injuries where possible. 14
Categorical variables were compared with chi-square test. Confidence interval was 95%, and therefore P values <.05 were considered to be statistically significant. Statistical analysis was performed using IBM SPSS Statistics, version 22.
Results
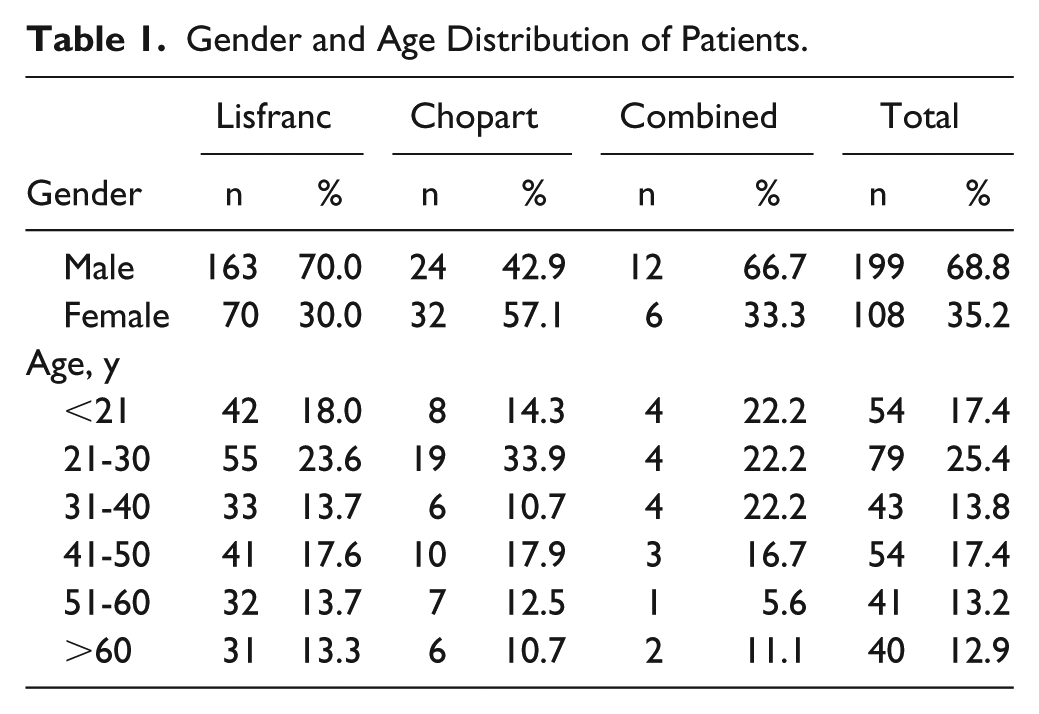
During the 5-year study period, 953 foot and ankle CT scans were obtained for acute injuries to the foot and ankle (Figure 3). Of these, 307 injuries affected the midfoot: 233 (75.9%) in the Lisfranc joint area, 56 (18.2%) in the Chopart joint area, and 18 (5.9%) were combined injuries or miscellaneous injuries in the midfoot. Of all patients presenting with midfoot injuries, 199 (68.8%) were male and 108 (35.2%) female (Table 1). Males were more likely to have Lisfranc injuries (70% vs 30%, P < .001) and females were more likely to have Chopart injuries (57% vs 43%, P < .0001). Differences between gender was not found in combined or miscellaneous injuries (67% vs 33%, P < .866). The male-female ratio was 1.8:1. The mean age of the males was 35.7 (9-88) years and 42.5 (10-76) years for females. In total, 25.4% of all midfoot injuries occurred in the 21 to 30 years age group. Concomitant foot or ankle injuries were found in 37 (12.1%) of the patients. Of all midfoot injuries, 73 (23.8%) were displaced more than 2 mm in CT and 234 (76.2%) were nondisplaced (less than 2 mm).
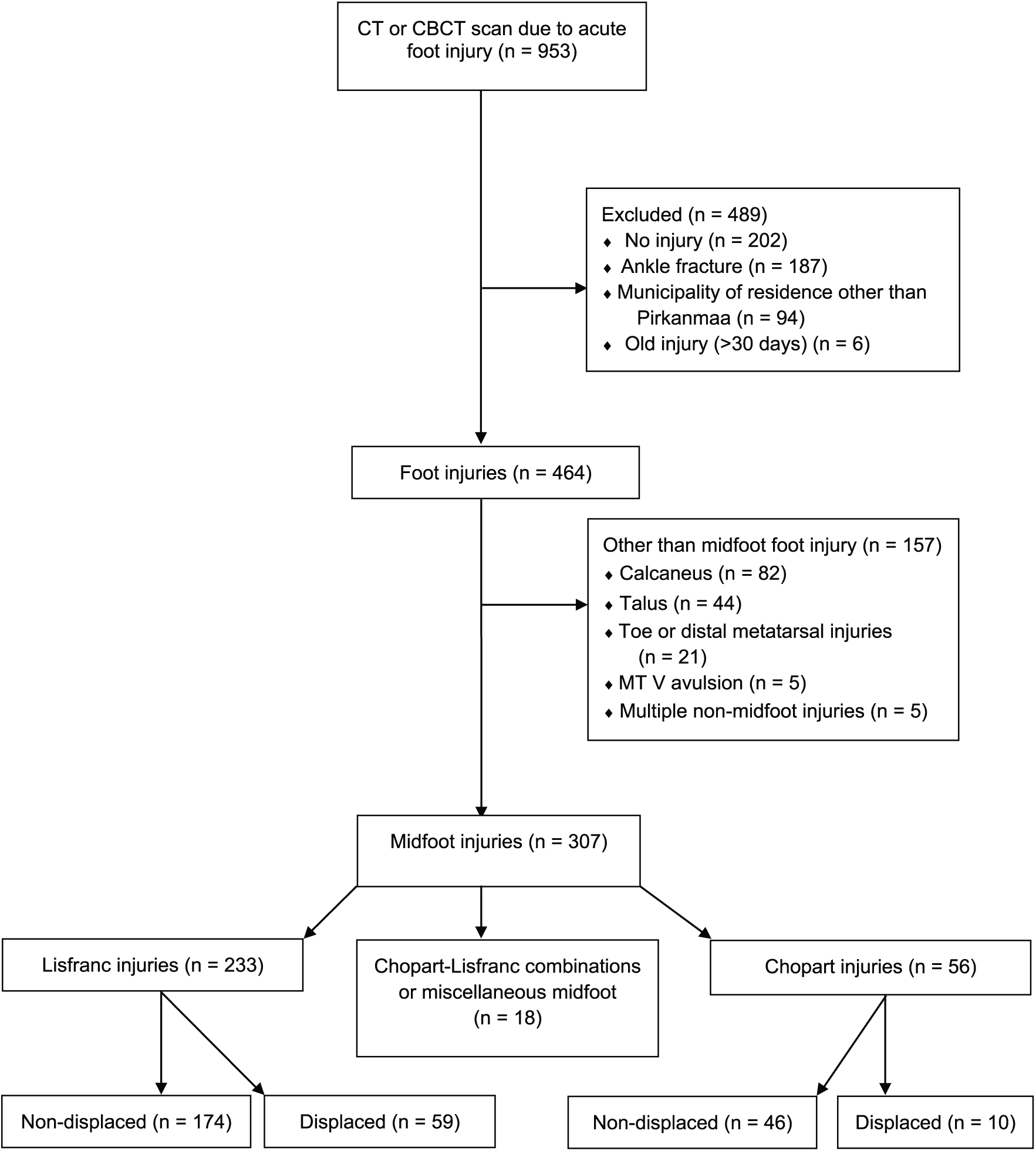
Flow chart of the study.
Gender and Age Distribution of Patients.
The incidence of all midfoot injuries in our study was 12.1/100 000 person-years. The incidence of Lisfranc injuries was 9.2/100 000 person-years while the incidence of Chopart injuries was 2.2/100 000 person-years. The occurrence of Chopart-Lisfranc combinations or miscellaneous injuries was rare, being 0.7/100 000 person-years.
The most frequent trauma mechanisms for Lisfranc injury were tumbling or slipping (36.9%) or direct injury (15.5%) (Table 2). Traffic accidents included 25 (92.6%) motorcycle accidents, and 2 (7.4%) car accidents. The “other” mechanism group comprised bicycle accidents (n=7), falling from chair (n=6), kick toward a solid object (n=5), and unknown mechanism (n=2). Low-energy trauma mechanisms caused 128 (54.9%) of the Lisfranc injuries and high-energy trauma mechanisms caused 85 (36.5%) of the injuries. We were not able to classify 20 (8.6%) injuries by trauma mechanism. No association between trauma energy and the severity of the injury (nondisplaced/displaced) was found in Lisfranc injuries (P = .069). Males had a higher rate of high-energy Lisfranc injuries than females (49% vs 19%, P < .0001).
Trauma Mechanisms of Midfoot Injuries.
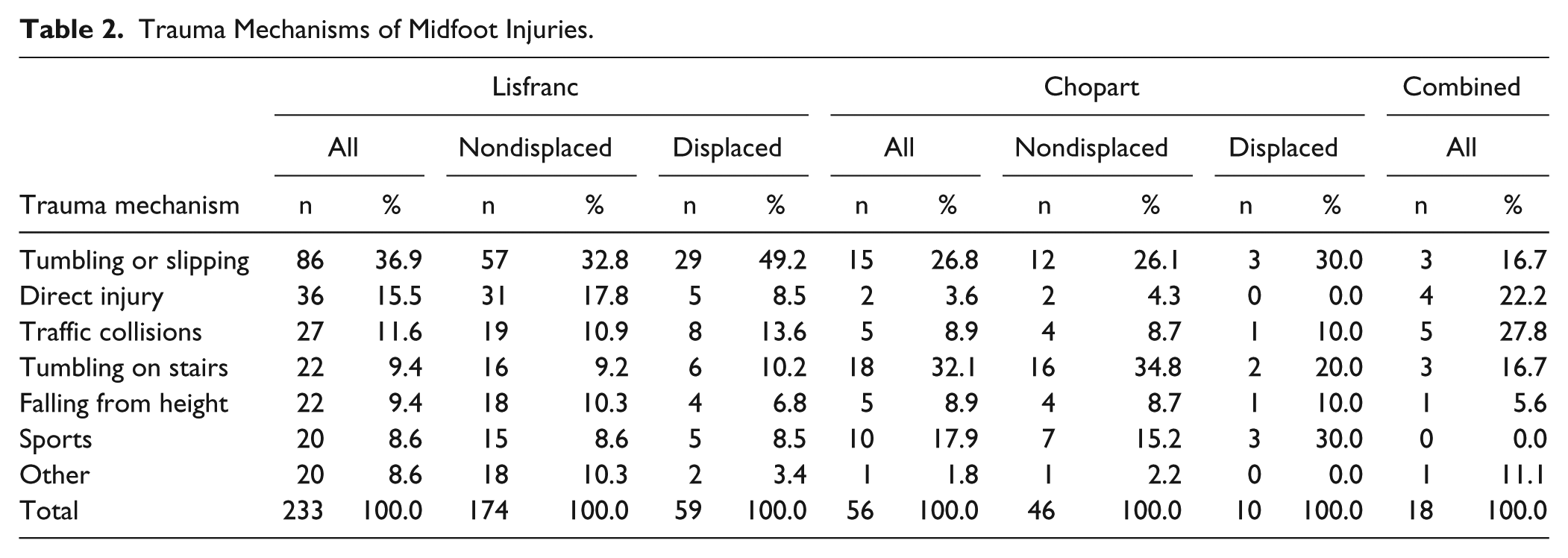
Displaced Lisfranc injuries accounted for 25.3% (n=59) of all Lisfranc injuries. The most frequent trauma mechanism in displaced injuries was tumbling or slipping (n=29, 49.2%) (Table 2). Nondisplaced Lisfranc injuries accounted for 74.6% (n=174) of all Lisfranc injuries. The most frequent trauma mechanisms for nondisplaced injuries were tumbling or slipping (32.8%), direct injury (17.8%), and traffic collisions (10.9%) (Table 2).
Of all Lisfranc injuries, only 13 (5.6%) injuries were displaced in such a way that they could be classified with the Myerson classification. The most frequent injury types were A (n=7, 53.8%), B2 (n=3, 23.1%), B1 (n=2, 15.4%), and C2 (n=1, 7.7%). Type C1 was not found in our study. Altogether, 220 (94.4%) injuries were not classifiable according to the Myerson classification. According to the Lau classification, 1 column was injured in 68 (29.2%) cases, 2 columns in 92 (39.5%) cases, and all columns in 73 (31.3%) cases (Table 3). Medial column was injured in 138 (59.2%) cases, central column in 195 (83.7%) cases, and lateral column in 138 (59.2%) cases.
Classification of Lisfranc Injuries by Lau.
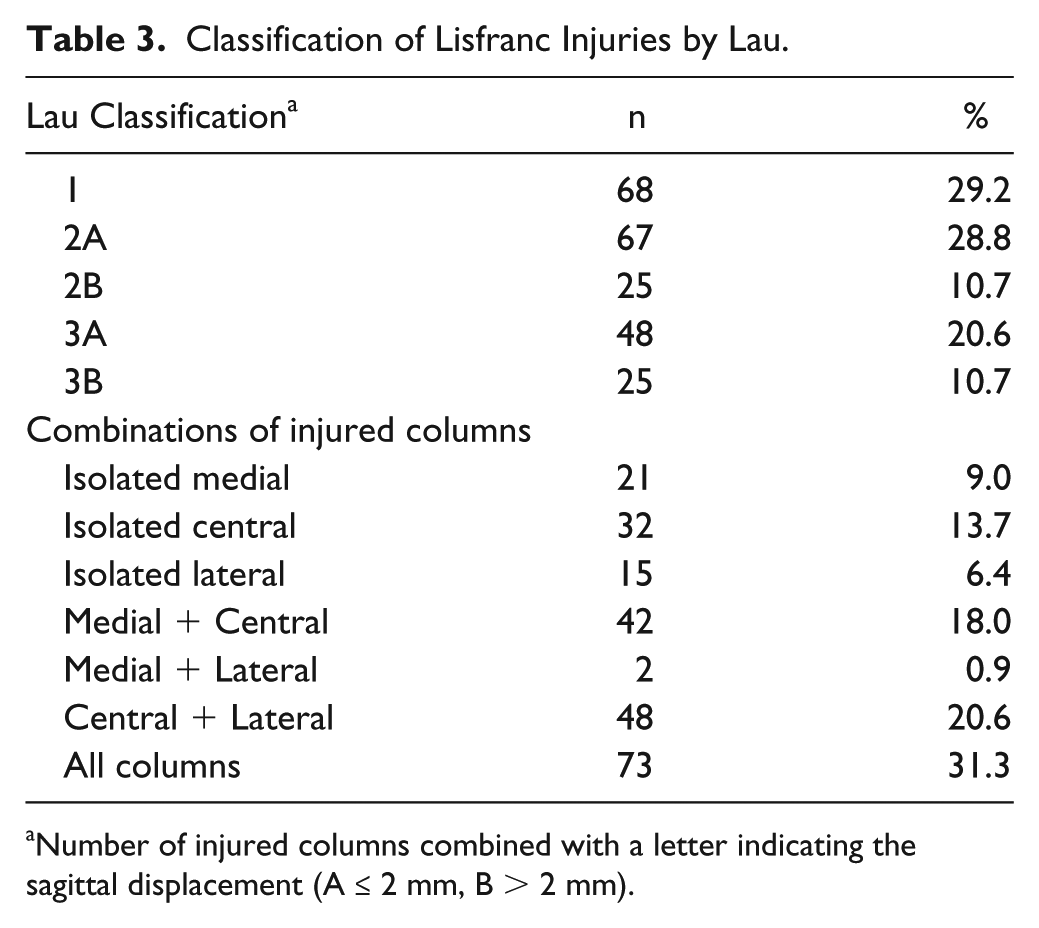
Number of injured columns combined with a letter indicating the sagittal displacement (A ≤ 2 mm, B > 2 mm).
Most of the Chopart injuries were nondisplaced (n=46, 78.0%), and most of the nondisplaced injuries were the result of low-energy trauma mechanisms, such as tumbling on stairs (n=16, 34.8%) and tumbling or slipping (n=12, 26.1%). Ten patients (22.0%) had displaced Chopart injuries. The most frequent trauma mechanisms for displaced injuries were sports-related activities (n=3, 30.0%) and tumbling or slipping (n=3, 30.0%) (Table 2).
The most frequent trauma mechanisms for Chopart-Lisfranc combinations or miscellaneous injuries were traffic collisions (n=5, 27.8%) and direct injury (n=4, 22.2%) (Table 2). Only 4 (25%) of these patients had displaced injuries.
Discussion
To our knowledge, this is the first CT-based study on the incidence of midfoot fractures. The strengths of our study are the precise imaging and diagnostics of these injuries. There is an ongoing RCT on Lisfranc injuries at our hospital, and therefore the awareness of these injuries in our institution is probably higher than on average. Our indication for CT imaging of the foot in acute trauma is an intra-articular injury or midfoot displacement seen in radiographs or a high suspicion of a midfoot injury based on clinical findings. Typical clinical findings of Lisfranc injury are swollen midfoot, tenderness and pain in the midfoot during movements and weightbearing, and plantar ecchymosis.4,24 Although not a nationwide study, the present study is significantly larger than any of the previous studies on the incidence of midfoot injuries. The weakness of this study is that MRI or weightbearing radiographs were not obtained, therefore some purely ligamentous injuries could have been missed. There are no studies where purely ligamentous injuries were scanned with CT, therefore it is not certain that purely ligamentous injuries would not include avulsion fractures that could not be detected under CT. In addition, even though severe foot injuries in our catchment area are mainly diagnosed and treated in our hospital, it is possible that some injuries may also be treated in private hospitals or public health centers. Therefore, our findings might underestimate the true incidence of midfoot injuries.
In our study, the annual incidence of Lisfranc injuries was 5 times higher than previously suggested.1,6 Even the incidence of displaced fractures was 1.3 times higher than the numbers presented in earlier studies. In a 10-year Finnish study, Vuori and Aro (1993) 28 reviewed 750 plain radiographs of treated tarsometatarsal injuries or metatarsal fractures from a catchment area of 250 000 residents at Turku University Hospital. A total of 66 Lisfranc injuries were found during this 10-year period, giving an incidence of 2.6/100 000 person-years compared with an incidence of 9.2/100 000 person-years in our study. The incidence of Chopart injuries, in turn, was slightly lower compared with earlier studies (2.2/100 000 person-years vs 3.6/100 000 person-years 3 ). All previous studies have been based on plain radiographs, and thus the proportion of undiagnosed injuries will have been higher than in our CT-based study. The higher incidence of Lisfranc injuries in our study is probably the result of increased knowledge of midfoot injuries and the better availability of CT imaging. The low incidence of Chopart injuries seen in our study compared with earlier studies probably results from the differences in injury definitions. The widely cited study by Court-Brown et al (2006) 3 included midfoot (navicular, cuneiform and cuboid) injuries, whereas we concentrated on injuries affecting the Chopart joint. Therefore, we may conclude that the present study is the first to investigate the incidence of Chopart joint injuries.
Lievers et al (2012) 11 conducted a literature review of Lisfranc dislocations. The most frequently reported injury mechanisms were traffic accidents (43%), fall from height (24%), direct crush (13%), sports (10%), and equestrian (1%). In our study, the most common trauma mechanism for Lisfranc injury was tumbling or slipping (37%). This mechanism was more than 2 times more frequent than direct injury (16%) and 3 times more frequent than traffic collisions (12%). Age distribution and gender ratio were quite similar in our study compared with Lievers et al’s analysis: about half of the patients were less than 35 years old, male-female ratio was 2:1. Their study showed that the injury mechanism was significantly related to age and sex. Crushing injuries (m/f 8) and motorcycle crashes (m/f 7) were significantly more prevalent in males, whereas low-energy falls were more prevalent in females (m/f 0.77). This finding is in line with the results of our study, as males sustained Lisfranc injuries from high-energy trauma mechanisms more often than females. Most of the traffic collisions were motorcycle accidents (93%). Of the 66 Lisfranc injuries found in the study by Vuori and Aro (1993), 28 12 (18%) were total dislocations, 47 (71%) were classified as partial dislocations, and 7 (11%) as subtle Lisfranc injuries based on the classification by Quenu and Kuss. 18 In their study, one-third of all Lisfranc injuries were caused by low-energy trauma mechanism. In our study, however, the number of subtle injuries (75%) and the proportion of injuries caused by low-energy trauma (55%) were significantly higher.
The traditional Lisfranc injury classifications by Quenu and Kuss (1909), 18 Hardcastle (1982), 9 and Myerson (1986) 14 are based on findings in plain foot radiographs. Basically, these classifications describe the pattern and direction of the displacement of bones in the Lisfranc joint region. Only 6% of patients in our study could be classified according to the Myerson 14 classification. Furthermore, none of the classifications have been useful in predicting outcomes or choosing the right treatment for Lisfranc injury. 29 The classification by Nunley and Vertullo (2002) 16 was developed primarily for low-energy trauma. The classification is based on the weightbearing radiographs of 15 patients with a “midfoot sprain” injury in the Lisfranc region 16 that are classified into 3 different stages. The classification has a few limitations: weightbearing may be impossible because of pain in the injured foot, and the sensitivity of plain radiographs is low when compared with CT.8,28 Therefore, more research on the clinical importance of the findings in CT and MRI studies and the treatment of the subtle injuries in the midfoot region is needed. Since these classifications, Chiodo and Myerson (2001) 2 and Lau et al (2017) 2 have changed the approach to these injuries. They have introduced a column-based classification, which also accounts for the subtle injuries and it is applicable with CT. Yet the evidence on how well the classification leads toward the best treatment is scarce, although the classification provides a fresh perspective on these injuries.2,10
Some authors classify these injuries as “high-energy” and “low-energy” based on the trauma mechanism.19,21,23 Renninger et al 21 studied the differences between low- and high-energy injuries. Low-energy injuries included athletic activity, ground-level twisting, and fall from less than 4 feet. High-energy injuries included motor vehicle crash, motorcycle crash, direct crush, and fall from greater than 4 feet. They reviewed all operatively treated Lisfranc injuries at a single military tertiary referral center for 5 years. Patients with high-energy injuries were more likely to have concomitant nonfoot fractures (37% vs 6%), concomitant foot fractures, cuboid fractures (31% vs 6%), metatarsal base fractures (84% vs 29%), displaced intra-articular fractures (59% vs 4%), and involvement in all TMT joints (23% vs 6%). We did not find any association between trauma mechanism and energy and the severity of the injury. This may be because energy affecting the foot is difficult to evaluate.
In conclusion, the incidence of Lisfranc injuries was significantly higher than previously thought. This finding could result from increased knowledge concerning midfoot injuries and more precise imaging (CT). Up to three-quarters of the midfoot injuries in our study population were nondisplaced injuries. No association was found between trauma energy and the displacement of the fracture. Therefore, we suggest that the classification of these injuries should be based on radiologic findings rather than on trauma energy. More research is needed on the treatment of these subtle injuries because the current classifications and the literature on the treatment of midfoot injuries focus mainly on more severe or displaced injuries.
Supplemental Material
FAI799741-ICMJE – Supplemental material for Incidence and Characteristics of Midfoot Injuries
Supplemental material, FAI799741-ICMJE for Incidence and Characteristics of Midfoot Injuries by Ville T. Ponkilainen, Heikki-Jussi Laine, Heikki M Mäenpää, Ville M. Mattila and Heidi H. Haapasalo in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital, Grant number 9R006 and R9031. Sosiaali- ja Terveysministeriö 9R006, R9031.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.