
Abstract
Background:
Open metatarsophalangeal (MTP) arthrodesis using locked plates produces good clinical outcomes. However, arthroscopic fusion with new-generation fully threaded compression screws is emerging as an alternative. The purpose of this study was to compare low-profile contoured locked plates with fully threaded compression screws for first MTP fusion, in a biomechanical cadaveric model.
Methods:
The first rays of 8 matched pairs of fresh frozen cadaveric feet underwent dissection and dual-energy x-ray absorptiometry (DEXA) scanning to measure bone mineral density (BMD). The “plate” group was prepared with cup-and-cone reamers, and fixation of the MTP joint with 1 compression screw and low-profile dorsal locked plate. The matched-pair “screws” group was prepared through a simulated arthroscopic technique, achieving fixation with 2 new-generation fully threaded compression screws. The plantar MTP gap was recorded with an extensometer during 250 000 90-N cyclic loads followed by a single load to failure.
Results:
The screw group demonstrated significantly greater stiffness, 31.6 N/mm (plates) and 51.7 N/mm (screws) (P = .0045). There was no significant difference in plantar gapping or load to failure, 198.6 N (plates) and 290.1 N (screws) (P = .2226). Stiffness and load to failure were highly correlated to BMD for the screw group, r =0.79 and r = 0.94, respectively, but less so for the plate group, r = 0.36 and r = 0.62, respectively. The maximum metatarsal head height measured on the lateral view was strongly correlated with load to failure for both the plate- and screw-only groups (r > 0.9).
Conclusion:
These data demonstrate that hallux MTP arthrodesis utilizing fully threaded compression screws had similar plantar gapping and load to failure when compared with the low-profile locking plate, but with significantly more stiffness. These results support an increased role of fully threaded screws for MTP arthrodesis using either the arthroscopic or open technique. However, with decreased BMD plate fixation may remain the better fixation choice.
Clinical Relevance:
Our data suggest that with regard to construct stability, fully threaded headless compression screws may be just as effective as low-profile locking plates, but BMD and MTP joint fluoroscopic measurements should be considered in the decision-making process for fixation.
Introduction
If conservative treatment fails for arthritis of the hallux metatarsophalangeal joint (MTPJ), arthrodesis has proven to be a successful treatment, as both a primary and salvage option.2,18 There are several surgical fixation techniques available to achieve successful MTP arthrodesis, including plates, screws, Kirschner wires (K-wires), memory staples, Steinmann pins, biodegradable rods, and monofilament wires. 22 Success rates have been shown to be between 80% and 100%. 30
Recent plating techniques yielded significant improvements in fixation stability and union rates.3,7-10,13,15,16,21,24,26-28,38,39 While plating techniques are highly successful, they necessitate a relatively large dorsal incision, which can lead to postoperative complications. 1 The plates can also be bulky, creating subsequent symptoms during activities and showing wear over time. In contrast, arthroscopic fusion requires smaller incisions, which may result in less swelling, less pain, and fewer complications. 35 The evolution of minimally invasive techniques and instruments has enabled the arthroscopic preparation of an arthritic hallux MTPJ for arthrodesis.7,25,33,37 Fixation for arthroscopic MTPJ fusion can be achieved by crossing compression lag screws.10,20,24 Compression lag screws were previously compared with standard dorsal plates,4,12,29,34 and standard plates were shown to be mechanically superior. Fully threaded headless screws may provide superior stability when compared with compression lag screws because the threads engage the cortex in 3 places, the outer cortex at the site of insertion and both cortices at the MTPJ. Standard compression lag screw threads, however, do not always engage cortical bone, depending on surgeon technique. Fully threaded screws may provide a more stable construct to allow early weightbearing, particularly if the subchondral plate is preserved. In addition, the headless design may reduce postop complications because there is no screw head to irritate the surrounding soft tissue. 22 However, there have been no biomechanical studies to compare the mechanical stability of the fully threaded screws to current generation locking plates.
The goal of this cadaveric study was to compare the stiffness and load to failure of fully threaded headless compression screws with the current generation of locking plates used with a single compression lag screw. We also sought to examine the relationship between stiffness and load to failure, in the context of bone mineral density (BMD) and bone dimensions of the MTPJ. We hypothesized that there would be no significant difference in plantar gapping during cyclic loading, stiffness, load to failure, or construct failure during cyclic loading between the 2 groups.
Methods
Preparation of Specimens
The study design was based on data from Hunt et al and the power calculations described by Dell et al.11,18 The Hunt study had 3 locked plate specimens fail during cyclic testing. 18 We assumed we would have the same number of failures in both groups. Using their plantar gapping data, we wanted to detect a difference of 1.6 mm and expected a standard deviation of 0.8 mm. Using an α of 0.05 and 1 – β of 0.8, we calculated a need for 4.95 specimens per group. That gave us n = 8 specimens when taking into account 3 specimens failing during cyclic loading.
Eight matched pairs of frozen mid-tibia to toe tip cadaver specimens were obtained from a tissue bank (ScienceCare, Phoenix, AZ). Cadaver research is not considered human subjects research and therefore did not require institutional review board (IRB) approval at our institution. There were 5 male donors (average age 58.6 years, range 45 to 68 years) and 3 female donors (average age 56.0 years, range 48 to 61 years). The specimens were evaluated visually and radiographically for gross deformity, previous operation, or fracture. No specimens were removed from the study based on these criteria. Subsequently, they underwent dissection comprising removal of the medial column including medial cuneiform and the first metatarsal bone with associated proximal and distal phalanges. Tendons, sesamoids, and muscles of the medial column were removed while ligamentous and capsular attachments were preserved. Dual-energy x-ray absorptiometry (DEXA) scanning was performed to measure the BMD of the metatarsals. The entire metatarsal was outlined with the DEXA software to measure the BMD of the entire metatarsal. Fluoroscopic images (superior-inferior; medial-lateral) were obtained for each specimen to make anatomic measurements. All left foot specimens were fixed with locking plates. The matched right foot specimens were fixed with fully threaded headless screws to create a paired analysis.
All specimens in the plate group were prepared by the same foot and ankle fellowship-trained orthopedic surgeon. The plate group was prepared by dissecting MTPJs using a standard arthrodesis procedure with cannulated power cup-and-cone reamers. The dorsal capsule was incised to allow preparation of the joint and plate attachment; however, the lateral, medial, and plantar aspects of the capsule were left in place. A single 1.6 mm K-wire was placed proximally through the center of the head of the metatarsal. A cup-shaped reamer was slid over the K-wire to expose the subchondral bone. The radius of the reamer was sequentially decreased in size until the entire articular surface was removed. The phalanx was reamed in a similar fashion with a cone-shaped reamer. The 2 bony surfaces were temporarily stabilized with crossed 1.6-mm K-wires with the hallux in approximately 20 degrees dorsiflexion and 10 degrees valgus at the MTPJ. A single cross-compression 3.5-mm lag screw was placed from distal-medial to proximal-lateral across the MTPJ in standard lag fashion. Then a low-profile titanium dorsal locking plate (Stryker, Mahwah, NJ) was fixed across the MTPJ with 5 bicortical 3.5-mm locking screws.
All specimens in the screw group were prepared and instrumented by the same foot and ankle fellowship-trained orthopedic surgeon. The screw group was prepared through a simulated arthroscopic technique achieving fixation with 2 fully threaded headless compression screws (Acutrak 2, Acumed, Hilsboro, OR) while preserving capsular attachments. The simulated arthroscopic procedure was performed from the plantar side as the sesamoids had been removed. The subchondral bone was left intact, as was the capsule. Small capsular incisions were made and the joints were prepared with small arthroscopic curettes and small joint osteotomes. One 1.37 mm guidewire was inserted across the MTPJ from the distal-medial cortex of the metatarsal toward the proximal-lateral inner cortex of the phalange. A second 1.37 mm guidewire was placed from the proximal-lateral cortex of the phalanx toward the proximal medial inner cortex of the metatarsal. The standard Acutrak 2 fully threaded headless compression screws with a 4-mm tip and 4.1-mm tail were then placed over the guidewires and inserted across the MTPJ to fix the joint. Figure 1 shows a radiograph of 2 specimens with screw fixation and locking plate, respectively. Fluoroscopic images were saved at the end of the procedure and the specimens wrapped in saline-soaked gauze and placed in a ‒25°C freezer for storage.
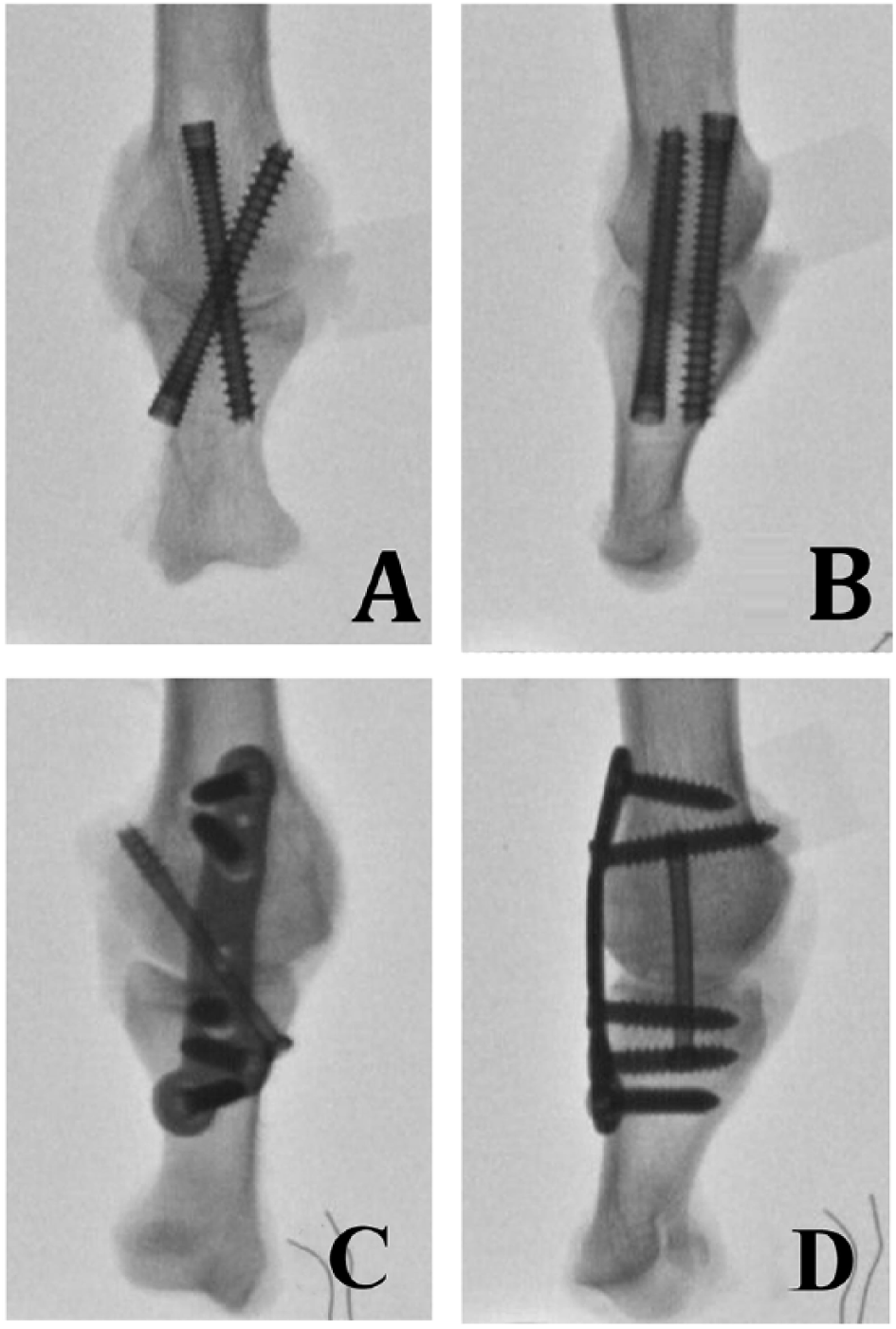
Fluoroscopic images of a matched-pair specimen after they were fixed and before mechanical testing. (A) Anteroposterior (AP) view of the screw group. (B) Lateral view of the screw group. (C) AP view of the plate group. (D) Lateral view of the plate group.
Specimens were thawed for 24 hours at room temperature and prepared for mechanical testing by embedding the proximal end of each specimen, including cuneiform and metatarsal base, in 6.35 cm-diameter aluminum tubing filled with Smooth-Cast 321 (Smooth-On, Inc., Easton, PA). The MTPJ was 30 mm and the edge of the plate was 10 mm from the edge of the potting material. The metatarsal base of the specimen was then mounted on the base of an Instron Model 1321 with 8500 controllers (Instron Corp., Norwood, MA) in 10 degrees of plantarflexion with the plantar surface facing up. The actuator loaded the phalanx from above. An Instron Model 2620-824 extensometer was rigidly held in place across the MTPJ with springs to measure gap formation during loading (Figure 2). Load, displacement, and extensometer data were collected at 100 Hz on a computer connected to an analog-to-digital board and data acquisition software.
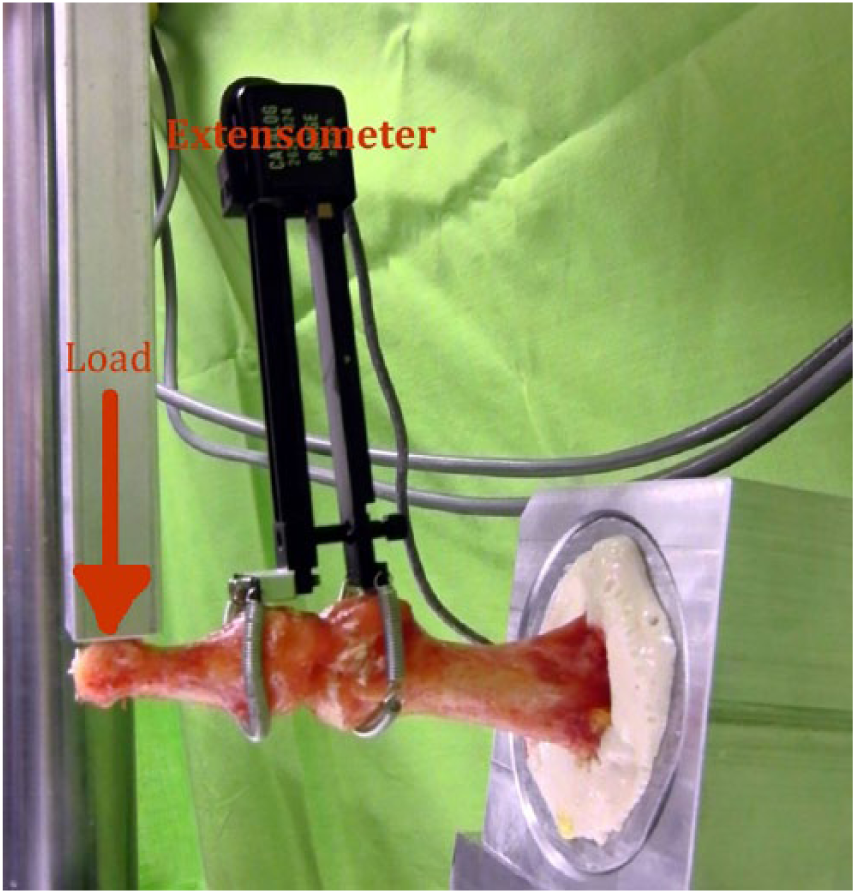
Metatarsophalangeal joint testing setup. The specimen is mounted with the plantar surface facing up and 10 degrees of plantarflexion. The extensometer is rigidly fixed to the bone with knife edge blades and springs. This specimen was fixed with 2 fully threaded headless screws.
Evaluation of Implants for Plantar Gapping, Stiffness, and Load to Failure
To apply the same moment across the MTPJ, the specimens were potted with the MTPJ 30 mm from the edge of the potting and each specimen was loaded on the proximal phalanx at a distance of 65 mm from the edge of the potting material in a cantilever fashion. A 90-N load was applied at 3 Hz for a total of 250 000 cycles. 18 A 90-N load was used to simulate weightbearing in a short leg walking cast and 250 000 cycles was chosen to simulate 6 weeks in the walking cast. 19 The plantar MTP gap was recorded using the calibrated extensometer at 1, 10, 100, 1000, 10 000, 50 000, 100 000, 150 000, 200 000, and 250 000 cycles. Cycling was discontinued if the plantar MTP gap reached 7 mm. Load-to-failure testing was performed on all specimens that endured 250 000 cycles at a rate of 1 mm/s and stiffness was calculated from the final load to failure. The failure load was the maximum load achieved during load-to-failure testing.
Radiographic measurements were made from fluoroscopic images taken after fixation and before mechanical testing with RadiAnt DICOM Viewer 3.0.2 (Medixant, Poznan, Poland). Calibration was made using a metal disc with a 24.18-mm diameter that was in each fluoroscopic image. Measurements taken in both the superior-inferior and lateral orientation included metatarsal mid-shaft, metatarsal head maximum width/height, MTPJ maximum gap, phalanx mid-shaft, and phalanx max width. Measurements taken only in the lateral orientation include the dorsiflexion angle. Measurements were taken independently by 2 authors, each doing 3 separate measurements in all orientations. These measurements were then averaged to give 1 measurement used for correlation analyses.
Statistical Analysis
All statistical analyses were conducted using SAS 9.4. 32 Using the paired t test with Holm-Bonferroni adjustment, analyses were performed to examine the differences in plantar gapping during cyclic loading, stiffness, load to failure, and BMD between the 2 groups. Pearson correlation coefficients were calculated for stiffness and load to failure in relation to BMD. Kaplan-Meier estimates were calculated to determine if the survival estimates of the 2 groups differed. A Cox proportional hazards regression model was fitted to determine if the rate of failure between the 2 groups was different when adjusting for BMD. Nonproportional hazards were tested for all covariates included in the model. Pearson product-moment correlation coefficients (r) between radiographic measurements and stiffness and load to failure were calculated. An absolute r value of greater than 0.7 was considered strong. All P values are reported for 2-sided hypothesis tests; a P value of < .05 was regarded as statistically significant.
Results
Results from the paired t test demonstrate that when comparing the locking plate group to the compression screw group, there was a significant difference in mean stiffness (P = .0045) (Table 1). However, no significant difference was found when examining mean load to failure between the 2 groups (P = .2226) (Table 1). Results from the paired t test also demonstrate that there was no significant difference in plantar gapping between the 2 groups (Table 1). The difference in plantar gapping between the 2 groups is shown in Figure 3. Pearson correlation coefficients are shown in detail in Table 2. It must be noted that the results shown in Table 2 only apply to the specimens that survived the cyclic loading. The locking plate group had n = 5, and the compression screw group had n = 6. Stiffness and load to failure had a statistically significant, strong, positive linear relationship overall (r = 0.82; P = .002). While there was a statistically significant, strong, positive linear relationship between BMD and load to failure overall (r = 0.77; P = .006), this relationship was stronger in the compression screw group (r = 0.938; P = .006).
Results of Paired t Test.
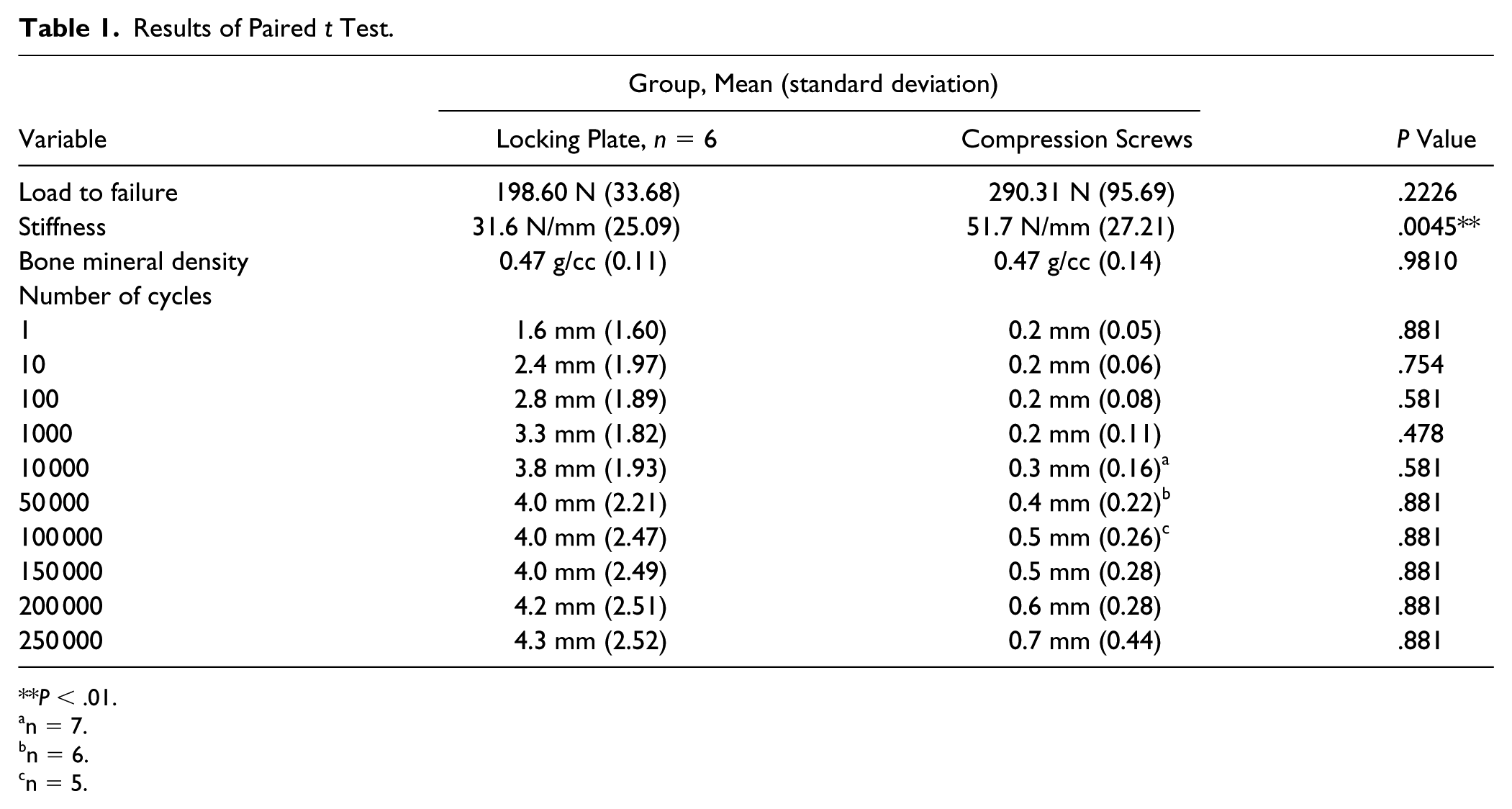
P < .01.
n = 7.
n = 6.
n = 5.
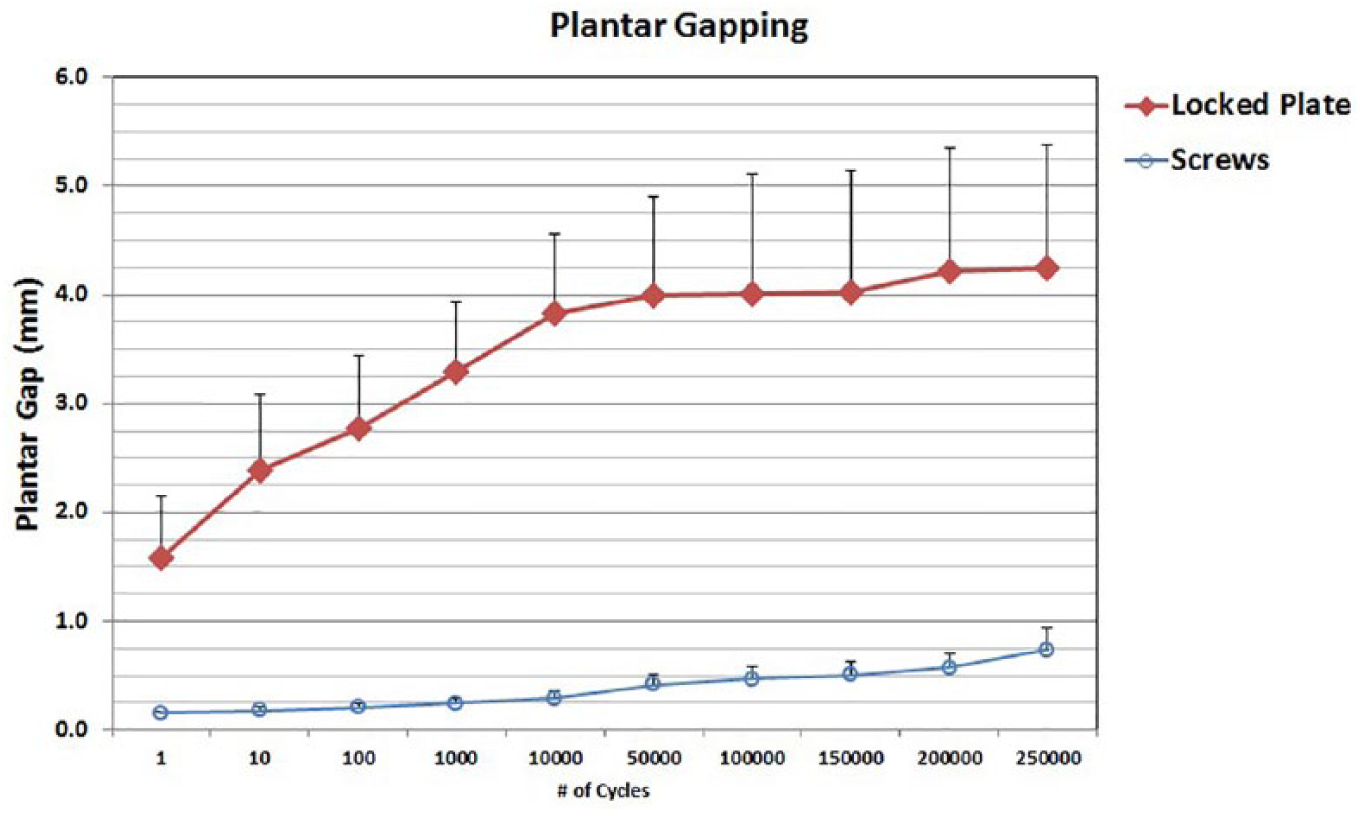
Plantar gapping, plate versus screws. The error bars show 1 standard deviation. The horizontal axis is a logarithmic scale.
Pearson Correlation Coefficients (P value).
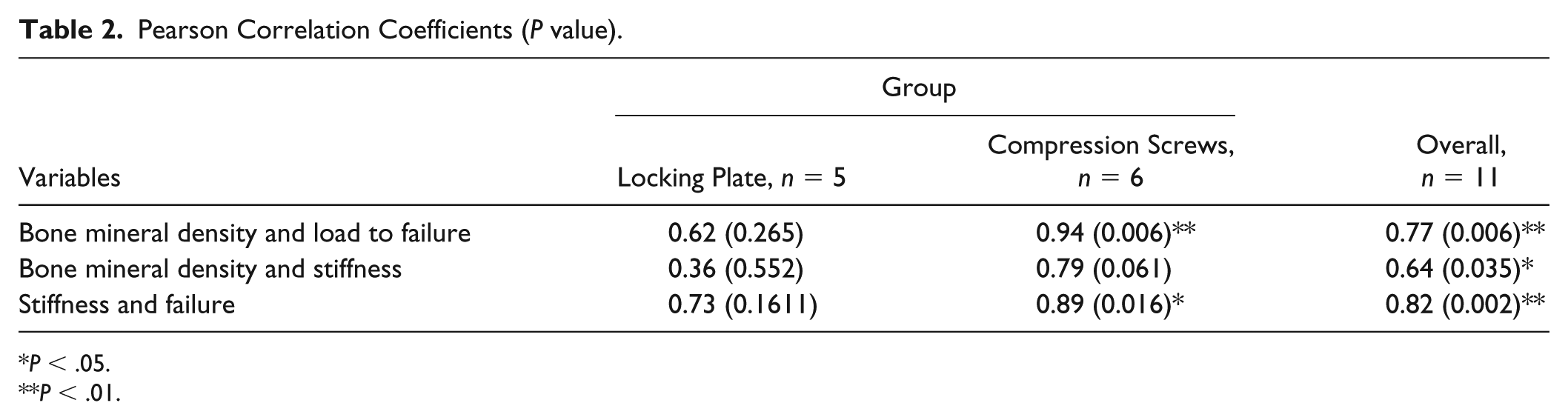
P < .05.
P < .01.
The Kaplan-Meier survival curve is shown in Figure 4. During cyclic loading, 2 of the 8 screw group specimens failed during the initial loading cycle. Three of the 8 locked plate group specimens failed at 6619, 35 385, and 87 408 cycles. The associated log rank statistic illustrates that there was no significant difference in survival time when comparing the plate group to the compression screw group (P = .7229). The results of the Cox proportional hazards regression are shown in detail in Table 3. Results from the Cox proportional hazards regression show that when adjusting for BMD, the group was not significantly associated with the failure (P = .0752). Additionally, BMD did not appear to significantly affect whether or not a group would experience failure (P = .0902).
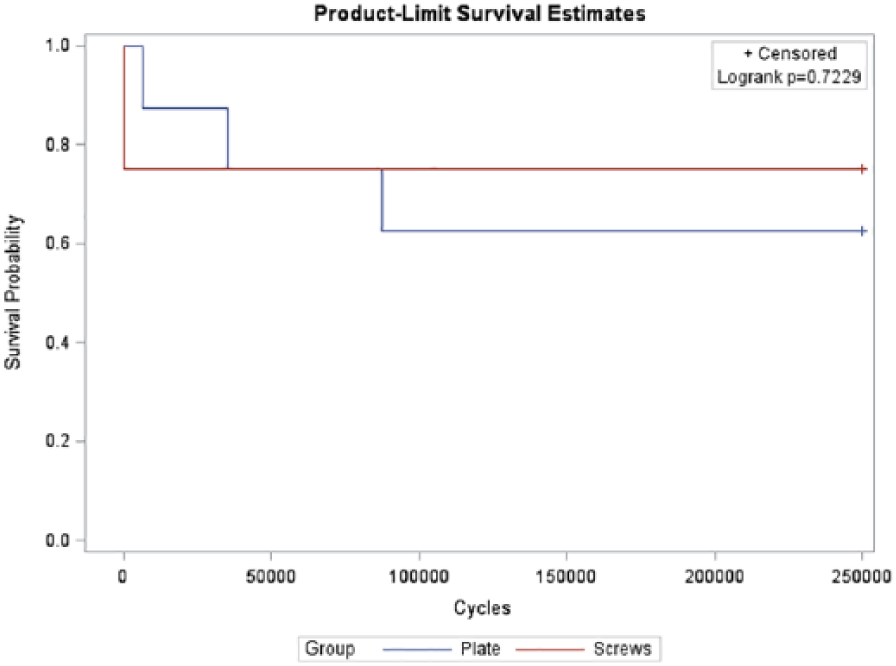
Kaplan-Meier analysis of failure, by group. During cyclic loading, 2 of the 8 screw grew specimens failed during the initial loading cycle, while 3 of the 8 plate group specimens failed at 6619, 35 385, and 87 408 cycles, respectively.
Cox Proportional Hazards Regression Model.
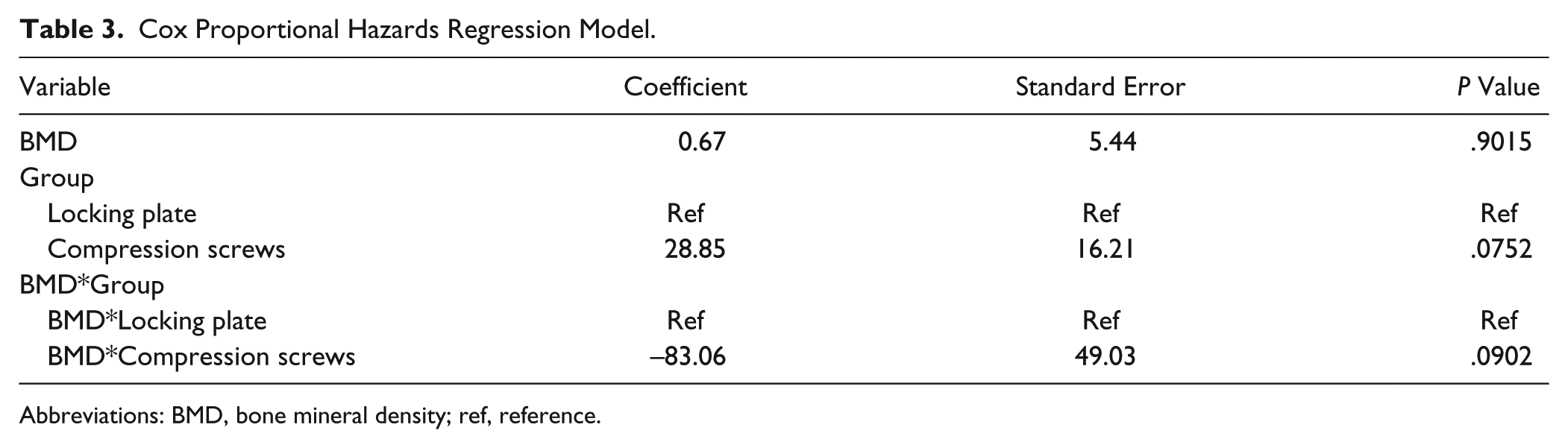
Abbreviations: BMD, bone mineral density; ref, reference.
The radiographic measurement with the strongest correlation to both stiffness and load to failure was metatarsal maximum head height (lateral view). For the screw group, the correlation between failure load and this measurement was 0.96, while the correlation for stiffness and this measurement was 0.865. Similarly, for the plates the correlation between failure load and this measurement was 0.936, while the correlation for stiffness and this measurement was 0.738. The screw group had other strong correlations, including (anteroposterior) phalanx mid-shaft width for both failure load (r = 0.721) and stiffness (r = 0.77). Full results are included in Table 4.
Pearson Product Correlation Coefficients. a
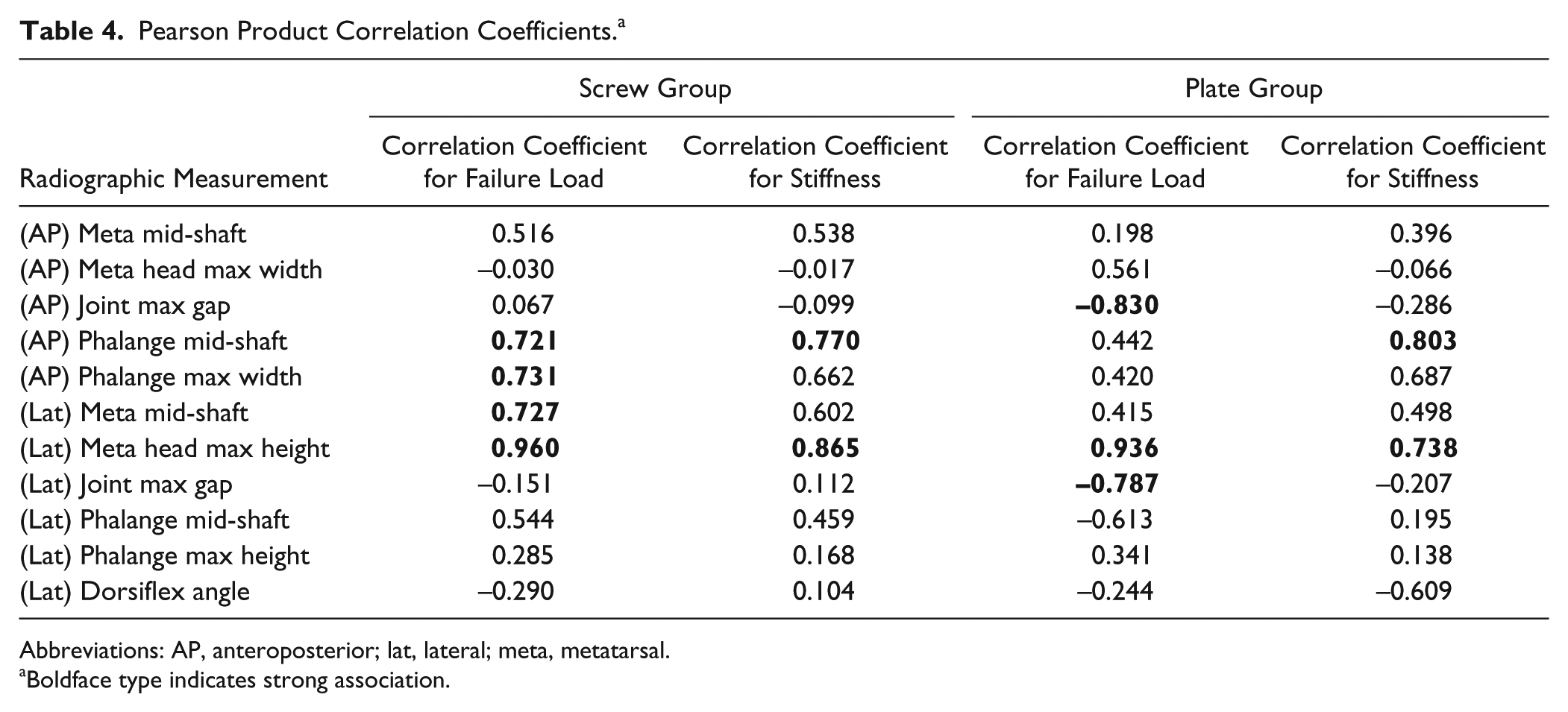
Abbreviations: AP, anteroposterior; lat, lateral; meta, metatarsal.
Boldface type indicates strong association.
Discussion
This cadaveric study compared the mechanical stability of the current generation of locking plates used in conjunction with a single compression lag screw to fully threaded headless compression screws. While locking plates have been highly successful in the treatment of MTPJ arthrodesis, they require a large dorsal incision and can be bulky, potentially resulting in a host of postoperative complications. The benefit of utilizing fully threaded headless compression screws in an arthroscopic technique is that arthroscopic incisions are smaller, and because there is no screw head to irritate the covering soft tissue, there is a decreased risk of experiencing postoperative complications. 31 By investigating the differences in plantar gapping, stiffness, load to failure, the effect of BMD, and construct failure during cyclic loading between the 2 groups, we were able to assess the stability of these 2 constructs. Ultimately, this may help orthopedic providers gain a deeper understanding of the mechanical characteristics of these different fixation techniques. While not germane to the outcome and conclusions of this study, we can anecdotally comment that the cost of the plate and screw construct is quoted as being twice as expensive as the 2 screws used in the study at our institution. However, we expect that prices of these implants will vary by institution.
Contrary to our hypothesis, the results indicated that there was a significant difference between mean stiffness but not in plantar gapping. The results also suggest that there is a strong, positive linear association between stiffness and load to failure, as well as BMD and load to failure. For load to failure and survival time, the results supported our hypothesis, as there was no significant difference between the 2 groups. There is a strong relationship between some of the bone dimensions of the MTPJ and load to failure, which may aid in patient selection and deciding which fixation method to use (Table 4). Specifically, the metatarsal max height (lateral view) had a correlation coefficient >0.9 for failure load in both the plate and screw groups, indicating a possible patient factor that might affect outcome regardless of fixation construct. Additionally, the metatarsal mid-shaft (lateral view), phalanx mid-shaft, and max width (anteroposterior view) all had correlation coefficients for failure load greater than 0.7 for the screw group but less than 0.5 for the plate group, indicating that clinicians can consider using fluoroscopic measurements to help guide fixation construct choice.
There are similar studies in the literature that compare the mechanical stability of dorsal plates to compression screws. Harris et al compared 2 crossed interfragmentary partially threaded lag screws with a dorsal titanium locked plate with a separate interfragmentary lag screw in a single load-to-failure synthetic MTPJ model. 17 Harris et al found the screws to be approximately 50% less stiff when compared with the plate, and they exhibited a similar maximum load. 17 In contrast, the current study found 2 fully threaded screws to be 64% stiffer than the plate, and they had a failure load 46% greater than that of the plate. The improved biomechanical performance of the screws in the current study may be due to the fully threaded design. Specifically, the maintenance of the subchondral bone during preparation improves the fixation strength, and a fully threaded screw will maintain the fixation of the subchondral bone. This may also be due to differences in the size and the materials of the screws used. It must also be noted that the Harris study used a synthetic MTPJ model and only measured a single load to failure, not a 250 000-cycle fatigue test followed by a single load to failure in a cadaver model. Buranosky et al tested a nonlocked plate with an interfragmentary lag screw or 2 crossed cortical screws that were inserted with a lag technique in a cadaver model. 5 They found that the plate and lag screw were significantly stiffer and had a higher ultimate load than the 2 crossed screws. However, this study found the opposite, as the fully threaded screws were stiffer and had a higher load to failure. Again, this difference may be due to a variety of factors, such as the fully threaded screw design that was not inserted with a lag technique, screw size, screw material, or the 250 000 cycles of loading prior to stiffness and failure loading.
There are several techniques that can be used to fix the first MTPJ. Campbell et al showed in a cadaver model that a dorsal plate and lag screw had greater failure load than 2 lag screws. 6 Buranosky et al also showed in a cadaver model that a dorsal plate and lag screw had greater failure load than 2 crossed lag screws. 5 Despite dorsal plates with a lag screw having superior failure loads, they are not without their surgical complications. In a retrospective study of patients that underwent MTPJ arthrodesis, Rashid et al showed that in patients treated with a plate and lag screw, the complication rate was 26% (6 of 23 patients), and in patients treated with a lag screw or plate alone, the complication rate was 20% (3 of 15 patients). 30 A systematic review of patients that underwent first MTPJ arthrodesis showed a similar complication rate of 23.1% (171 of 741 patients), with the most common complications being nonunion or delayed union and implant removal. 36 The introduction of fully threaded headless lag screws may offer an improved alternative to plate and lag screw arthrodesis. This study showed the mechanical advantage of using the fully threaded compression screws. In addition, the headless screws would not leave a metal screw head protruding above the cortical bone that could cause surgical complications with the surrounding soft tissue.
One of the goals of MTPJ arthrodesis is to return the patient to their full normal routine. An additional goal is to return to the patient to their full function as quickly as possible. To be able to accomplish this, the patient must be allowed full weightbearing on the MTPJ. Ledoux et al found that during normal gait the percent body weight subhallucal was 19.5% in the neutrally aligned foot and 25.0% in the pes planus foot. 23 The average weight of the donors in the current study was 175.5 pounds. To allow full weightbearing during normal gait in the pes planus foot, the MTPJ arthrodesis hardware would have to support 196 N. This value could be higher for other activities, such as stair climbing, getting out of a chair, or running. In the current study the failure loads were 198 and 290 N for the locking plate and compression screws, respectively. Therefore, full, unprotected weightbearing is not recommended until the arthrodesis has time to heal. Our postoperative protocol for both techniques includes weightbearing to tolerance in a rocker-sole short CAM walker boot until radiographic healing.
There were limitations to the study. It was a cadaver study that simulated 6 weeks of walking in a short leg walking cast but did not simulate the effect that healing of the MTPJ would have on the mechanical tests. The loading was done in cantilever bending to simulate the ground reaction force, but the in vivo loads are more complex when muscle forces across the MTPJ and inversion/eversion are considered. Additionally, the average age of the specimens in this study was 57.6 years, which may be older than the population that typically has an MTPJ arthrodesis. However, BMD was measured and correlated to both stiffness and load to failure to account for the bone quality of the specimens. Furthermore, while there are several techniques to perform MTPJ arthrodesis, only 2 were tested in this study. The locking plate with a compression lag screw was used because it has been shown to be mechanically superior to a nonlocking plate. 18 The fully threaded headless crossing screws were used because they represent a new application of an existing design that may improve stability over the partially threaded compression lag screw while potentially decreasing the surgical complications of a dorsal plate. Testing only 2 different constructs allowed us to test matched pairs that reduced confounding factors between matched pairs. However, the fixation method was not randomized by side because only left dorsal locking plates were available. The current study did not use stiffness or load-to-failure data from the Hunt study for the power analysis to calculate the number of specimens to test. Using these data instead of just the plantar gapping data may have resulted in a different number of specimens tested. The Hunt study used 9 specimens per group and had 3 locked plates and 4 nonlocked plates fail during cyclic loading, leaving 5 and 6 for stiffness and load-to-failure testing, respectively. They found a significant difference in stiffness but not load to failure, as did the current study.
Additionally, it should be noted that this study was funded by Acumed, which is listed in our disclosures. However, our main objective was to compare the mechanics of fully threaded compression screws to low-profile locking plates. One author receives consulting income from Acumed, which is entirely separate from this study. This author was involved for his expertise in joint preparation and instrumentation but was not in any way involved with mechanical testing, data acquisition, or data analyses.
Conclusion
Our data indicate that hallux MTP arthrodesis utilizing fully threaded compression screws had higher mean stiffness and similar load to failure and plantar gapping compared with a low-profile locking plate. Therefore, preparation in an arthroscopic fashion and fixation using 2 full-thread screws should be at least mechanically equal to a dorsal plate and a cross screw. Surgeons should be aware that there is a difference between using a full-thread screw and subchondral fixation versus using a partial thread screw and compression. 14 Our technique with fully threaded screws ensured engagement of both subchondral cortices, not one.
These results support an increased role of fully threaded screws that would be used in an arthroscopic procedure in lieu of more invasive open preparation and fixation techniques in certain patients. However, failure of the screw-only cohort occurred in specimens with the lowest BMD, potentially indicating a clinical contraindication with this technique in patients with poor bone quality. This therefore assists in the decision-making process for fixation. Poor BMD may predict early failure; therefore, in elderly patients with low bone strength or known osteoporosis a plate technique may be preferable. Likewise, if the surgeon elects to perform an arthroscopic procedure and finds that the bone density is poor, the addition of a dorsal compression plate should be considered. In addition, BMD may aid in predicting early failure and more conservative postoperative protocols might be used to improve results for these patients.
Supplemental Material
FAI837524-ICMJE – Supplemental material for Biomechanical Comparison of Low-Profile Contoured Locking Plate With Single Compression Screw to Fully Threaded Compression Screws for First MTP Fusion
Supplemental material, FAI837524-ICMJE for Biomechanical Comparison of Low-Profile Contoured Locking Plate With Single Compression Screw to Fully Threaded Compression Screws for First MTP Fusion by Richard S. Fuld, Pam Kumparatana, Judas Kelley, Nicholas Anderson, Todd Baldini, Alastair S. E. Younger and Kenneth J. Hunt in Foot & Ankle International
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Richard S. Fuld III, BA, reports grants from Acumed, during the conduct of the study. Todd Baldini, MSc, reports grants and nonfinancial support from Acumed, during the conduct of the study; grants and nonfinancial support from Stryker Endoscopy, outside the submitted work. Alastair S. E. Younger, MD, MSc, reports personal fees from Acumed, grants from Acumed, outside the submitted work. Kenneth J. Hunt, MD, reports grants from Acumed, during the conduct of the study. ICMJE forms for all authors are available online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Acumed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.