
Abstract
Background:
The evidence regarding the prevalence of deep vein thrombosis (DVT) after foot and ankle surgery in elective patients that need to be 6 weeks non–weight bearing postoperatively is incomplete and has limitations.
Methods:
The prevalence of DVT in 114 procedures involving the hindfoot and midfoot was determined using ultrasonographic surveillance at 2 and 6 weeks after surgery.
Results:
The prevalence of DVT was observed to be 25.4%. The majority (68.9%) of DVTs were diagnosed at the ultrasonographic scan performed 2 weeks postoperatively. The remainder (31.1%) of DVTs were diagnosed at the 6-week postoperative ultrasonographic scan. At least 75% of the patients who had early and late DVT had no clinical symptoms or signs of DVT. The prevalence of DVT in clinically detectable patients was 6%. The average age of patients with early DVT was 62.2 years, significantly higher compared to those who had no DVT. The mean tourniquet time for patients with early DVT was 68.1 minutes, significantly higher compared to those without DVT. All DVTs detected were distal to the popliteal vein.
Conclusions:
The prevalence of clinically silent DVT was significantly higher than was previously thought. We believe this increased rate is directly attributable to the use of ultrasonographic surveillance postsurgery both at 2 and 6 weeks. The risk of DVT continued after the 2-week visit, and 30% of the DVTs were detected at the ultrasonographic scan at 6 weeks.
Level of Evidence:
Level II, prospective cohort.
Introduction
Foot and ankle surgery has a wide variety of procedures involving the ankle, hindfoot, midfoot and forefoot. The evidence regarding the prevalence of deep vein thrombosis (DVT) after foot and ankle surgery is conflicted.2,6,11,14,26,35,36 The incidence of DVT in foot and ankle surgery has been reported between 0.22% and 8.46%, 32 with 0.15% developing into nonfatal emboli.6,11,26,36 A systematic review by Mangawani et al 22 and a meta-analysis by Calder et al 3 stated that the overall incidence of DVT in foot and ankle surgery is low; however, the studies that met their criteria for inclusion are an assortment of retrospective studies that include the nonoperative management of trauma, surgery to all parts of the foot or ankle relying on the clinical diagnosis of DVT as well as a retrospective review of charts based on a coding system.
A review of the studies that investigated the prevalence of DVT in foot and ankle surgeries revealed that most authors base their findings on clinical assessment of their patients or chart review.2,11,15 Clinical examination has been found to be inaccurate in the diagnosis of DVT as most are asymptomatic. 36 This leads to underreporting of cases.32,36 Solis and Saxby 36 performed postoperative duplex ultrasonography on both lower extremities of 201 patients undergoing surgery of the foot or ankle, excluding those with prior DVT. Ultrasonographies were performed on the first follow-up visit, an average of 10.5 days postoperatively. Deep clots were found in only 3.5% of their subjects; however, most (47%) of their subjects underwent forefoot procedures, which allow patients to bear weight through their heels postoperatively. Saragas et al 32 did not detect any DVT in 86 of their patients who underwent forefoot procedures and were weight bearing postoperatively. No study has been published that prospectively looks at a group of low-risk patients undergoing elective ankle and hindfoot surgery that requires 6 weeks non–weight bearing postoperatively.
It is our belief that the risk of DVT in patients undergoing elective ankle and hindfoot surgery who are non–weight bearing for 6 weeks is much greater than the literature suggests because of serious limitations in the previous studies outlined above. Therefore, determining the true prevalence of DVT after elective foot and ankle surgery in low-risk patients who are non–weightbearing postoperatively is an important endeavor. This article prospectively determined the prevalence of DVT formation using ultrasonographic surveillance at 2 and 6 weeks postoperatively in these low-risk patients and compared the prevalence on clinical grounds. There has been no study published that has prospectively determined the risk of a DVT with ultrasonographic surveillance in this group of patients.
Methods
The study population consisted of patients older than 16 years who were recruited prospectively from the senior author’s private practice. All patients had elective surgery of the foot or ankle performed by the senior author, requiring a minimum of 6 weeks postoperative non–weight bearing. The following exclusion criteria were utilized:
Patients undergoing surgery for Achilles tendon ruptures
Patients undergoing surgery for acute trauma of the foot and ankle
History of previous DVT or thromboembolic events
Family history of DVT (first-degree relative)
Current use of anticoagulant/antiplatelet agent therapy within 6 weeks prior to surgery
Known thrombophilia
Active malignancy
Heart, liver, or renal failure
Currently pregnant
The exclusion criteria were compiled from previously identified factors that increase the risk of DVT1,2,32 and input from the senior vascular physician (A.O.).
After securing approval from our institution’s Practice Development and Research Council, consecutive patients were recruited from November 2014 to March 2017 as they presented to the clinic. Eligible patients were contacted prior to their scheduled surgery and informed about the study. Informed consent was obtained before surgery. The senior author performed all surgeries from November 2014 to April 2017. Following the surgery, subjects were non–weight bearing with axillary crutches or knee walker mobility scooter, and scheduled for follow-up at 2 weeks and 6 weeks postoperatively.
A total of 111 patients who underwent 114 procedures were eligible and subject to analysis. 209 patients undergoing elective surgery were considered for participation in the study. 83 patients were excluded based on the exclusion criteria. Eleven patients refused participation in the study and 4 were excluded because they would need anti-coagulation for long travel immediately after surgery. Three patients had surgeries for both feet, 1 year apart. Both surgeries were included in the study and were counted as different procedures. The majority of the subjects (66%) were female, with a mean age of 51.7 years (17-79 years).
Prophylaxis for DVT was withheld for the entire 6-week duration for all subjects included in the study; this included the use of Aspirin. Mechanical prophylaxis was used for the contralateral extremity during the procedure and for the duration of their hospital stay. To ensure statistical significance of the conclusions, sample size was computed based on Saragas et al, 32 using SigmaStat software. A sample consisting of 113 patients provided a conclusion with a power of 0.8 at 95% confidence. t tests were used to compare means ± SD, with the significance level set at P <.05.
The investigators were well trained in looking for DVT. They assessed for symptoms and signs of DVT at the follow-up visit 2 weeks postoperatively. Episodes of calf pain, abnormal leg swelling, cramping, breathlessness, chest pain, or confusion were recorded as these are common symptoms of DVT and its sequelae.3,9,10,12 Ultrasonographic examination of the operated extremity was done at our vascular laboratory. The vascular laboratory performs in excess of 10 000 DVT scans a year as we are part of a major Tertiary Referral Institution. Qualified technicians using a Philips EPIQ 5 or Siemens S2000 ultrasonographic machine performed the examination. A middle frequency (4-9 MHz) transducer was used in most cases; however, a lower frequency transducer was used for obese or swollen legs. The test required the patient to remove their shoes, trousers, and splint. The thigh was examined with the patient in semirecumbent position and the calf was examined with the patients in an upright-seated position, with the lower leg over the side of the bed and dependent. If the scan was negative for DVT, the patient’s leg was placed in a short leg cast or CAM (controlled ankle motion) walker boot and non–weight bearing status was maintained until the second follow-up at 6 weeks after surgery. At the 6-week follow-up, the ultrasonographic process was repeated.
Patients with positive ultrasonographic scans at 2 weeks postoperatively were classified as having early DVT. Patients diagnosed to have DVT by ultrasonography were referred to a vascular physician for further evaluation and treatment. If the patient was positive for DVT at 2 weeks, the findings were recorded and they were no longer in the study. Their follow-up was carried out by the vascular physician. The remaining patients were scanned at 6 weeks postoperatively. The DVTs diagnosed at the 6-week visit were classified as late DVT.
Results
The overall prevalence of DVT was observed to be 25.4% (29/114). The majority 20/29 (68.9%) of DVT were diagnosed at the ultrasonographic scan performed 2 weeks postoperatively (early DVT; Table 1). The remainder 9/29 (31.1%) of procedures had DVT diagnosed only at the sixth week postoperative visit (Late DVT, Table 1). All DVT detected were below the knee. For patients who had DVT, 51.7% were female, and 48.3% were male. The average age of patients with early DVT was 62.2 years ± 11.1 SD, which was significantly higher compared to those who had no DVT 49.1 years ± 16.1 SD (P = .0008). The average age of patients with late DVT was 54.1 years ± 13.1 SD, which was not significantly different from those without DVT (P = .371). Of the 114 procedures in the study, only 7 DVTs were diagnosed on clinical grounds. This represents 6% of the total number of patients in the study. In 12 of the 29 procedures there were multiple DVTs. DVT occurred at the junction of the popliteal vein in 1 case, in the posterior tibial vein in 5 cases, in the peroneal vein in 10 cases, and in the soleal vein in 24 cases. There were no pulmonary emboli in this group.
Distribution of Early and Late Deep Vein Thrombosis (DVT) Patients.
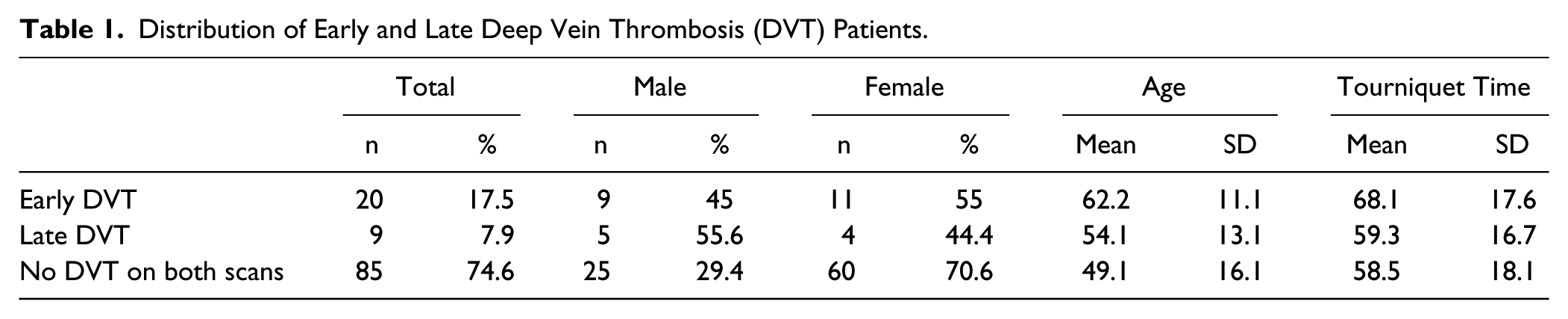
The mean tourniquet time for patients with early DVT was 68.1 minutes ± 17.6 SD which was significantly higher compared to those without DVT, which was 58.5 minutes ± 18.1 SD (P = .034). The tourniquet time for patients with late DVT was 59.3 minutes ± 16.7 SD (Table 1). The tourniquet times of those with late DVT were not significantly different from patients without DVT (P = .899).
The elective procedures performed on these patients are listed in Table 2. Most patients in this study underwent hindfoot surgery, predominantly ankle arthrodesis, midfoot fusions, and calcaneal osteotomies with tendon transfers, all requiring 6 weeks non–weight bearing after surgery.
Procedures Undergone by Patients.
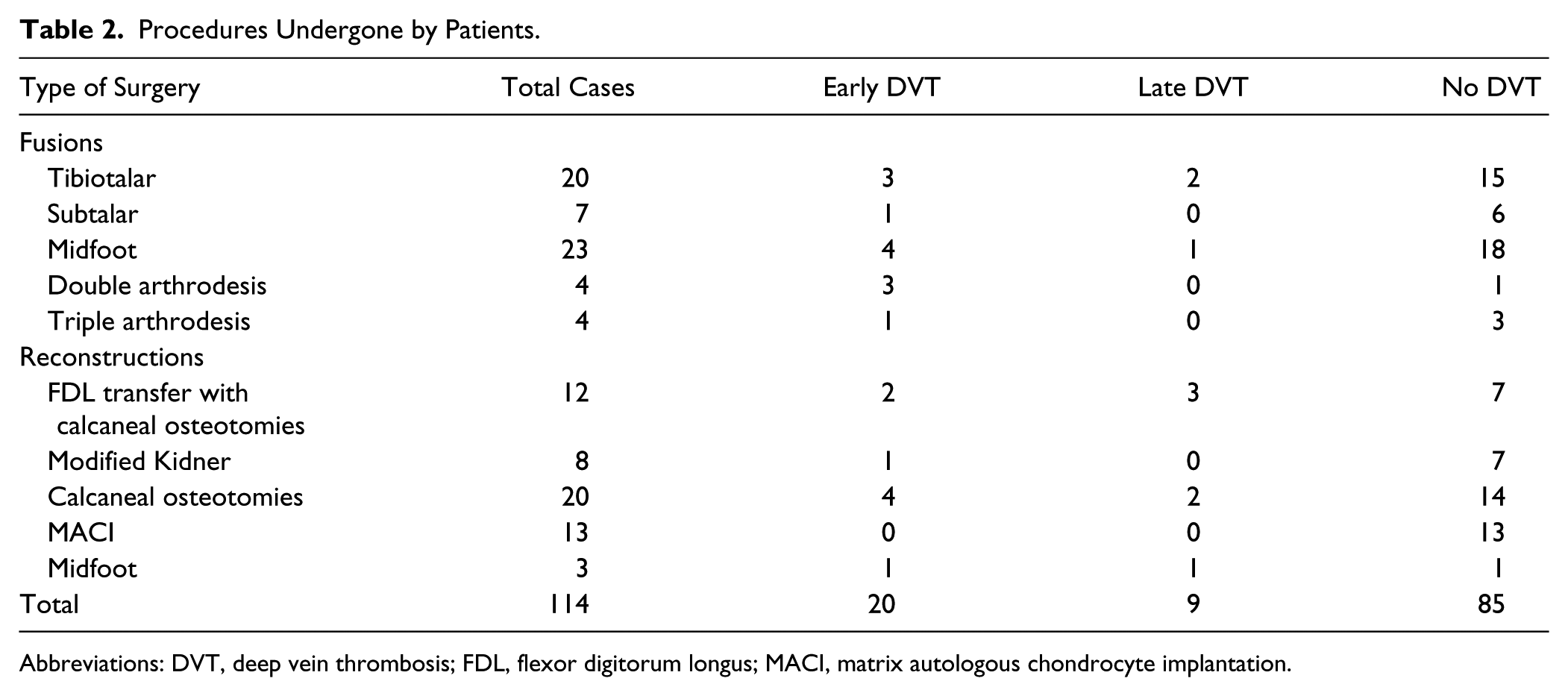
Abbreviations: DVT, deep vein thrombosis; FDL, flexor digitorum longus; MACI, matrix autologous chondrocyte implantation.
Seventy-five percent (15/20) of the procedures diagnosed with thrombosis at 2 weeks postoperatively had no clinical symptoms or signs of DVT. Seventy-eight percent (7/9) of procedures detected with thrombosis at 6 weeks postoperatively lacked symptoms or signs suggestive of a DVT (Table 3).
Symptomatic Patients With Deep Vein Thrombosis (DVT).
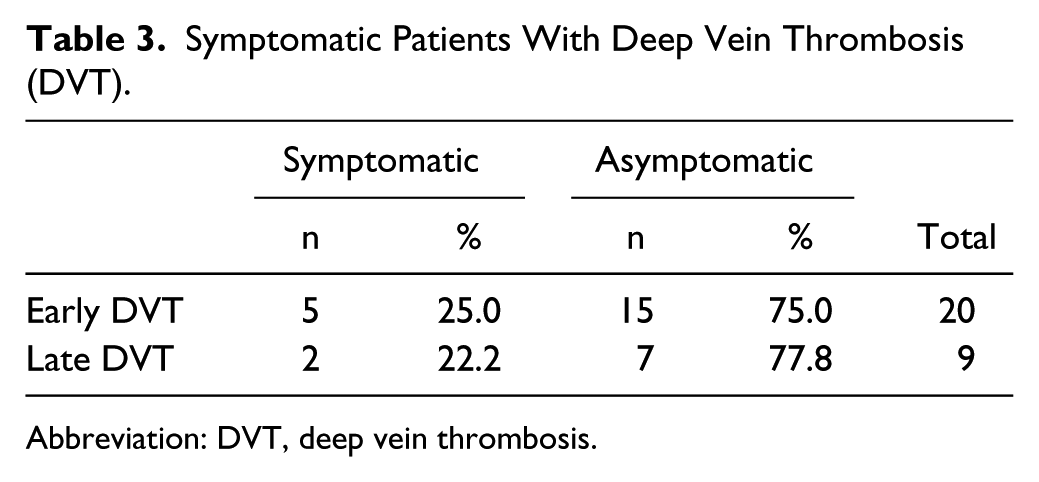
Abbreviation: DVT, deep vein thrombosis.
Discussion
The American Orthopaedic Foot & Ankle Society and the American Academy of Orthopaedic Surgeons have so far found insufficient evidence to formulate practice standards for DVT in the foot and ankle.1,37 Studies have had inconsistent methodology and heterogeneous populations, factors that have been specifically addressed in this study. A meta-analysis by Calder et al found a pooled DVT rate of 12.5% in immobilized patients without any prophylaxis. The included studies except for the one by Solis and Saxby were trauma patients and the majority had not undergone surgery. 3 A 2014 Cochrane review reported incidence rates ranging from 4.3% to 40% for patients with immobilized lower extremities for 1 week. 38 Patients had DVT scans carried out after cast removal. Both studies when compared to our study are misleading as they include predominantly trauma patients who have or have not undergone surgery and the weight bearing status was variable. Trauma patients and Achilles rupture patients were excluded in our study.
We found the overall incidence of DVT after scanning a group of low-risk patients undergoing elective foot and ankle surgery with 6 weeks non–weight bearing postoperatively to be 25.4%. This is a relatively high finding and we can only surmise the possible explanations for this. Our exclusion criteria were more extensive than previous studies reporting on the incidence of DVT. Our study involved 2 ultrasonographic scans spread out over 6 weeks postsurgery. Saragas et al 32 reported an incidence of 8.46% with ultrasonographic surveillance in patients undergoing foot and ankle surgery who were non–weight bearing and were immobilized with a cast for at least 4 weeks postoperatively. They performed a single scan, coinciding with the change or removal of plaster between 2 and 6 weeks postoperatively. Their study included patients undergoing forefoot surgery such as arthrodesis of the first MTP joint or correction of hallux valgus. This did not require cast immobilization or non–weight bearing. The incidence of DVT in this subgroup of patients undergoing forefoot surgery was 0%. After they excluded this subset of patients, the incidence of DVT in the series of patients who were immobilized and non–weight bearing undergoing elective surgery was 8.46%. In all 114 procedures in our study, the patients were non–weight bearing for a period of 6 weeks. In 29% of cases, the patients were non–weight bearing but were actively moving the ankle and foot.
Solis and Saxby prospectively looked at patients undergoing foot and ankle surgery and reported 7/201 patients who had true DVT. This represented 3.5% of the total population. They reported 46.6% of the procedures to be carried out on the forefoot and if you exclude the forefoot patients from the study then the incidence of true DVT is 6.5%. The patients in their study underwent a single ultrasonographic scan at the first postoperative visit around 2 weeks after the surgery. The patients in this group did not undergo further ultrasonography after 2 weeks. In their study, although it is not documented, it is likely that patients did not use knee roller walkers. For patients who were non–weight bearing and immobilized, the use of knee roller walkers has increased significantly since the Solis and Saxby study was published in 2002. The effect of this on venous blood flow may be a factor in the higher prevalence and would certainly need further investigation.
Solis and Saxby also reported hindfoot surgery with or without immobilization to be a factor associated with occlusive DVT. The majority of patients in our study consisted of patients undergoing hindfoot surgery. They did not give any indication of the type of surgery performed in their article; however, they do report that 44% of their patients underwent hindfoot or ankle procedures. In our series, 80% of the patients underwent hindfoot or ankle procedures that may account for the higher incidence of DVT compared to Saragas’s and Solis’s results. Another factor that may have led to our study finding a figure higher than these 2 studies is that the patients in this study underwent vascular testing in a laboratory that performs more than 10 000 vascular scans a year. Solis and Saxby recommended that routine ultrasonographic screening postoperatively was not indicated. They also found that the prevalence of DVT following foot and ankle surgery was higher than previously suggested. In their article, they were unable to give any reasons for this other than that the DVTs were predominantly asymptomatic and the higher prevalence was due to the ultrasonographic screening process.
Our study showed that patients who had normal scans at 2 weeks could then go on and develop a DVT in the period between the 2- and 6-week visits. Of the total number of DVTs diagnosed in the study, 31.1% were diagnosed at the 6-week visit. This indicates that a significant risk of DVT continues after the 2-week visit.
Solis and Saxby found that increased tourniquet time was associated with DVT formation; however, they recorded that tourniquet time was not associated with occlusive DVT formation. In our study, the mean tourniquet time for patients with early DVT at 68 minutes was significantly higher when compared to the tourniquet time for procedures without DVT, which was 58 minutes.
The accuracy of retrospective clinical chart data and diagnosis using physical examination in detecting DVT has previously been questioned as it may lead to under-reporting of DVT.2,11,36 In our study 75% of early and 78% of late DVT were clinically silent. If we had not undertaken surveillance using ultrasonography and had relied on notes or clinical assessment, the prevalence would have been reported as 6% (7/114), comparable with results in the literature.3,38 Ultrasonography is considered the first choice of imaging modalities to identify DVT in clinical practice, with overall sensitivity and specificity of 89% and 94%, respectively. 17
The consequence of clinically silent DVT after foot and ankle surgery remains a topic of debate, however numerous studies have shown that proximal propagation of clots occur in up to 30% of patients.* With propagation, the risk of more serious sequelae such as pulmonary embolism (PE) and post-thrombotic syndrome (PTS) increases.20,23,28 Both PE and PTS have been shown to cause significant morbidity and even mortality.* Subsequent treatment of these complications may be prolonged and costly.5,13,35 The American College of Chest Physicians recommends at least 3 months treatment for confirmed DVT distal to the popliteal vein. 24 There were no cases of pulmonary embolism in this group or in the reports by Solis and Saxby.
Saragas et al reported in their study 2 cases of pulmonary embolism; however, their study had patients including Achilles tendon surgery and trauma surgery. They do not indicate what type of surgery the patients had who developed pulmonary emboli. The risk of propagation increases further as the number of affected veins increases. 24 Lohr et al 20 found that the most proximal levels of propagation were the popliteal vein, superficial femoral vein, and common femoral vein. Proximal propagation carries a 10% to 40% risk of causing potentially fatal pulmonary embolism.3,9,10 The reported prevalence of calf DVT is 7% to 11% in cases with suspected PE. 27 Among those that do not develop fatal embolic events, a proportion may develop chronic thromboembolic pulmonary hypertension, causing persistent increases in pulmonary capillary wedge pressure, even if asymptomatic. 7
Saragas and Ferrao, in a recent article published in 2017 on DVT and foot and ankle surgery, highlighted the concept of venous thromboembolism being a disease with short-term mortality and long-term morbidity. 33 Postthrombotic syndrome is the most common complication of DVT, which develops in 20% to 80% of patients.4,21-25,28-30 Features include chronic pain, swelling, edema, heaviness, skin changes, and venous ulceration in severe cases. 16 Markel 23 found that PTS is generally more severe in patients with distal thrombosis. Symptoms and signs of venous insufficiency may also occur in 37% of patients following DVT. 34 Asymptomatic DVT could therefore cause painful chronic complications that adversely affect outcomes of the surgery performed.
Patients may also be at risk of recurrence of DVT, particularly in the perioperative setting. 19 All patients in this study who developed DVT now become high risk for DVT for any future surgeries. Philbrick et al 28 reported a recurrence rate of 29% for symptomatic patients after short-term intermittent heparinization. Although the mortality risk is low, consideration should be given to the morbidity associated with DVT following foot and ankle surgery.
In our study, all DVT were distal to the knee with no known incidence of proximal propagation. Most of the patients with confirmed DVT were asymptomatic. Therapeutic anticoagulation was given to all patients with DVT confirmed by ultrasonography in this study, which could have prevented any migration or progression of DVT.
In conclusion, overall our study identifies the importance of awareness of DVT. Ultrasonographic surveillance has been shown to detect a higher prevalence of DVT in the past and in this study the prevalence was considerably higher than the 2 previous studies using ultrasonographic surveillance. No definitive explanation can be given for this. Further research is worthwhile, particularly identifying the differences between clinical examination and ultrasonographic surveillance to see if there is a reduced incidence of complications of DVT such as pulmonary embolism or post thrombotic syndrome.
Supplemental Material
FAI_807889_ICMJE – Supplemental material for Prevalence of Deep Vein Thrombosis in Low-Risk Patients After Elective Foot and Ankle Surgery
Supplemental material, FAI_807889_ICMJE for Prevalence of Deep Vein Thrombosis in Low-Risk Patients After Elective Foot and Ankle Surgery by Martin Sullivan, Ilian Dominiq Eusebio, Kristin Haigh, Juan Paulo Panti, Abdullah Omari and Jacqueline Hang in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.