
Abstract
Background:
Chronic ankle instability (CAI) is associated with postural control impairment. Orthotic devices are routinely used to improve postural control of CAI patients and prevent recurrence of ankle sprain. This study aimed to evaluate and compare the effect of combined mechanism ankle support (CMAS) with soft ankle support (SAS) and custom-molded foot orthosis (CFO) on static and dynamic postural control in patients with CAI.
Methods:
Twenty-two patients with CAI and 22 matched healthy subjects were recruited. The participants were evaluated in four orthotic conditions (without orthosis and with the CMAS, SAS, and CFO). Static balance was investigated in single-limb stance on the force platform, and dynamic balance was assessed using the Star Excursion Balance Test (SEBT).
Results:
Statistically significant differences were found for the main effects of the groups in all center of pressure (COP) parameters and reach distances in medial (M), anteromedial (AM), and posteromedial (PM) directions of the SEBT (P < .05). The main effect of the orthotics for all evaluated parameters, except reach distance in the PM direction, was statistically different. All COP parameters were significantly lower with the CMAS compared with other orthotic conditions in CAI patients. Also, the higher reach distances with the CMAS were obtained in the AM and M directions of the SEBT.
Conclusion:
The CMAS improved impaired postural control in static and dynamic stability tests, but no similar effect was found for SAS and CFO. This result may have implications for the best bracing for CAI.
Level of Evidence:
Level II, comparative study.
Introduction
Ankle sprain is the most frequent ankle injury that affects both the athletic and general population. 8 A single ankle sprain can cause structural damage to the ligamentous structure of the ankle joint as well as nerves and musculotendinous units. 3 Increasing subtalar joint motion and consequently changing the position of the talus in the talocrural joint has been reported following a lateral ankle sprain. 34 These impairments can increase the risk of reinjury up to 80% and lead the injured subject to chronic ankle instability (CAI). 42 CAI is a complex syndrome with various insufficiencies, such as ligamentous laxity, muscle weakness, proprioceptive deficit, neuromuscular impairment, and frequent episodes of giving way.9,39 Based on these insufficiencies, patients with CAI are classified into different subgroups.21,24 Consideration of these classifications is important for selecting the best treatment approach for patients who suffer from CAI.
Static and dynamic postural control deficits are a common finding in patients with unstable ankle. 1 Due to the importance of postural control in both athletic and recreational activities, various research has been conducted to investigate different treatment strategies for restoring balance and postural control.18,20,30 Orthotic devices are acceptable treatment options to prevent recurrence of ankle sprain and achieve improvement of postural control in CAI patients.17,18,20
Many studies have investigated the effectiveness of ankle supports as well as foot orthoses in CAI patients with postural control deficits.2,15,17,18,20 The mechanism of action of these devices includes maintaining ankle joint alignment in a neutral position, mediolateral (ML) support of the ankle, and reducing ankle or subtalar joint range of motion. Improvement of ankle joint proprioception and reduction of muscular strain around the ankle were also demonstrated.2,11 Ankle supports can improve postural control by applying mechanical and functional effects. ML support of the ankle joint and reducing the linear center of pressure (COP) movement that leads to reduced single-limb postural sway in ankle instability patients are some of the mechanical features of ankle supports. 2 A recent study demonstrated that ankle support can reduce time to inversion and velocity of ankle joint inversion. It suggested that these mechanisms allow the body’s protective system to react and reduce the possibility of ankle sprain. 19
Functional mechanisms of the ankle supports are enhancement of the joint proprioception and musculoskeletal activation. 11 They can be used as a kinesthetic awareness of ankle positioning and control excessive ankle joint motion, especially in inversion. 5 Increasing afferent feedback from the cutaneous receptors around the ankle and skin plantar receptors by these devices are effective in increasing proprioception, which leads to an improved ankle joint position sense. 7
Foot orthoses could provide similar mechanical and functional effects to ankle orthoses. They could position the subtalar joint in a more neutral position, increase contact area on the plantar surface of the foot, and stimulate cutaneous and skin plantar receptors.28,31 It is notable that there are many types of ankle and foot orthoses, and all of these devices could not meet every abovementioned characteristic. Previous studies speculated that the effectiveness of orthotic devices depends on the properties and application method of orthotic devices. These devices have offered different mechanisms of action based on their design and material characteristics.25,26
In a recent study, Hadadi et al introduced a new design of ankle support, the combined mechanism ankle support (CMAS), and claimed that the comprehensive mechanism of this device is sufficient for improving deficits associated with all subgroups of CAI patients. 15 Due to its design, the CMAS was expected to provide various mechanical and functional mechanisms to improve the foot and ankle insufficiency. They demonstrated the beneficial effects of the CMAS on reducing postural sway in patients with CAI. But there is a need to evaluate the CMAS in more challenging dynamic conditions as well as comparison with other ankle and foot orthoses to confirm the efficiency and superiority of this recently designed device.
A superior effect of soft ankle support (SAS) to other types of ankle supports, on static and dynamic postural control, was shown previously.17,18 The SASs are more effective in providing functional support for the foot and ankle. Additionally, the superiority of custom-molded foot orthoses (CFOs) compared with prefabricated foot orthoses on dynamic balance was confirmed in a previous investigation. 33 As an insole, the CFO is more effective in controlling subtalar joint position and plantar receptor stimulation. Therefore, the aim of this study was to evaluate the effect of the CMAS on dynamic postural control, as well as to compare the effect of the CMAS with a CFO and a SAS on static and dynamic postural control in CAI patients.
Methods
Twenty-two patients with CAI and 22 matched healthy subjects participated in this study. The patients were volunteers who came to the rehabilitation center of Shiraz University of Medical Sciences. They had unilateral CAI. The characteristics of these participants are displayed in Table 1. All of the inclusion and exclusion criteria for CAI patients were selected based on the guidelines introduced by the International Ankle Consortium. 12 In this regard, the CAI patients had at least one significant ankle sprain that had occurred 12 months or more prior to the study with a continuing feeling of instability and/or ankle giving way. Also, they reported at least 2 times a feeling of giving way at 6 months prior to participating in the study. The last occurrence of ankle sprain had happened at least 3 months before the study. Mechanical instability (MI) of the ankle was diagnosed by 2 clinical tests, the talar tilt and anterior drawer tests, which were performed by an expert practitioner. Participants were categorized as having functional instability (FI) if they acquired a score of less than 24 from the Cumberland Ankle Instability Tool (CAIT) and less than 90% from the Activities of Daily Living Subscale and less than 80% from the Sport Subscale of the Foot and Ankle Ability Measure (FAAM). The healthy individuals were chosen if they had no history of ankle sprain or sensation of giving way. They also had to acquire a score of higher than 27 from the CAIT and higher than 90% on the Activity of Daily Living Subscale and higher than 80% on the Sport Subscale of the FAAM. The Persian versions of the CAIT and FAAM were used for these assessments.16,29 All of the recruited patients had no history of physical therapy or orthotic treatment.
Participant Demographics.
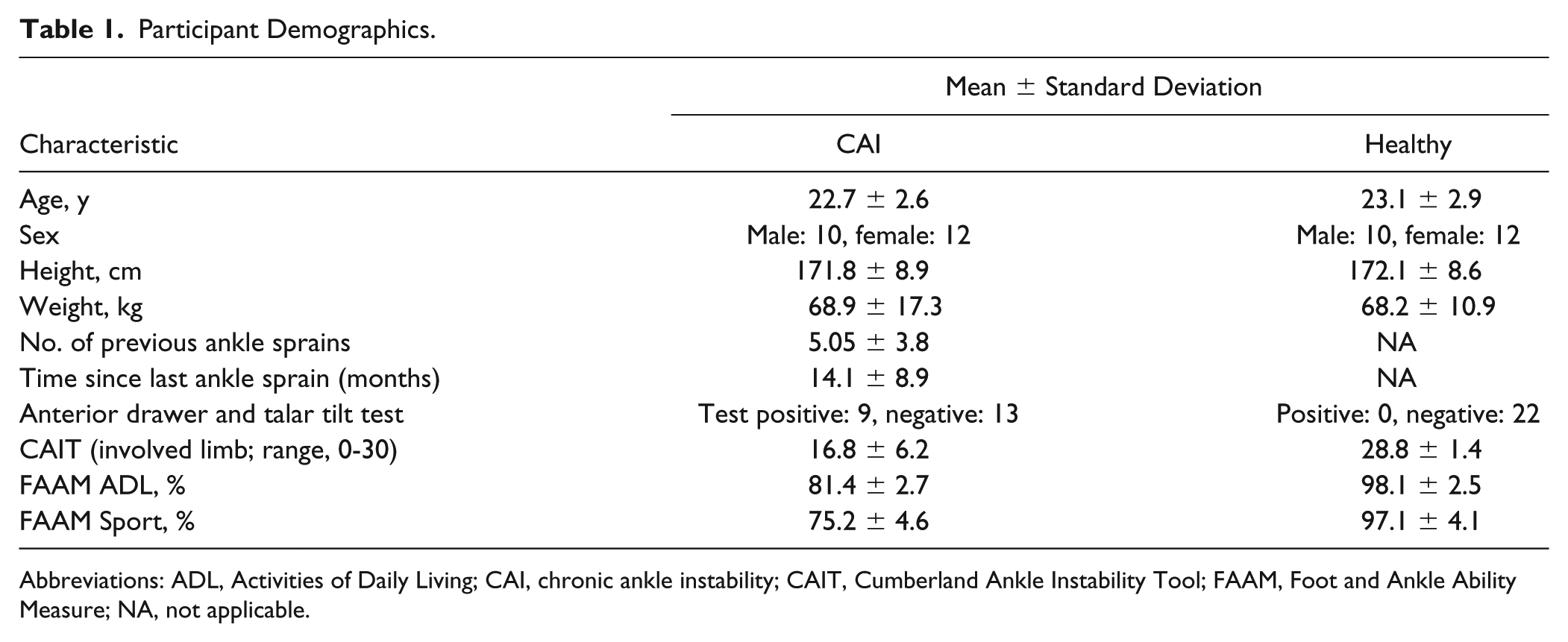
Abbreviations: ADL, Activities of Daily Living; CAI, chronic ankle instability; CAIT, Cumberland Ankle Instability Tool; FAAM, Foot and Ankle Ability Measure; NA, not applicable.
In both groups, the individuals were excluded from the study if they had a history of surgery, fractures or acute injuries of their lower extremity. In addition, patients with uncorrected visual impairment, vestibular or respiratory disorders, and anything that influenced their balance, such as medicine, could not participate in the current study. Participants read and signed an informed consent approved by the ethics committee of Shiraz University of Medical Sciences prior to the study.
In this study 3 kinds of orthoses (CMAS, CFO, and SAS) were tested on static and dynamic postural control of CAI patients (Figure 1). The CMAS was fabricated for each participant based on the method introduced by Hadadi et al. 15 First, an impression of the foot was done in a sitting position while the subtalar joint was aligned in the neutral position, the midtarsal in maximum pronation, and the first ray in neutral. In the next stage, a positive mold of the patient’s ankle and foot was prepared. The CMAS has 3 distinct sections: footplate, medial and lateral supports, and sleeve. The footplate was extended two-thirds along the plantar surface of the foot distally and also was extended to the level of the malleolus and formed a stirrup proximally. Two thermoplastic shells were added medially and laterally to the stirrup and formed the second part of the CMAS. The connection between these 2 sections made a free hinged joint. The third part was a sleeve section that was prepared based on the ankle and foot dimensions and encompassed the whole ankle. A figure-of-eight lift strap secured the orthosis around the ankle.

(A) Combined mechanism ankle support orthosis. (B) Custom-made foot orthosis. (C) Soft ankle support.
The CFO was a custom-made insole. It was made of 3-mm thickness polyethylene that extended to the metatarsal head. It was also trimmed medially and laterally beneath the malleolus to support the medial and lateral longitudinal arches of the foot. In order to achieve better support of the heel section, a 2-cm depth was considered for the heel cup. For fabrication of this insole, an impression of the foot was done in a sitting position while the subtalar joint was aligned in the neutral position.
The SAS was a prefabricated low-profile neoprene ankle support. It encompassed the whole ankle and foot and supported the medial and lateral parts of the ankle. It also had figure-of-eight lift straps that secured it to the ankle.
Participants attended one test session that included assessment of static and dynamic postural control. Static postural control was assessed using the Kistler 9286 BA piezoelectric force platform, Kistler 9865 charge amplifier, and Kistler 5691 A data logger (Kistler, Winterthur, Switzerland). The force-plate measures were selected due to their acceptable sensitivity to discriminate CAI patients from those with stable ankles.27,37 Participants were instructed to adopt a single-leg stance on the force platform with their involved limb (Figure 2). They were asked to look forward and hold their unsupported leg approximately in 30 degrees of hip flexion and 90 degrees of knee flexion. The participants preserved this position for 25 seconds. The trials were discarded and repeated if the unsupported leg touched the weightbearing foot or the force platform. The test was performed randomly in 4 conditions, without orthotic devices and with the CFO, SAS, and CMAS. Three trials were performed in each condition. Rest periods of 30 seconds between trials and 2 minutes between conditions were considered to minimize fatigue effects.
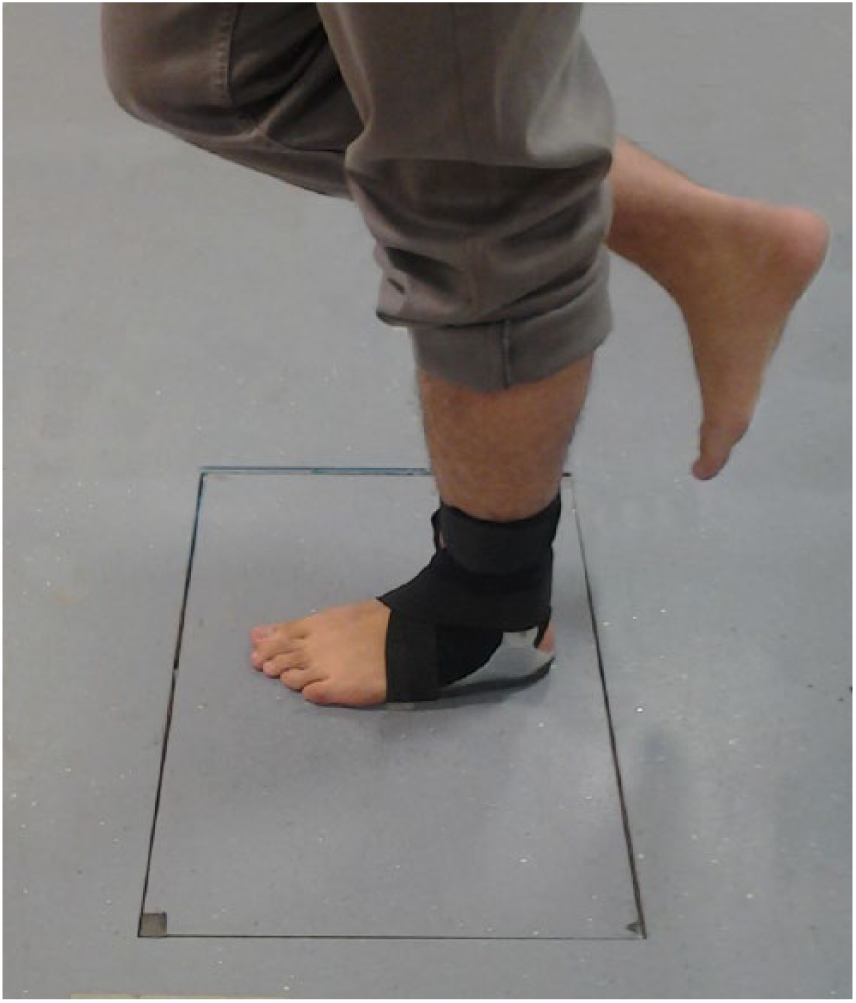
Static test position on force plate with combined mechanism ankle support orthosis.
Because it has been theorized that static single-limb stance tasks may not challenge the postural control system sufficiently, the Star Excursion Balance Test (SEBT) was also used as a dynamic postural assessment in order to better evaluate the mentioned orthotic devices. 38 It has been suggested that the SEBT is an efficient test to distinguish postural control deficits associated with musculoskeletal injuries like CAI. 32 The SEBT was created by 8 directions at 45 degrees to each other from the center of a circle. Participants placed the involved foot of their stance leg in the middle of the testing grid. They were instructed to make a maximum reach with the opposite leg in the anteromedial (AM), medial (M), and posteromedial (PM) directions. 22 They lightly touched the floor with the most distal part of the reaching foot and returned to a double-leg stance position (Figure 3). Successful trials required that hands remained on the hips, that the foot of the stance leg remained in contact with the floor, and avoidance of placing excessive weight on the reaching limb. If these criteria were not met, the trial was repeated. Before the testing procedure, 6 practice trials were performed in each direction to prevent a learning effect. 23 Then 3 successful reaches for each of the 3 directions were performed by the participants. Reach distances were recorded by measuring the distance between the mark point and the center of the test in centimeters with a tape measure.
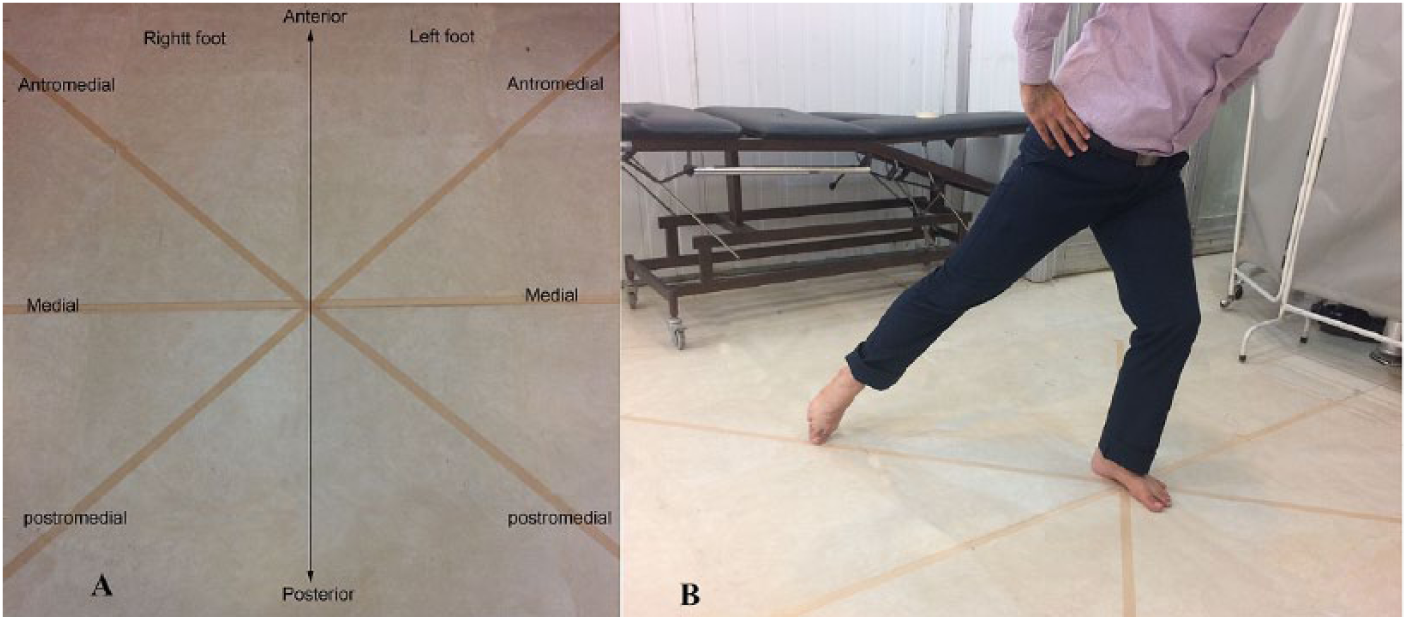
(A) Star Excursion Balance Test directions. (B) Performance of the Star Excursion Balance Test in the posteromedial direction.
Same as the static test, the SEBT was performed randomly in 4 conditions, without orthotic devices, and with the CFO, SAS, and CMAS in the 3 mentioned directions. The SEBT directions were also selected randomly for each participant. The randomization was done by use of random number table. Rest periods of 30 seconds, 2 minutes, and 5 minutes were considered, respectively, between trials, between each direction, and between the orthotic conditions to minimize the effect of fatigue.
The COP data were sampled at 100 Hz. A fourth-order zero-phase Butterworth low-pass filter with a cutoff frequency of 10 Hz was applied to obtained signals. The filtered data were used to compute COP parameters, including mean total velocity, phase plane portrait, the standard deviation of velocity in the anteroposterior and ML directions, and fractal dimension. These parameters were introduced as qualified measures of different aspects of postural behavior with appropriate reliability. The parameters were calculated for each of the recorded trials and the mean of the 3 repetitions in each condition was used for statistical analysis. For dynamic balance data, obtained excursion distances were normalized to the individuals’ leg length. 13 The mean of 3 normalized reach distances in each direction was considered for statistical analysis.
For both static and dynamic tests, 2 × 4 (group × orthotic) mixed-model analysis of variance was considered. These analyses were performed for each parameter of the static test and each direction of the SEBT separately. Bonferroni correction was applied to specify multiple comparisons. All data were analyzed using SPSS version 21 (IBM Statistics, Armonk, NY). In all evaluated conditions the significance level was set at .05. Also, a power analysis was performed. The observed power calculated more than 0.85 and 0.60 based on static and SEBT parameters, respectively.
Results
With the numbers available, no significant difference could be detected in age, height, and weight between the 2 groups (P > .05). The scores of CAIT and both subscales of the FAAM were statistically different (P < .001) between healthy and patient participants. Table 2 demonstrates the mean and SD values of COP parameters and the normalized reach distance for 4 orthotic conditions in CAI and healthy groups.
Mean and Standard Deviation of COP Parameters and Normalized Reach Distance in 4 Orthotic Conditions.
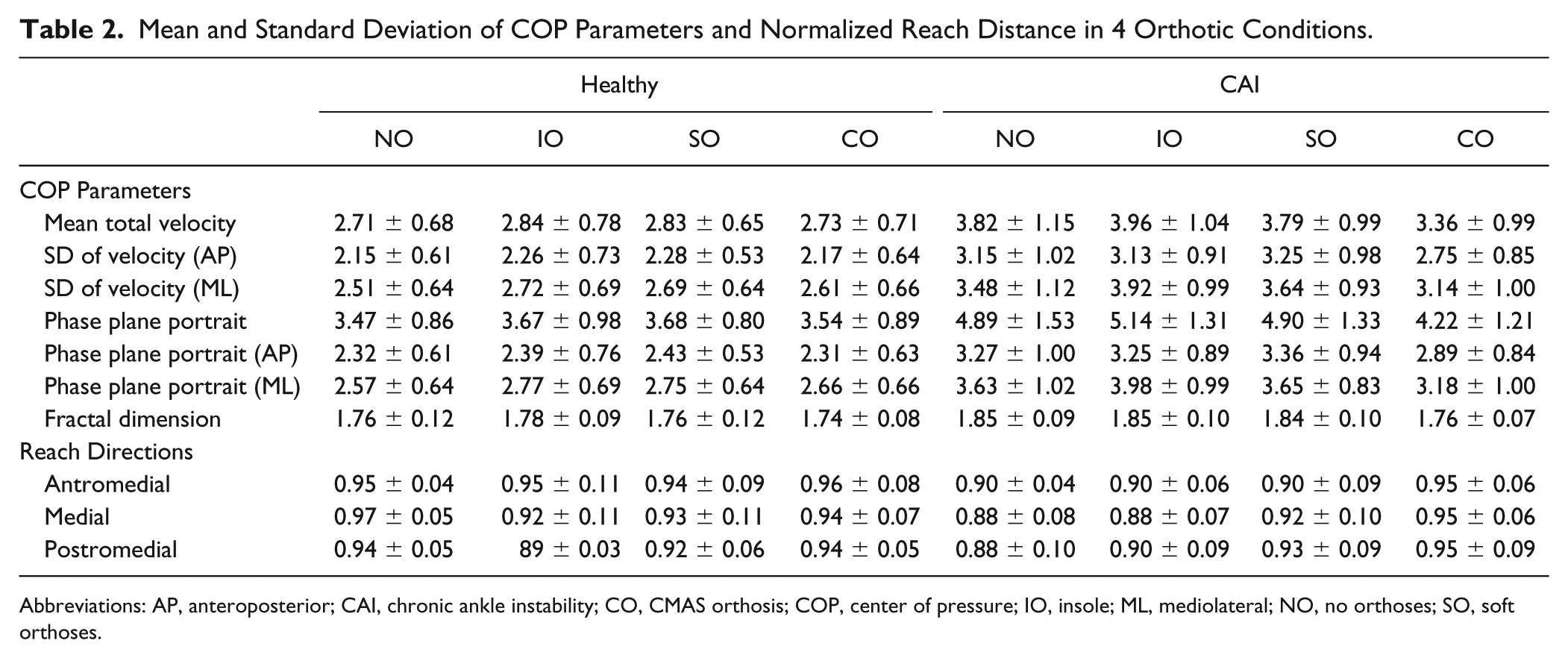
Abbreviations: AP, anteroposterior; CAI, chronic ankle instability; CO, CMAS orthosis; COP, center of pressure; IO, insole; ML, mediolateral; NO, no orthoses; SO, soft orthoses.
In both static and dynamic evaluation, the CAI patients had a different postural control status in comparison with healthy ones. The statistically significant difference was found for the main effect of group in all COP parameters and the reach distance in 3 investigated directions of the SEBT (P < .05). The main effect of the orthotic for all evaluated parameters, except reach distance in the PM direction, was statistically different. Investigation of the effect of orthotics in the healthy group showed no significant difference between various orthotic conditions in both static and dynamic tests. In contrast, post hoc analysis in the CAI group revealed that all COP parameters were significantly lower with the CMAS compared with other orthotic conditions. Also, this group obtained higher reach distance with the CMAS in the AM and M directions of the SEBT. The mean difference and P value of multiple comparisons of the orthotic conditions in the CAI group are displayed in Table 3.
Multiple Comparisons of COP Parameters and Reach Distance of CAI Patient in Various Orthotics Conditions: Mean Difference and P Values by Variable. a
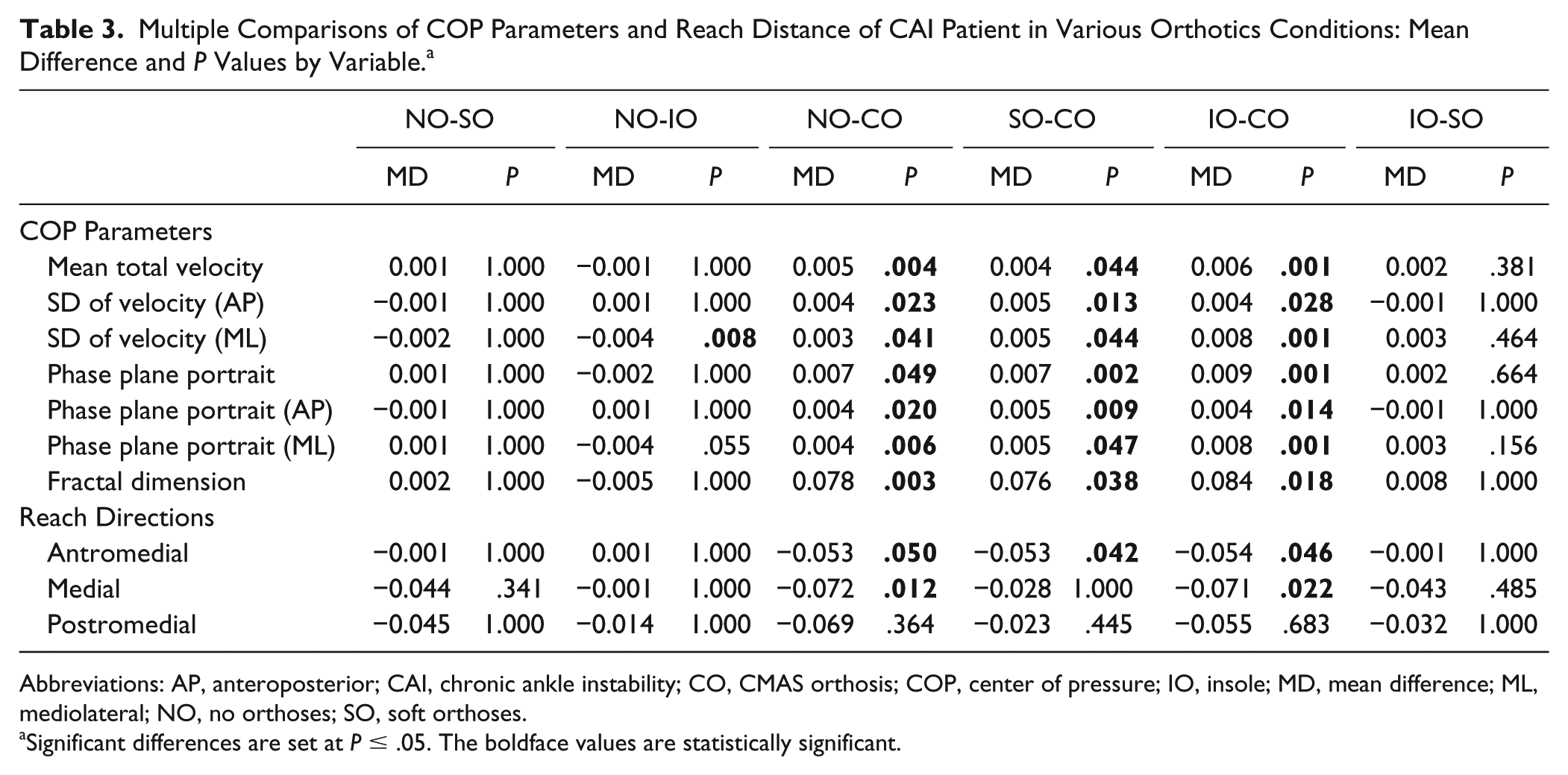
Abbreviations: AP, anteroposterior; CAI, chronic ankle instability; CO, CMAS orthosis; COP, center of pressure; IO, insole; MD, mean difference; ML, mediolateral; NO, no orthoses; SO, soft orthoses.
Significant differences are set at P ≤ .05. The boldface values are statistically significant.
Discussion
The current study, in line with previous ones, showed that patients with CAI have more postural sway in the single-leg stance position and less efficient performance in the SEBT than the control group. Hadadi et al15,17 and Hamlyn et al 20 found greater postural sway parameters in FAI and CAI patients compared with healthy ones. Likewise, Plante et al 35 reported decreased balance during the SEBT performance in CAI patients compared with healthy individuals. Despite diversity in prefabricated foot and ankle orthoses action mechanisms, to the authors’ knowledge, none of them could provide a comprehensive mechanism to meet various needs of CAI patients. Since the therapeutic needs of CAI patients are varied regarding their mechanical and/or functional insufficiency, the recommended orthotic for these patients needs specific customization. The custom-made CMAS is a new introduced orthotic device that could provide such properties. 15
We found that the CMAS improved static postural control in CAI patients but not in the control group. This result is in agreement with the first evaluation of the effect of the CMAS on static postural control in CAI patients. 15 Moreover, in all evaluated COP parameters, the patients with use of the CMAS had lower postural sway rather than those with use of the SAS and CFO. The SAS and CFO had no effect on improvement of postural sway parameters in patients with CAI. In contrast to the current findings, Baier and Hopf found that the ML sway velocity decreased when wearing ankle orthoses in FAI patients. 2 Similarly, Hadadi et al 17 showed not only the improvement of the single-limb stance of FAI patients by using ankle orthoses but also the superiority of SAS compared with semirigid ankle orthoses. Also, Hamlyn et al 20 found that the foot orthosis improved static postural control in patients with FAI. Furthermore, investigation of orthotic devices in more challenging dynamic conditions by the SEBT demonstrated that the CMAS improved patients’ performance in the AM and M directions of this dynamic test but had no effect on the PM direction. Unlike the CMAS, the SAS and CFO did not have a similar effect. There was no difference between patients’ SEBT performance with and without these 2 orthoses.
These findings confirm the results of some previous studies. Gribble et al 14 displayed that prefabricated ankle support did not have any effect on dynamic postural control as measured with the time to stabilization (TTS) test on subjects with CAI. Also, Cattoni 4 found no TTS changes in patients with CAI using the same ankle brace. Although this study introduced similar results, it should be noted that the SEBT and TSS showed different sensitivity in CAI patients. 1 Another study, conducted by Wikstrom et al, 41 revealed that none of the soft and semirigid ankle supports improved dynamic postural control assessed by the dynamic postural stability index in CAI subjects.
In contrast to the current results, Sesma et al 38 demonstrated improvement of dynamic postural control performance after 4 weeks of use of CFO in patients with CAI. This improvement had a more pronounced effect in the M, AM, and PM directions of the SEBT. In the same way, Hadadi and co-workers 18 investigated the effect of soft and semirigid ankle orthoses on the M, AM, and PM directions of the SEBT in patients with FAI. They suggested that ankle supports improved the SEBT performance immediately after the orthotic intervention. They also found the dominant effect of SAS in comparison with a semirigid one. Likewise, Faraji et al 6 demonstrated the immediate beneficial effect of soft and semirigid ankle orthoses on dynamic and semidynamic postural control assessed by the Biodex Balance System in basketball players with CAI. Also, Lee et al 26 found that custom-molded ankle support with hinged joint provides better control on the subtalar and ankle joints of patients with a history of ankle sprain during a lateral cutting maneuver.
The disparity between the current study and the previous studies may be due to the differences in patient groups. The patients evaluated in this study consisted of various subgroups of CAI (MI, FI, etc). The more beneficial effect of the CMAS compared with other ankle supports may be due to its more efficient design. The comprehensive mechanism of the CMAS could restore the subtalar and hindfoot alignment with its foot section, support the ankle complex by means of the ML stirrup section, and stimulate skin and muscle mechanoreceptors with the help of the sleeve part. In regard to the mechanism of action of orthotic devices, Richie 36 revealed that the most viable mechanisms of action of foot orthoses in patients with CAI are improvements in somatosensory feedback and reduced muscular load by influencing multiple levels of neuromuscular control of the ankle. Also, Verhagen and Bay 40 expressed that external ankle supports act primarily by supporting the impaired neuromuscular control in patients suffering from ankle sprain rather than by mechanical support of the ankle joint. A closer look at previous studies revealed that most of the evaluations found positive effectiveness of foot orthosis or ankle supports on CAI patients.2,17,18,20 Additionally, other similar studies did not specify the subgroups of their CAI participants.6,38 Based on these results, it is reasonable that other orthotic devices had a more pronounced effect on functional aspects of postural control insufficiencies. The orthotic device should provide both mechanical and functional benefits to be effective for all subgroups of patients with different insufficiencies. This speculation has been supported by a recently published review that evaluated the effectiveness of foot orthoses on postural control in patients with CAI. 10
This study has some limitations. All of the participants were young, so the generalizability of results to an older population is unknown. Since we evaluated the immediate effect of orthotic devices in CAI patients in the current study, it is necessary to examine the long-term effect of this device in forthcoming studies. Likewise, it is suggested that future studies evaluate the kinematic and kinetic changes resulting from this new ankle support in static and dynamic conditions in patients with CAI.
Conclusion
The orthotics had no effect on the healthy group. The CMAS improved impaired postural control in static and dynamic conditions in patients with CAI, but no similar effect was seen with the SAS and CFO.
Supplemental Material
FAI833993-ICMJE – Supplemental material for Comparison of the Effect of the Combined Mechanism Ankle Support on Static and Dynamic Postural Control of Chronic Ankle Instability Patients
Supplemental material, FAI833993-ICMJE for Comparison of the Effect of the Combined Mechanism Ankle Support on Static and Dynamic Postural Control of Chronic Ankle Instability Patients by Mohammad Hadadi and Faezeh Abbasi in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shiraz University of Medical Sciences, grant number 1396-01-51-14991.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.