
Abstract
Background:
The structural importance of the spring ligament complex in arch stability has been described. Furthermore, the pathology of this complex is often noted in patients with posterior tibial tendon dysfunction. The purpose of this biomechanical study was to evaluate spring ligament repair alone versus augmentation with the FiberTape device in a cadaveric flatfoot model.
Methods:
Eight paired, below-the-knee, cadaveric specimens underwent flatfoot creation and reconstruction. The experimental group received augmentation with FiberTape (InternalBrace). After potting, specimens were loaded statically to measure talonavicular contact pressures and flatfoot correction. Cyclic loading was performed in a stepwise fashion. Loading was performed at 1 Hz and 100 cycles, at 100-N intervals from 500 to 1800 N, with the Achilles tendon also loaded to simulate weightbearing in the postoperative period.
Results:
Control specimen analysis demonstrated failures of 8 of 8 (100%) spring ligament suture repairs, occurring through suture cut-through (5 specimens), suture fatigue and elongation (2), or knot failure (1). One of 8 (12.5%) FiberTape-augmented repairs failed after cyclic loading. The difference in number of repair failures was statistically significant between the 2 groups (P = .0014). Analysis revealed that at forces of 1600 N (P = .03) and 1700 N (P = .02) there were statistically significant differences between the FiberTape-augmented group and the control group, with a greater collapse in the lateral Meary talo–first metatarsal angle in the controls. There was no significant difference or abnormal increase in contact pressures of the talonavicular joint in both groups.
Conclusion:
FiberTape augmentation of the spring ligament appears biomechanically safe and effective under cyclic loading.
Clinical relevance:
Spring ligament augmentation with this device may be another biomechanically safe and reasonable treatment modality for surgeons during flatfoot reconstruction. It is possible that early protected weightbearing after these procedures may be performed.
Introduction
Surgical reconstruction for flexible acquired flatfoot deformity from posterior tibial tendon dysfunction often includes a medial displacing calcaneal osteotomy (MDCO), flexor digitorum longus (FDL) transfer, and possible calcaneonavicular spring ligament repair when indicated. Incompetency of the spring ligament complex has been well described in the acquired flatfoot deformity. In the setting of posterior tibial tendon dysfunction, the tissue of the spring ligament complex is torn, attenuated, or elongated in more than 87% of patients. 6 Surgical tightening of the ligament through a wedge resection or reefing has been described; however, with an attenuated ligament, these repairs are often tenuous.
The InternalBrace FiberTape ligament augmentation device (Arthrex, Naples, FL) has been reported in a clinical series as an adjunct for spring ligament augmentation for the treatment of flatfoot correction with excellent clinical results at short-term follow-up. 1 Furthermore, this device has been safe and effective when used to augment lateral ligament repairs while allowing for accelerated rehabilitation and recovery. 5 Additionally, it has been studied biomechanically for this indication and has demonstrated improved strength compared with standard ligament repair. 12 While this device has demonstrated excellent clinical results in ligament augmentation, there are no biomechanical studies that evaluate its performance in augmenting spring ligament repairs.
The purpose of this biomechanical study was to evaluate spring ligament repair alone versus augmentation with the InternalBrace FiberTape device in a cadaveric flatfoot model. The objectives of this biomechanical evaluation included assessment of deformity correction, intra-articular contact pressure across the talonavicular joint, and the performance of the device compared with standard reefing under cyclic loading.
Methods
Specimen Selection and Preparation
Eight paired, below-the-knee, cadaveric specimens without preexisting foot deformity were utilized. Exclusion criteria included specimens with preexisting foot or leg deformity, preexisting implants in the foot or leg, and those outside of the designated age range. Specimens were thawed overnight. Preparation began with dissection of the proximal tibia and fibula articulation, which was fixed using solid syndesmotic screw fixation. Next, specimens were potted using PVC piping and an auto body filler material (Bondo, 3M). The Achilles was whipstitched with heavy polyethylene braded suture for mechanical loading. The talonavicular joint was exposed for pressure sensor insertion as described below. For angular measurements, the navicular-cuneiform and cuneiform–first metatarsal joints were dorsally exposed and superiorly oriented K-wires were inserted into the talar neck, navicular, and first metatarsal. A lateral oriented wire was inserted into the calcaneus, and markings were made on the anterior aspect of the exposed tibia. Sixteen surgical flatfoot reconstructions were completed and analyzed, 8 matched pairs in total. There were 5 males and 3 females, average age 54 ± 10 years (range, 37-63), average height 170 ± 12 cm (range, 157-188), average weight 77.3 ± 20.2 kg (range, 57.2-108.9).
Loading Apparatus
A previously described mechanical loading setup by our institution was used.2,3,11 Briefly, the tibia potting was fastened to the vertical actuator of a servohydraulic test frame (FlexTest 40, MTS, Eden Prairie, MN). Tension was applied to the Achilles with a pneumatic cylinder. The plantar surface of the foot rested on a horizontal plate supported by bearings that enabled horizontal translation and rotation. The ground reaction force was measured with a load cell (1010ACK-500-B, eccentric load compensated; Interface, Scottsdale, AZ).
Talonavicular Pressures and Photographs
A flexible, thin pressure sensor (K-scan sensor 4205-300, Tekscan, Boston, MA) was calibrated with static weights, trimmed, and carefully inserted into the talonavicular joint. With the Achilles force held at 350 N, the tibia was pressed down until a ground reaction force of 400 N was reached, simulating standing.4,6 Talonavicular contact pressures were recorded. Then, 2 orthogonal digital photographs of the inserted K-wires and tibia markings were recorded from standardized lateral and anterior positions, for analyzing motions in the sagittal and coronal planes as described below. These pressure measurements and photographs were repeated after creation of the flatfoot model, and after the surgical reconstruction steps below.
Flatfoot Model and Radiographic Measurement
Next, a flatfoot model was achieved as described in the literature through stepwise sectioning of the posterior tibial tendon attachments, the spring ligament, and the plantar capsule. 7 The specimen was placed in a separate apparatus that enabled radiography (mini C-arm) with the tibia under 400 N of static weight (Figure 1). The lateral talo–first metatarsal angle of Meary was measured. Values of greater than 4 degrees plantarflexed were considered acceptable flatfoot specimens.
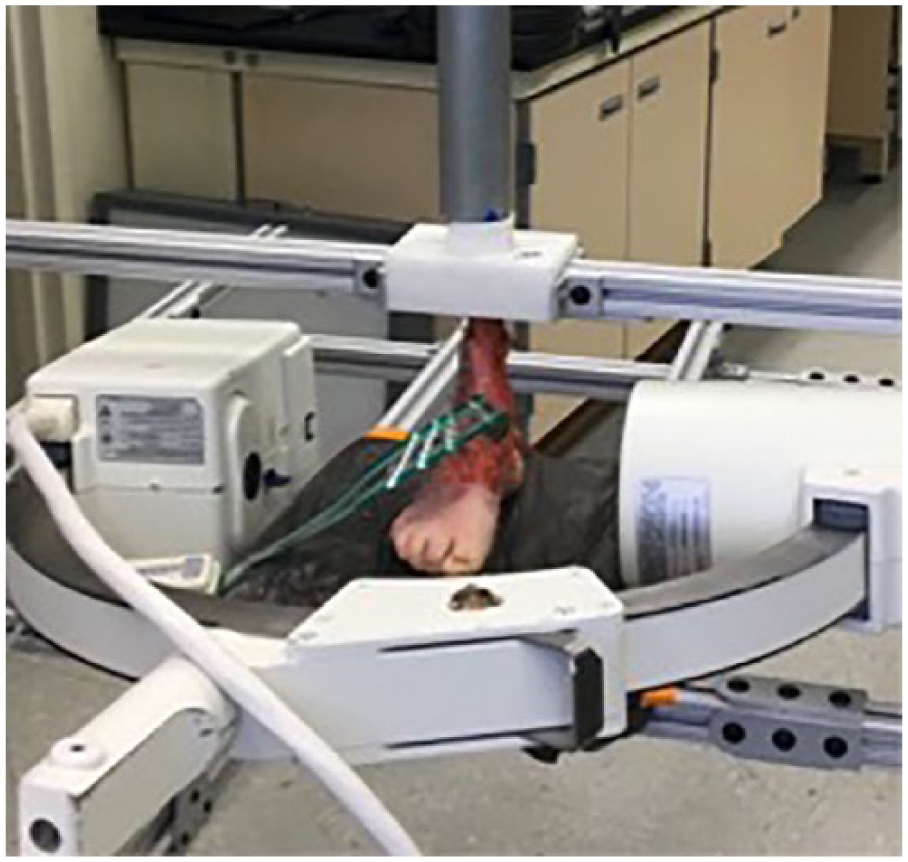
Image of the static loading apparatus performing lateral imaging to confirm flatfoot creation.
Flatfoot Reconstruction Surgery
Next, both groups underwent flatfoot reconstruction via MDCO using a 7.5-mm calcaneal step plate, a spring ligament repair (2-0 fiberwire suture), and an FDL transfer through a navicular bone tunnel with interference fixation via a 4.75 × 15–mm biotenodesis screw (Arthrex, Naples, FL). The experimental group received augmentation with an InternalBrace FiberTape device as described by the manufacturer’s specifications. The sustentaculum tali was dissected and the contents of the tarsal tunnel were protected. A guidewire was then placed in the sustentaculum and overdrilled after ensuring that it did not violate the subtalar joint. It was then tapped by hand and the 3.5-mm BioComposite SwivelLock (Arthrex, Naples, FL) anchor with FiberTape was inserted by hand. After repairing the spring ligament, the FiberTape suture limbs were brought from plantar to dorsal and dorsal to plantar to recreate the “hammock” effect of the spring ligament to protect the repair (Figure 2). The foot was inverted and plantarflexed and the FDL was brought through the bone tunnel and fixed with the 4.75-mm BioComposite SwivelLock anchor. Suture from the FDL whipstitch and the FDL itself was sewn back onto the FDL.
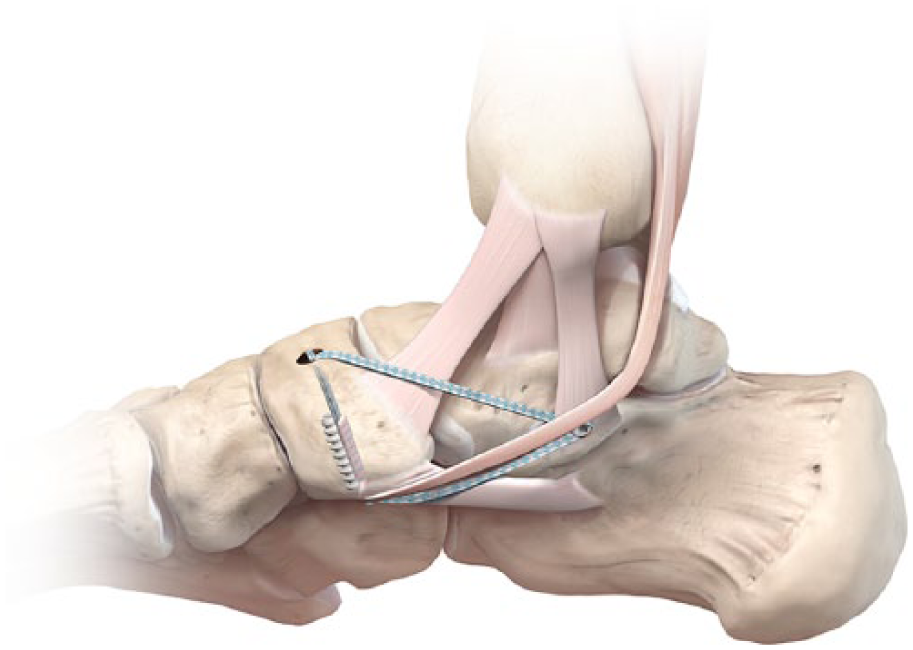
Schematic representation of the spring ligament reefing utilizing the FiberTape device and its hammocklike support. The 3.5-mm SwivelLock anchor is fixed in the sustentaculum and the 4.75-mm anchor is utilized to fix the 2 limbs of suture with the flexor digitorum longus transfer into the navicular bone tunnel. This image provided courtesy of Arthrex, Naples, FL, 2018.
Cyclic Loading
Cyclic loading was performed with stepwise increases in ground reaction force. Loading was performed at 1 Hz and 100 cycles, at 100-N intervals from 500-N to 1800-N peak ground reaction force to simulate weightbearing in the early postoperative period (Supplemental Figure 1). The Achilles tension was held at 350 N. 4 Photographs of K-wire locations were repeated after every 100-cycle interval with simulated standing (400-N ground reaction force) (Figure 3). Specimens were removed from the frame once loading was complete. Reconstruction sites were inspected. Failure of the spring ligament repair was defined by a diastasis at the soft tissue repair site of 2 mm or greater.
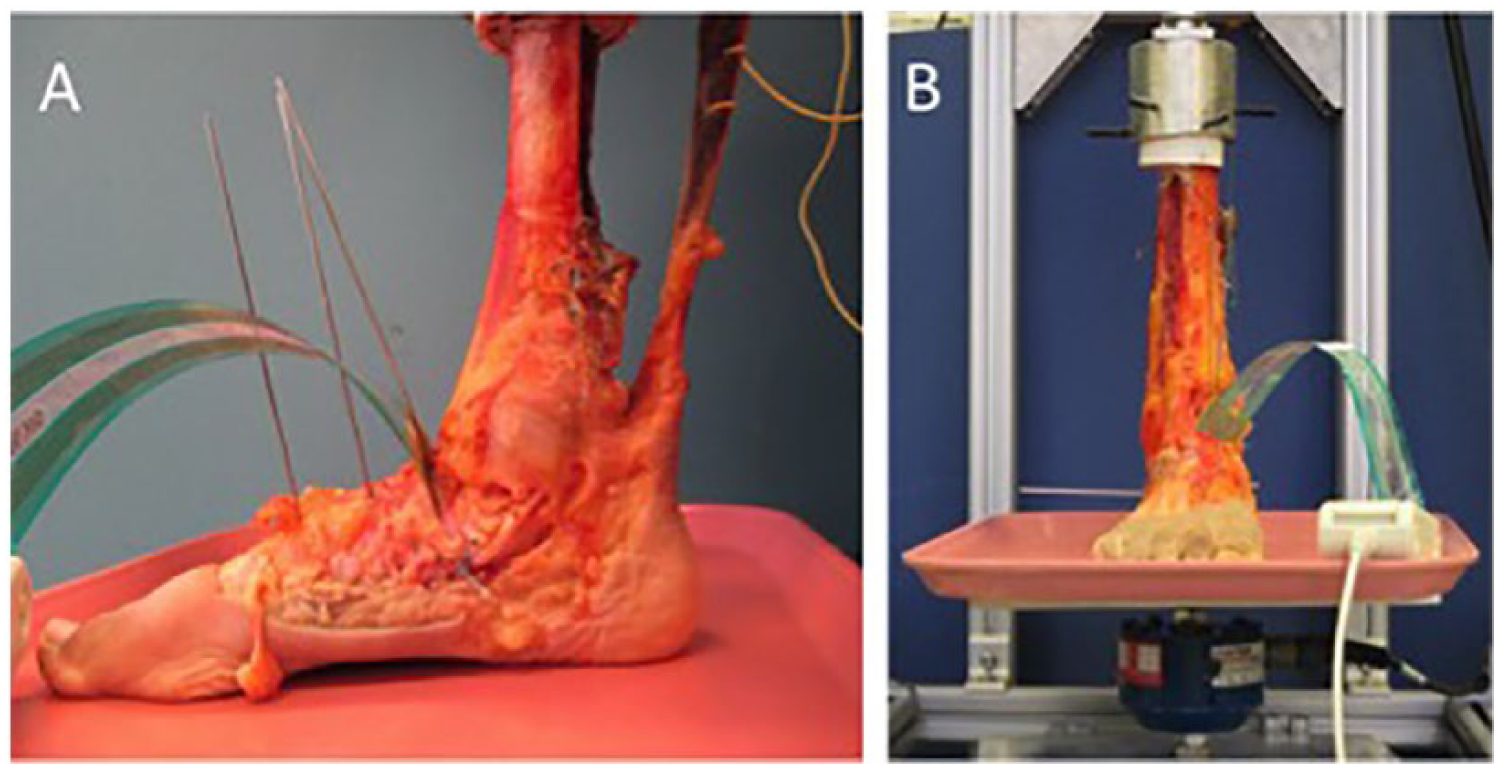
Images of a specimen mounted in a cyclic test machine with K-wires and a talonavicular pressure sensor. (A) Using sagittal plane photographs similar to this one (with the sensor removed), we calculated the change in talometatarsal angle as cyclic loading progressed. (B) Using coronal plane hotographs similar to the one shown, we calculated changes in the talonavicular and tibiocalcaneal angles.
Data Analysis
Talonavicular pressure maps and the Tekscan software were used to determine average and peak pressures. Following the approach by Zanolli et al, changes in 2 angles important in flatfoot deformity were monitored: the talus–first metatarsal angle in the sagittal plane and the talus-navicular angle in the axial plane. 13 Both the Zanolli et al and our study monitored these angles in two-dimensional planes (analogous to radiographic measurements) using pins inserted into the bones. Instead of using electronic clinometers connecting the pins (which has the potential of increased inertial effects), the present study used digital analysis of high-resolution photographs of the pins themselves. Also, in addition to the above 2 angles, this study measured the tibia-calcaneus angle in the coronal plane as an indication of hindfoot valgus.
For analyses of the bone angles between brace and control groups at each force, general linear models with correlated errors were used to account for the matched specimen design and repeated measurements (different force magnitudes) per subject. The presence or absence of spring ligament repair failure after cyclic loading was compared between groups using exact Pearson’s chi-square test. Statistical analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC) by our institution’s biostatistics division.
Results
Spring Ligament Repair and Specimen Analysis
Control specimen analysis after cyclic loading demonstrated failures of 8 of 8 (100%) spring ligament suture repairs (Figure 4B). Most often this occurred through suture cut-through (5 specimens), suture fatigue and elongation (2), or knot failure (1). One of 8 (12.5%) of FiberTape-augmented repairs failed after cyclic loading. The difference in number of repair failures was statistically significant between the 2 groups (P = .0014). The 1 spring ligament failure in the FiberTape cohort occurred via suture cut-through. Additional specimen evaluation demonstrated no biomechanical failures or anchor pullouts of the FiberTape device (Figure 4A). There were no failures of the FDL transfer or the medial calcaneal osteotomy hardware in either group. Dorsal tibiotalar and talonavicular capsular disruption occurred in 2 matched specimens at 1000 N (control), 1500 N (brace), and 1400 N (brace and control).
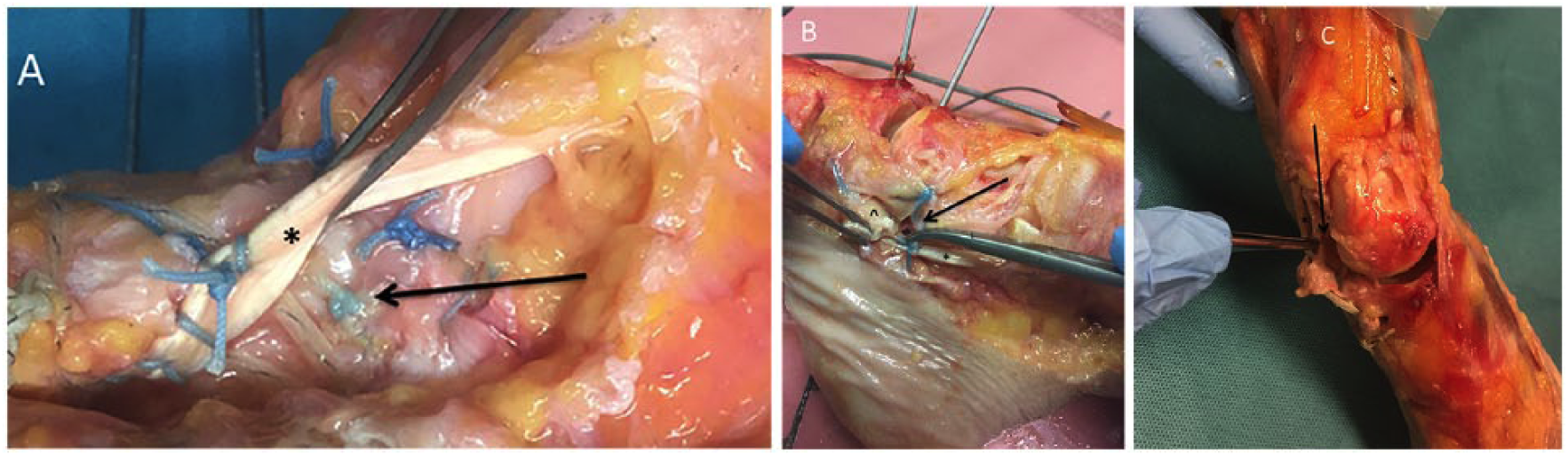
(A) Intact flatfoot and spring ligament repair in a FiberTape specimen after cyclic loading. A bold arrow marks the spring ligament repair site. An asterisk marks the FDL tendon. (B) Control specimen spring ligament repair failure after loading with diastasis of the repair site via suture cut-through. The FDL is marked with an asterisk, the torn spring ligament is marked with a carrot, and the arrow identifies the diastasis of the repair site. (C) Specimen dissection and closer evaluation demonstrates intact spring ligament with augmentation demonstrating the hammock effect of the repair. The FDL is marked with an asterisk, and the spring ligament is identified with a bold arrow.
Cyclic Loading and Digital Bone Angle Analysis
For the majority of forces below 1600 N, there was no statically significant difference detected in the average change in Meary’s talometatarsal angle between groups; however, at forces of 1600 N (P = .03) and 1700 N (P = .02) there were statistically significant differences between the FiberTape-augmented group and the control group, with a greater collapse in the talo–first metatarsal angle at these forces in the control group (Figure 5). There was no significant difference in the talonavicular coverage angle with the FiberTape group compared with controls; angular differences at higher forces neared statistical significance (eg, at 1700 N, P = .07). There were no differences detected in tibiocalcaneal angle changes at any load magnitude between groups (P > .05).
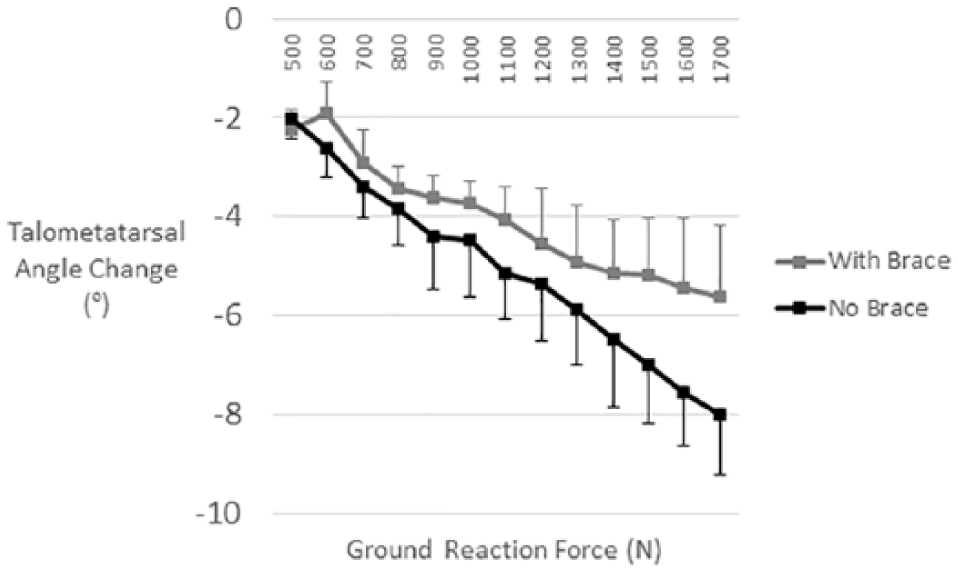
Average changes in talometatarsal angle due to cyclic loading of the feet (n = 5 per group). The 3 pairs of specimens (3 per group) that did not survive loading to 1700 N were excluded to eliminate misleading dropout effects. Zero degrees corresponds to alignment prior to cyclic loading. Error bars indicate 1 SEM.
Talonavicular Contact Pressures
The mean peak talonavicular contact pressures during simulated standing (kPA) of control native cadaver (2596 ± 747 kPA), flatfoot creation (2295 ± 862 kPA), and flatfoot reconstructions (2231 ± 561 kPA) demonstrated no significant differences associated with reconstruction when compared with FiberTape augmentation: native (2232 ± 835 kPA), flatfoot creation (2137 ± 1100 kPA), and after flatfoot reconstruction (2067 ± 1067 kPA) (P = .996). Furthermore, there was no difference detected in the increase in total intra-articular contact force (integrated pressure) associated with flatfoot reconstruction when comparing the FiberTape group (46.9 ± 61.1 N) and controls (59.7 ± 51.4 N) (P = .15) (Figures 6 and 7). After drops in total contact force associated with flatfoot creation, both surgical corrections demonstrated restoration of contact forces to near-intact levels.
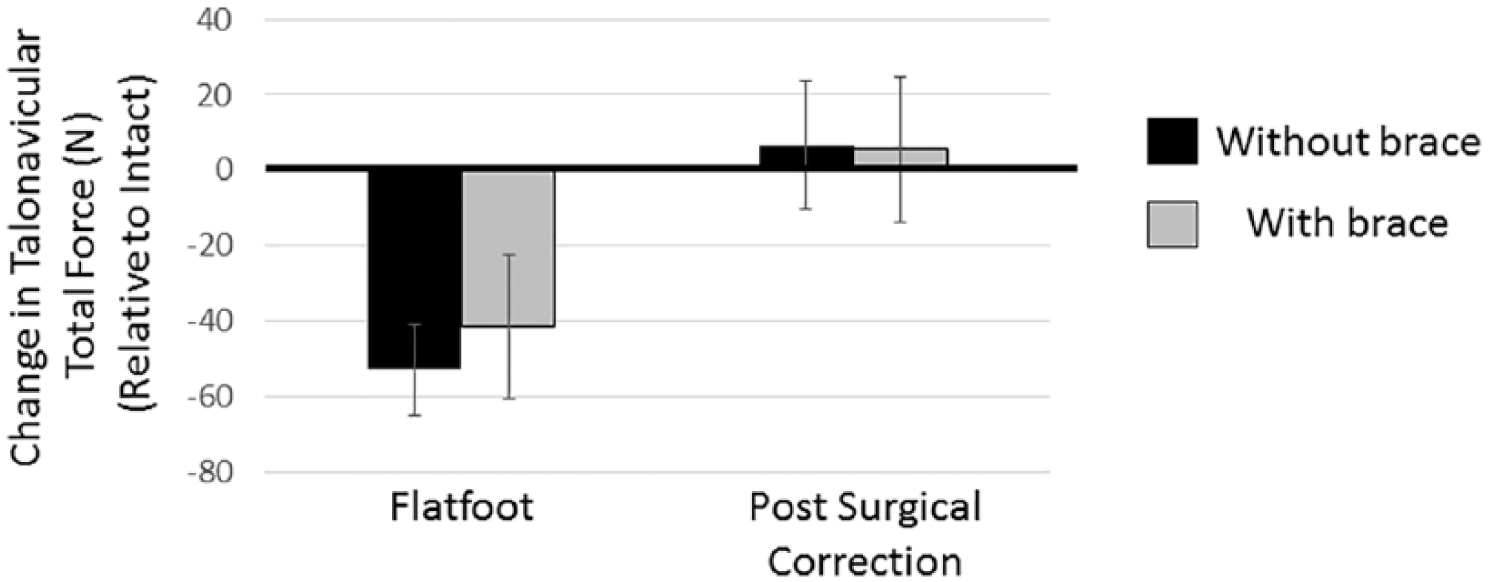
Mean changes in talonavicular total force measured by Tekscan pressure sensors inserted in the joint. Changes were calculated for each specimen relative to its intact, pre-flatfoot creation state (corresponding to 0 in the graph). A statistical difference was not found between the 2 different repair constructs (without and with brace).
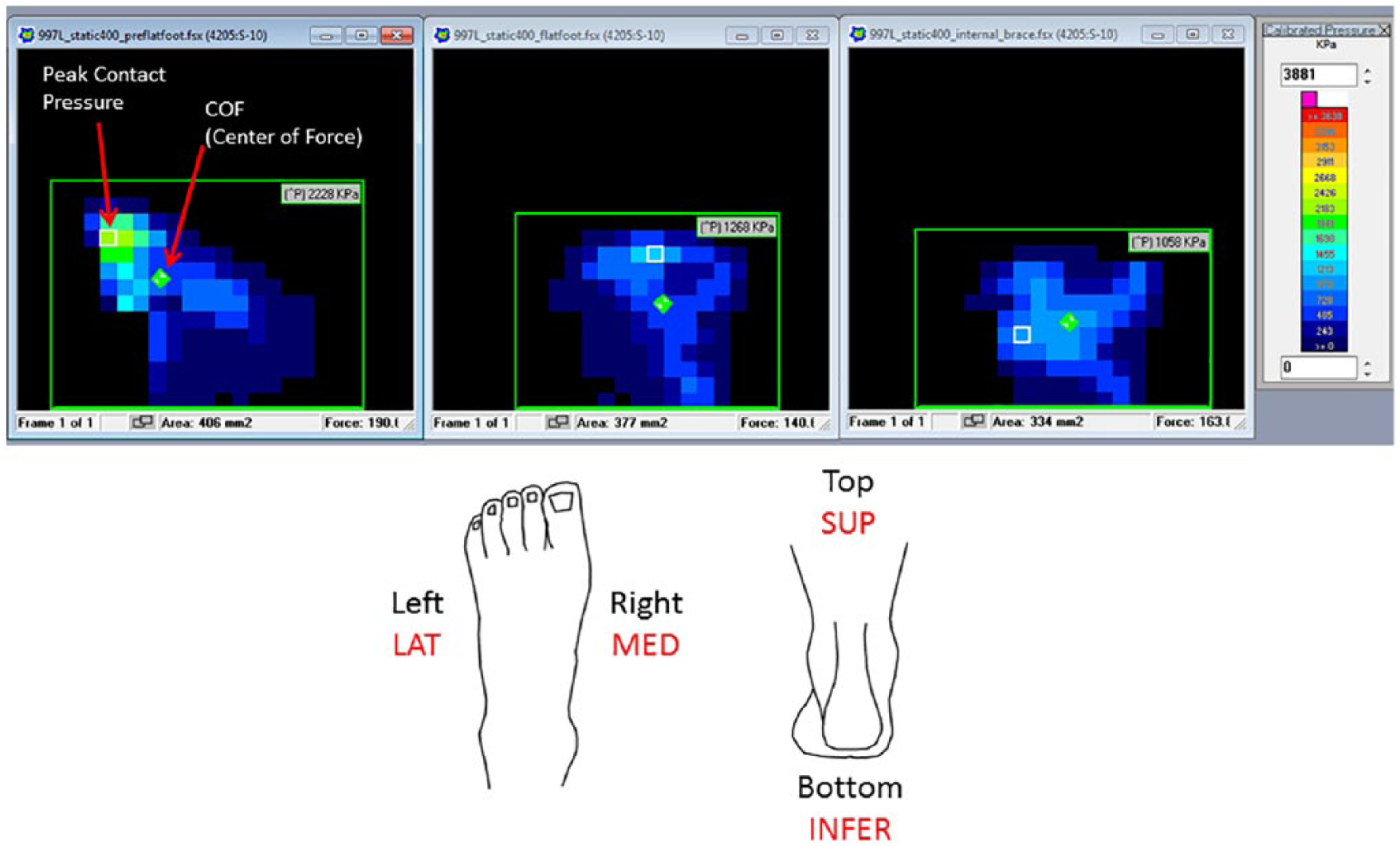
Tekscan pressure measurements of a FiberTape specimen demonstrating peak contact pressures across the talonavicular joint with static loading of the native cadaveric foot measured in kilopascals (far left), talonavicular joint contact pressures after creation of a flatfoot model under static loading (center), and repeated talonavicular contact pressures after flatfoot reconstruction (right). The center of force is labeled in each with a diamond, and the peak contact pressure location with an open box.
Discussion
The purpose of this biomechanical study was to evaluate spring ligament repair alone versus augmentation with the InternalBrace FiberTape device in a cadaveric flatfoot reconstruction model. The results of this study suggest that use of the FiberTape device to augment spring ligament repair may have mechanical benefits under cyclic loading, especially at higher load magnitudes. It remains unclear if the differences between repair methods detected at higher loads are of relevance for the in vivo situation, and thus the clinical relevance of our findings requires further evaluation. At ground reaction force magnitudes of less than 1600 N, there were no significant differences between the reconstructions (although there were apparent trends in the data; Figure 5). Furthermore, augmentation with the FiberTape device did not appear to alter intra-articular talonavicular joint contact pressures. Lastly, the performance of the specimens with FiberTape augmentation suggests that early, postoperative, protected weightbearing may be biomechanically safe after these reconstructions.
The structural importance of the spring ligament complex in arch stability during midstance has been well demonstrated in a biomechanical study by Jennings et al. 8 Furthermore, ligament attenuation, elongation, and even tears are common in the setting of posterior tibial tendon dysfunction. 6 Because isolated spring ligament repairs, or tendon transfers, in the setting of posterior tibial tendon dysfunction often fail, the combination of several corrective maneuvers is an appealing option for surgical correction.9,10 Furthermore, the augmentation of a ligament repair with a FiberTape device has shown excellent biomechanical properties and patient outcomes.5,12 With these results in mind, we sought to evaluate biomechanical performance in augmenting standard spring ligament reefing in a controlled laboratory environment.
Specimen analysis of the controls following cyclic loading to 1800 N demonstrated a 100% failure rate of the spring ligament repair, defined as 2 mm or greater of diastasis. As in most cadaveric studies testing repairs in soft tissues, suture cut-through was the most common mechanism of failure. Conversely, in the FiberTape group there was only 1 failure via suture cut-through. Inspection of this specimen revealed elongation of the FiberTape, intact suture anchors, but diastasis of the underlying repair. In effect, there were no failures of the device itself, nor were there any complications such as inadvertent placement into the subtalar joint or fracture of the sustantaculum tali during insertion. The results observed support the concept that FiberTape augmentation of a ligament repair with this device protects the underlying tissue from the forces applied that may represent early postoperative weightbearing. Another unanticipated observation of this study was the resilience of the FDL reconstruction and osteotomy repair site. In both groups, these repairs maintained their integrity to 1800 N of cyclic loading. The observed data would suggest that early, protected weightbearing with an accelerated rehab might be safe after flatfoot reconstruction.
Cyclic loading of the FiberTape device augmentation compared with controls demonstrated effectiveness at maintaining surgical correction in both groups when analyzing digital imaging in 2 planes, Meary’s talo–first metatarsal lateral angle and talo-navicular coverage. Interestingly, as forces exceeded 1500 N the augmented repair resisted displacement in the sagittal plane compared with controls (P = .03). The most likely explanation is the placement of the device on the tension side of the reconstruction. At higher loads, it appears that the device strengthens the resistance to plantar displacement, augmenting the desired hammock effect of the calcaneonavicular spring ligament.
Any device that crosses a highly mobile joint such as the talonavicular joint can in theory cause abnormal constraint, increasing contact pressure. In this study, there were no differences detected in pressures measured through intra-articular pressure measurements in either group immediately following reconstruction, compared with the pre-flatfoot state and compared with each other. It appears that, first, the standard FDL transfer, MDCO, and spring ligament reefing do not substantially alter the normal pressure forces across the talonavicular joint. Second, the augmentation of the spring ligament with a FiberTape device during flatfoot reconstruction also does not substantially alter contact pressures across this joint.
Limitations of this study include the use of a created flatfoot specimen model and the mechanical loading scheme, which is a simplification of physiologic loading during standing, gait, and other activities. However, the approach of applying cyclic loading of the tibia with the Achilles held at a constant force has been used in recent flatfoot cadaveric studies.7,13 The number of applied cycles at each load magnitude (100) was chosen based on a patient taking a limited number of steps early postoperatively, as well as practical considerations, such as preventing gradual loosening of the tibia-actuator fixation. Another limitation of the study was the direct assessment of the spring ligament repair site via inspection after loading. The precise moment of repair separation could not be determined utilizing the current protocol. Miniature transducers or DVRT placed at the repair site may have been able to record the exact moment and load at the time of diastasis; however, they were not used in this experiment for several reasons. First, these devices measure linear motion, whereas the diastasis occurring during the flatfoot reconstruction and the deformity is three-dimensional, which would lead to inaccuracies. Second, the FDL reconstruction is directly superficial to the deep spring ligament repair, making the application of these measurement tools at the precise location difficult. Last, cyclic loading of these specimens on a freely rotating platform to accurately reproduce the ground reaction force would have made it even more difficult to stay in place during the loading protocol. It is for these reasons that we chose to measure the spring ligament repair site diastasis directly at the time of the final specimen assessment after completion of the loading protocol to determine whether a failure occurred. No statistical correction for multiple comparisons was used. Although none were observed, clinicians should be conscientious to avoid fracture of the sustentaculum tali or aberrant placement into the subtalar joint when inserting this device.
Conclusion
In summary, the results of this study suggest that use of a FiberTape device to augment spring ligament repair in a flatfoot model has some biomechanical advantage under cyclic loading at higher loads. Furthermore, augmentation with the FiberTape device did not appear to substantially alter intra-articular talonavicular joint contact pressures. The InternalBrace FiberTape device may be considered a reasonable surgical adjunct to spring ligament repair when performed in flatfoot reconstruction. Early, postoperative, protected weightbearing with an accelerated rehabilitation protocol may be biomechanically safe after flatfoot reconstruction, although clinical study is needed in this area.
Supplemental Material
DS_10.1177_1071100719828373 – Supplemental material for Biomechanical Evaluation of Spring Ligament Augmentation With the FiberTape Device in a Cadaveric Flatfoot Model
Supplemental material, DS_10.1177_1071100719828373 for Biomechanical Evaluation of Spring Ligament Augmentation With the FiberTape Device in a Cadaveric Flatfoot Model by Michael C. Aynardi, Kaitlin Saloky, Evan P. Roush, Paul Juliano and Gregory S. Lewis in Foot & Ankle International
Supplemental Material
FAI828373-ICMJE – Supplemental material for Biomechanical Evaluation of Spring Ligament Augmentation With the FiberTape Device in a Cadaveric Flatfoot Model
Supplemental material, FAI828373-ICMJE for Biomechanical Evaluation of Spring Ligament Augmentation With the FiberTape Device in a Cadaveric Flatfoot Model by Michael C. Aynardi, Kaitlin Saloky, Evan P. Roush, Paul Juliano and Gregory S. Lewis in Foot & Ankle International
Footnotes
Acknowledgements
We gratefully acknowledge Allen Kunselman, PhD, for providing statistical analysis, Anand Vora, MD, for his help planning the experiment, and Arthrex Inc. for their institutional research grant to support this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael C. Aynardi, MD, reports grants from Arthrex during the conduct of the study and personal fees and other from Arthrex outside the submitted work. Gregory S. Lewis, MS, PhD, reports grants from Arthrex during the conduct of the study. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Arthrex Inc., grant number ST964.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.