
Abstract
Background:
The relationship between juvenile hallux valgus (JHV) and flatfoot has not been clearly established. The aim of this study was to assess radiographic measurements in feet with JHV compared with matched controls and to investigate whether the foot alignment of JHV is related to flatfoot.
Methods:
We retrospectively reviewed 163 patients with JHV as defined as hallux valgus angle greater than 20 degrees and intermetatarsal greater than angle than 10 degrees. Patients with open physes of the feet and who had weight-bearing radiographs of the feet were included. Another 55 normal participants served as controls. Patients with JHV were divided into 2 subgroups: Group 1 included patients with asymptomatic JHV and group 2 consisted of those treated with correctional surgery for painful JHV. Twelve radiographic indices were analyzed, including calcaneal pitch angle, tibiocalcaneal angle, talocalcaneal angle, naviculocuboid overlap, talonavicular coverage angle, lateral talo–first metatarsal angle, anteroposterior talo–first metatarsal angle, metatarsus adductus angle, hallux valgus angle, intermetatarsal angle, distal metatarsal articular angle, and first metatarsal cuneiform angle. The groups were compared by age, gender, and the above radiographic parameters.
Results:
There was no significant difference in hindfoot alignment of patients with JHV and controls. Naviculocuboid overlap (P <.001), lateral talo–first metatarsal angle (P = .002), and metatarsus adductus angle (P = .004) were significantly greater in patients with JHV than in controls, whereas the anteroposterior talo–first metatarsal angle (P = .026) was significantly less. Symptomatic and asymptomatic JHV patient subsets showed no significant radiologic differences.
Conclusion:
Radiographic profiles in patients with JHV were inconsistent with regard to features of flatfoot, and foot alignment was unrelated to the presence of symptoms or degree of deformity in JHV.
Level of Evidence:
Level III, retrospective comparative series.
Introduction
Juvenile hallux valgus (JHV) is often linked with flatfoot, the latter having been implicated in both development and postoperative recurrence of JHV. 23 By measuring various radiographic angles, some authors have shown that the incidence of flatfoot in adolescents with bunions is 8- to 24-fold greater. 16 Some literature has refuted such findings. In one study, the incidence of flatfoot in patients with JHV was comparable to that of the population at large, 3 and other researchers have claimed that arch height is irrelevant with respect to JHV. 17 No correlation between flatfoot and the success of corrective surgery has emerged from several investigations.1,3,17 Although recent literature has shown no consistent association between hallux valgus and foot posture such as the arch index,14,21,22 those studies were conducted in adult populations. The relation between JHV and flatfoot is still a controversial matter.
In most instances, patients with JHV complain of the aesthetics, rather than citing pain or tenderness, although pain may be the chief issue in some. Operative correction is generally compelled by the intensity of pain experienced and not the degree of deformity. In fact, there is considerable discordance between symptom severity and degree of deformity in those presenting with JHV. 2 Although the longitudinal arch of foot may have a bearing on the degree of hallux valgus, we have found no studies as of this writing addressing correlations between the magnitude of symptoms or deformity and the degree of flatfoot manifested by patients with JHV.
Therefore, the purpose of this study was to assess radiographic measurements in feet with JHV compared with matched controls and to investigate whether the foot alignment of JHV was related to flatfoot. We also examined whether the foot alignment of JHV affected the presence or absence of symptoms or severity of hallux valgus by comparing asymptomatic and symptomatic patients. The hypotheses were that the radiologic parameters in feet with JHV would be representative of a flatfoot and the low longitudinal arch or hindfoot valgus would be related to JHV.
Methods
This retrospective study was approved by our hospital’s institutional review board. All records of patients visiting our orthopedic clinic between March 2006 and December 2016 were subject to review, identifying those presenting with JHV. Our inclusion criteria were as follows: patients with idiopathic hallux valgus defined as a hallux valgus angle greater than 20 degrees and an intermetatarsal angle greater than 10 degrees,2,3,16 patients with bilateral standing weight-bearing radiographs of the feet, and patients with open physes of the feet. Any comorbidity impacting foot appearance, such as congenital anomalies, neuromuscular diseases, accessory navicular bones, or hallux valgus interphalangeal deformities led to exclusion.
Once these records were attained and filtered, a total of 163 patients qualified for this study. Parameters compiled for this study included age, gender, laterality, underlying disease, presence/absence of pain, and treatment method. The average age was 11.8 (range 8-14) years. There were 29 boys and 134 girls, most (120/163, 73.6%) displaying bilateral JHV. Of the 33 patients who underwent operative treatment, 16 patients underwent bilateral surgery. To avoid selection bias, right feet only were assessed if both feet were involved or treated operatively. The cohort (163 feet) was then grouped by treatment rendered for JHV: group 1, untreated/asymptomatic (n=130); group 2, operatively treated/symptomatic (n=33). Most patients with JHV were asymptomatic during activity, with no complaints of medial great toe tenderness. These patients and their parents had aesthetic concerns, so no intervention was needed. 2 However, symptomatic patients were those presenting with pain that made walking or sports difficult or with medial great toe tenderness. Such patients had been treated conservatively (ie, shoe and activity modification) for at least 6 months, reserving operative remedies for those failing to show improvement. The primary indication for operative intervention was the presence of pain, as opposed to degree of deformity or cosmetic concern. Corrective osteotomy of the first metatarsal bone and distal soft tissue procedure were performed by one of the authors.
The control group (n=55) was identified by searching for patients with fractures, sprains, polydactyly, or coalition who had been treated in our institution, and selected on the basis of radiograph availability (bilateral weight-bearing views of the foot). Opposing uninvolved feet were examined for our purposes, none afflicted with JHV.
Radiologic assessments were performed by 2 orthopedic fellows who were blinded to study details. All measurements were made independently, twice for each radiograph, with at least 6 months between assessments. The radiographs from initial patient visits were used for measurements.
Eight radiographic indices were measured on initial standing anteroposterior (AP) and lateral radiographs (Figure 1): calcaneal pitch angle, tibiocalcaneal angle, talocalcaneal angle, naviculocuboid overlap, talonavicular coverage angle, lateral talo–first metatarsal angle, and AP talo–first metatarsal angle. These indices show exceptional reliability and high discriminant validity,7,19,26 each reflecting alignment at specific points in the foot7,19 as follows: (1) hindfoot: calcaneal pitch, tibiocalcaneal, and talocalcaneal angles; (2) midfoot: naviculocuboid overlap and talonavicular coverage angle; and (3) forefoot: lateral and AP talo–first metatarsal angles. Additionally, the metatarsus adductus angle was obtained to accurately characterize forefoot alignment, applying the modified Sgarlato method,9,10,13 because the deformity of the first metatarsal in instances of hallux valgus may affect forefoot alignment assessments based on AP talo–first metatarsal angle.
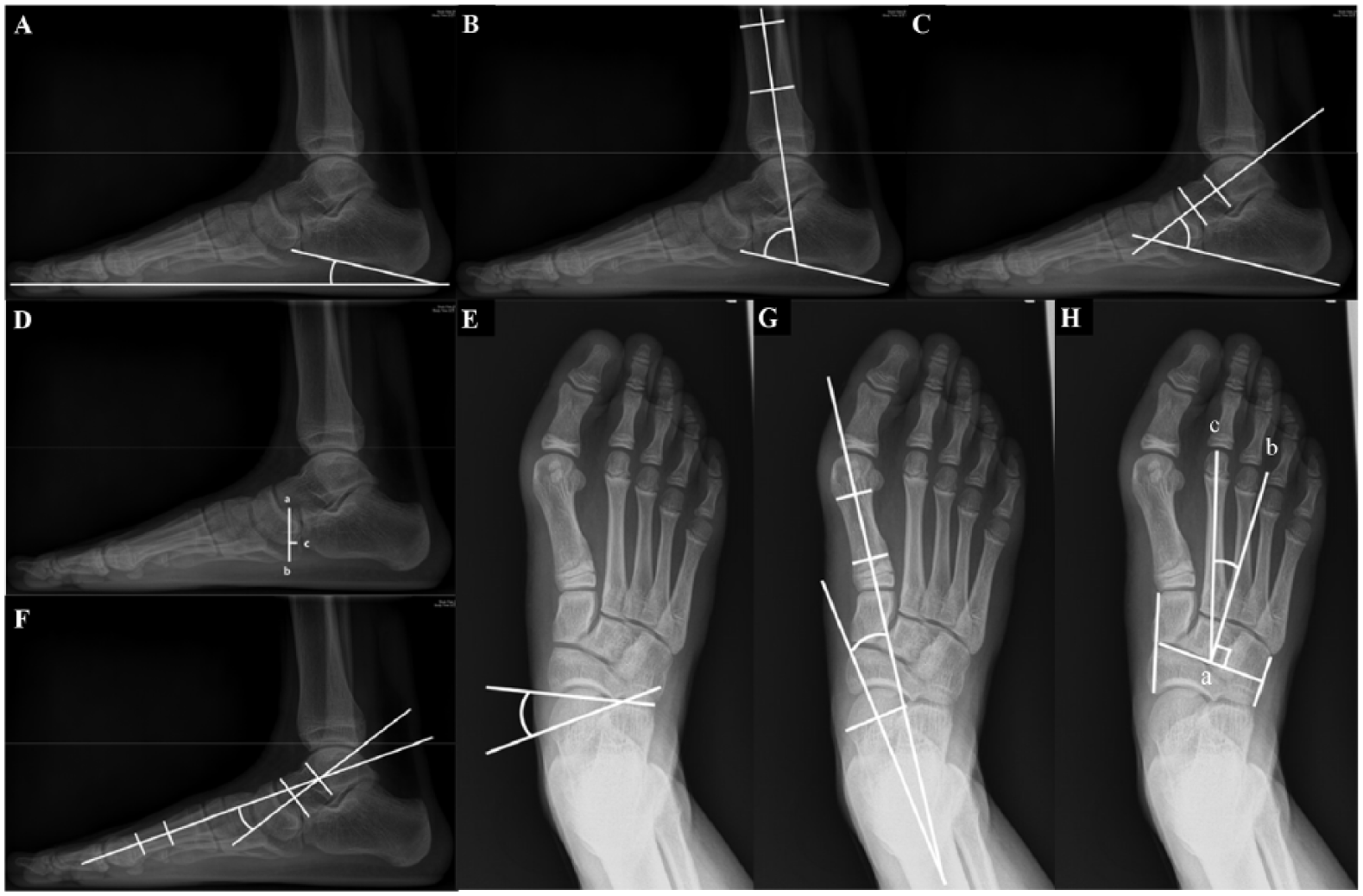
Radiologic measurements of foot alignment. (A) Calcaneal pitch angle: the angle between a line drawn along the edge of the plantar soft tissue shadow and a line drawn along lower calcaneal margin. (B) Tibiocalcaneal angle: the angle between long axis of tibia and a line described in panel A. (C) Talocalcaneal angle: the angle between long axis of talus and a line described in panel A. (D) Naviculocuboid overlap: ac/ab × 100. Superior (a) and inferior (b) margins of cuboid. Inferior navicular margin (c). (E) Talonavicular coverage angle: the angle between a line bisecting anterior articular surface of talus and a line bisecting the proximal articular surface of navicular bone. (F) Lateral talo–first metatarsal angle: the angle between the long axis of talar head and the long axis of first metatarsal bone. (G) AP talo–first metatarsal angle: the angle between a line bisecting the anterior surface of talus and the long axis of the first metatarsal bone. (H) Metatarsus adductus angle: a line (a) connecting the midpoint between the most distal medial point of first cuneiform and the proximal point of navicular bone and the midpoint between proximal and distal lateral points of cuboid bone. Another line (b) perpendicular to line (a) and an angle between line (a) and the longitudinal axis (c) of second metatarsal represents Modified Sgarlato metatarsus adductus angle.
To evaluate degree of hallux valgus, we measured 4 radiologic parameters on standing AP radiographs: hallux valgus angle (HVA), intermetatarsal angle (IMA), distal metatarsal articular angle (DMAA), and first metatarsal cuneiform angle (Figure 2). The first metatarsal cuneiform angle was measured to evaluate the first metatarsal cuneiform joint. 15 An abundance of studies have confirmed the reliability of these determinants in evaluating hallux valgus.5,15,18,24,25 We then compared the degrees of hallux valgus between groups. Finally, the relationships between radiologic parameters reflecting degree of hallux valgus and each radiologic parameter indicative of foot alignment were analyzed.
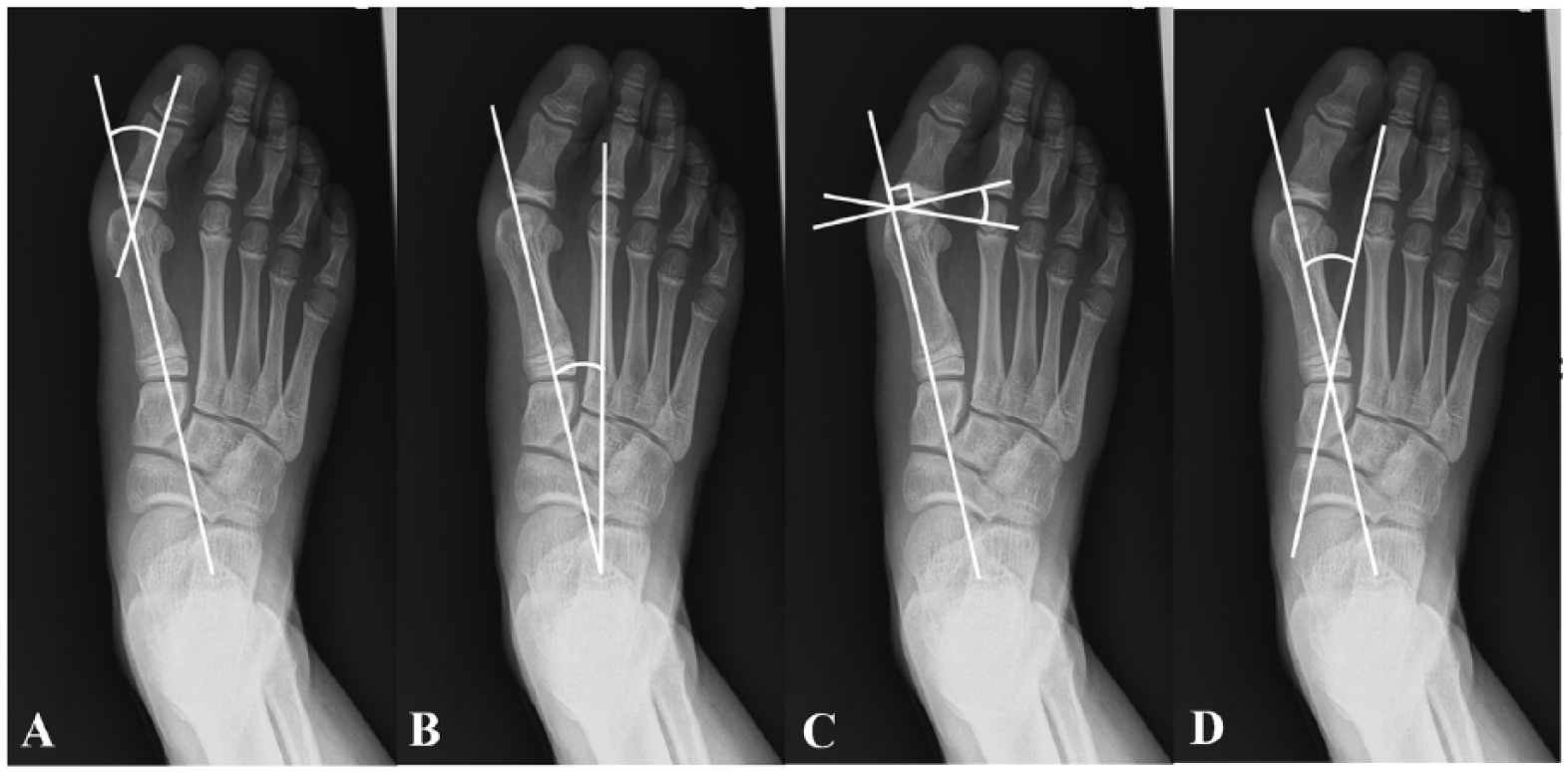
Radiologic measurements assessing degree of hallux valgus: (A) hallux valgus angle: the angle subtended by a line drawn along the central longitudinal axis of the first metatarsal and a second line drawn along the central longitudinal axis of the proximal phalanx. (B) Intermetatarsal angle: the angle subtended at the intersection of 2 lines drawn along the central axes of the first and second metatarsals. (C) Distal metatarsal articular angle: the angle subtended by a line drawn parallel to the articular surface and the central longitudinal axis of the first metatarsal. (D) First metatarsal cuneiform angle: the angle subtended at the intersection of 2 lines drawn along the central axes of the first metatarsal and medial cuneiform.
Statistical Analysis
To compare the 2 groups regarding clinical characteristics and radiologic measurements, the 2-sample t test was used for continuous variables, and the χ2 test was employed to compare categorical variables. To compare clinical characteristics and radiologic measurements among 3 subgroups of each group, a 1-way analysis of variance for continuous variables and the χ2 test for categorical variables were used. A post hoc test with Bonferroni correction was used to assess differing subgroup means. The interrelationships of radiographic indices measured on various planes were defined by Pearson correlation coefficients. Inter- and intraobserver reliabilities were also gauged via intraclass correlation coefficients, interpreted as follows: poor, <0.4; marginal, >0.4 but <0.75; and good, >0.75. All computations relied on standard software (SPSS v23.0; IBM Corp, Armonk, NY), setting significance at P <.05. A post hoc power analysis was also carried out using Power Analysis and Sample Size 11 for Windows software package (NCSS Inc, LLC, Kaysville, UT).
Results
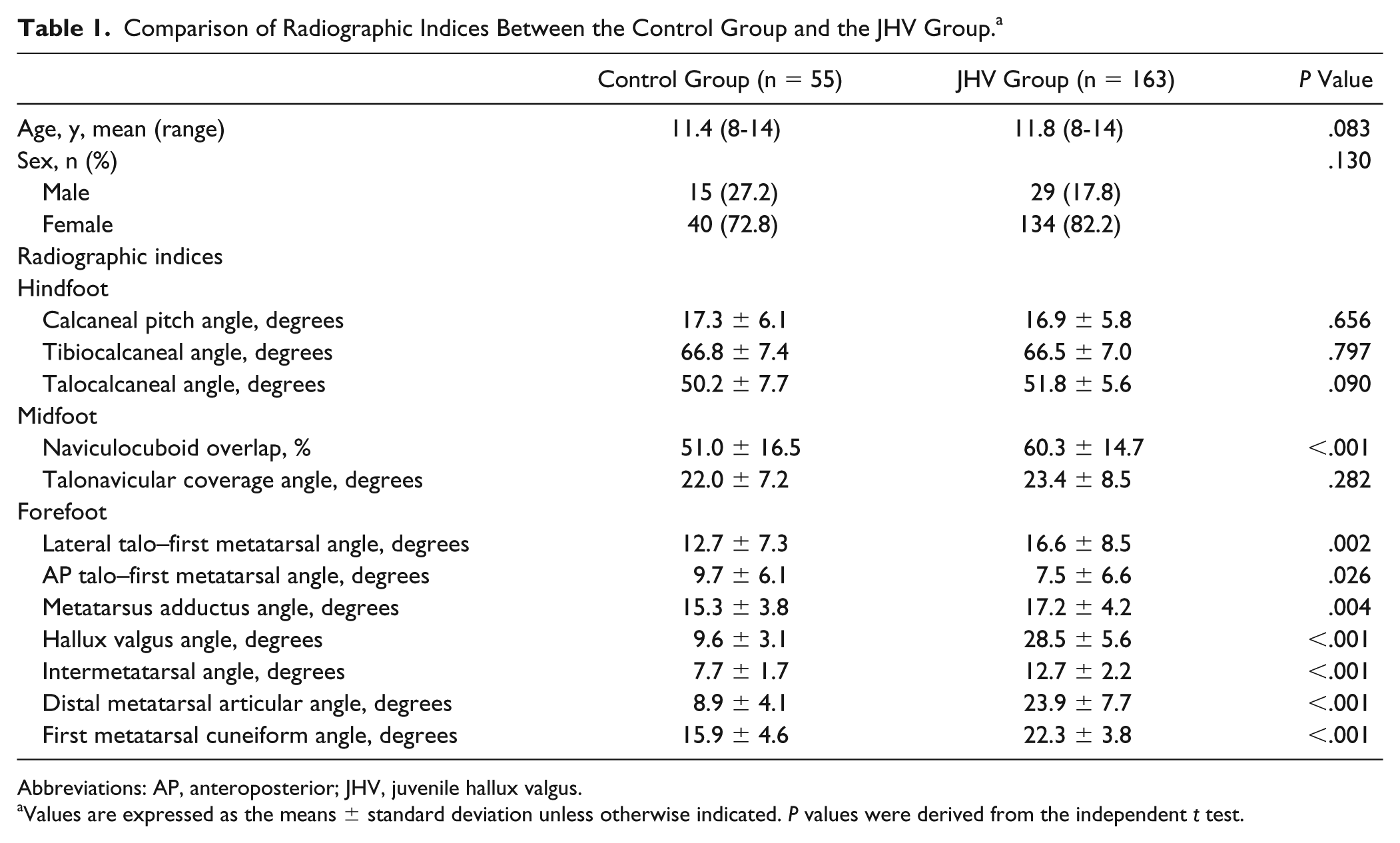
Characteristics of patients with JHV and control subjects are summarized in Table 1. Respective demographics did not differ significantly. Naviculocuboid overlap (P <.001), lateral talo–first metatarsal angle (P = .002), and metatarsus adductus angle (P = .004) were significantly greater in the JHV group than in controls, whereas the AP talo–first metatarsal angle (P = .026) was significantly less. Post hoc power analysis revealed that the power was 0.97 for naviculocuboid overlap, 0.88 for lateral talo–first metatarsal angle, 0.86 for metatarsus adductus angle, and 0.60 for AP talo–first metatarsal angle between JHV group and controls. HVA (P <.001), IMA (P <.001), and DMAA (P <.001), indicating the severity of hallux valgus, were significantly greater in the JHV group than in controls. Interestingly, first metatarsal cuneiform angle (P <.001), representing the motion or orientation of first metatarsal cuneiform joint was also increased in the JHV group compared to controls. The statistical power was 1 for HVA, IMA, and DMAA and 0.99 for first metatarsal cuneiform angle between the JHV group and controls. Other radiologic parameters measured were not significantly different. Of note, the mean radiographic determinants generated for our control group closely approximated values reported in the literature. 7
Comparison of Radiographic Indices Between the Control Group and the JHV Group. a
Abbreviations: AP, anteroposterior; JHV, juvenile hallux valgus.
Values are expressed as the means ± standard deviation unless otherwise indicated. P values were derived from the independent t test.
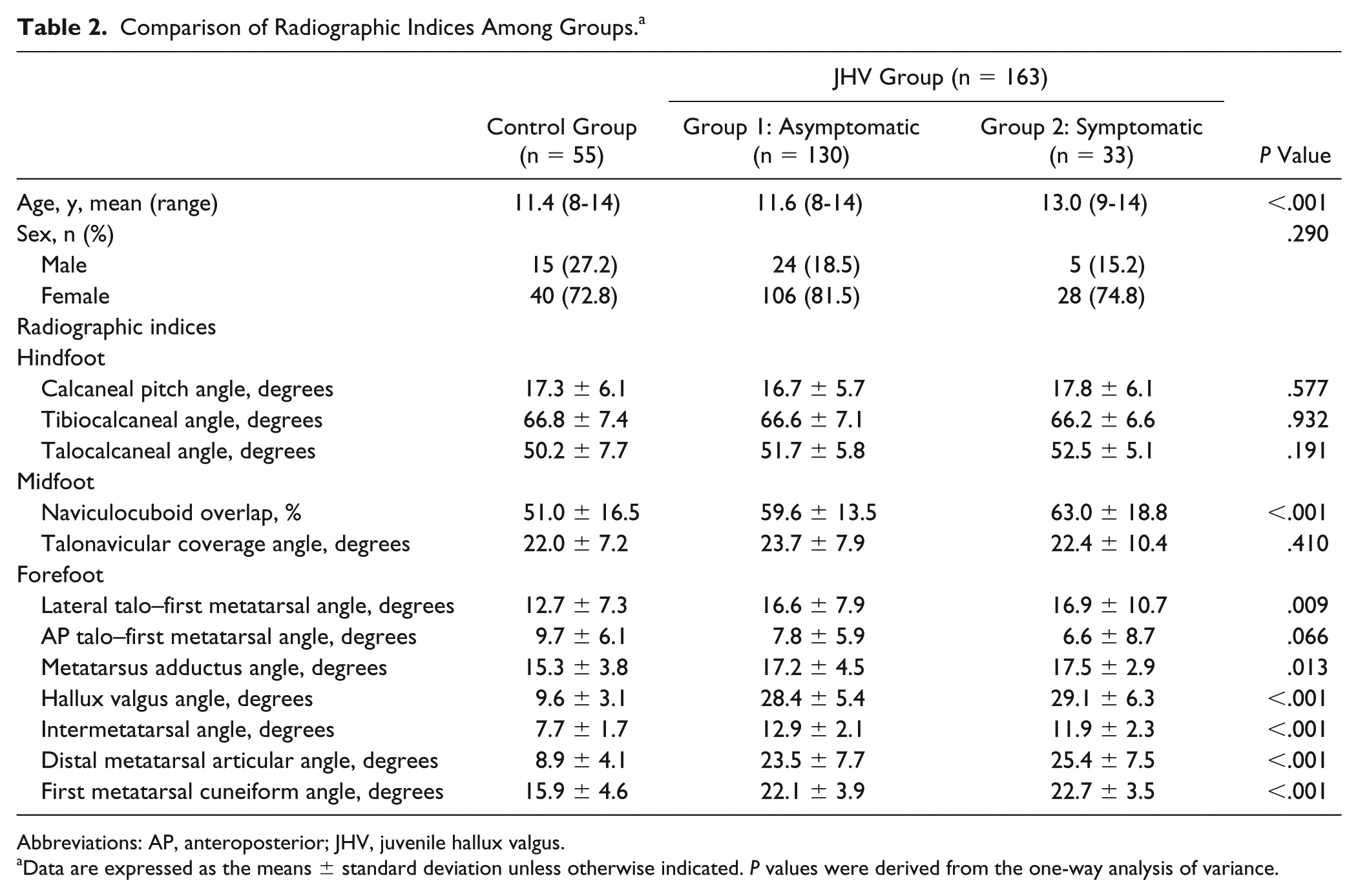
We also compared demographic data and radiologic parameters of the 3 groups (Table 2). The mean age of patients treated with surgery (Group 2) was significantly older than that in the other groups (P <.001), but gender was comparable in all groups. Naviculocuboid overlap (P <.001), lateral talo–first metatarsal angle (P = .009), and metatarsus adductus angle (P = .013) differed significantly among the 3 groups, and post hoc testing showed that these 3 radiographic indices were significantly lower for controls than in group 1 or 2. Post hoc power analysis revealed that the power was 0.93 for naviculocuboid overlap, 0.75 for lateral talo–first metatarsal angle, and 0.87 for metatarsus adductus angle among the 3 groups. Furthermore, none of the radiologic parameters in groups 1 and 2 differed significantly, and there were no significant differences in HVA, IMA, DMAA, and first metatarsal cuneiform angle.
Comparison of Radiographic Indices Among Groups. a
Abbreviations: AP, anteroposterior; JHV, juvenile hallux valgus.
Data are expressed as the means ± standard deviation unless otherwise indicated. P values were derived from the one-way analysis of variance.
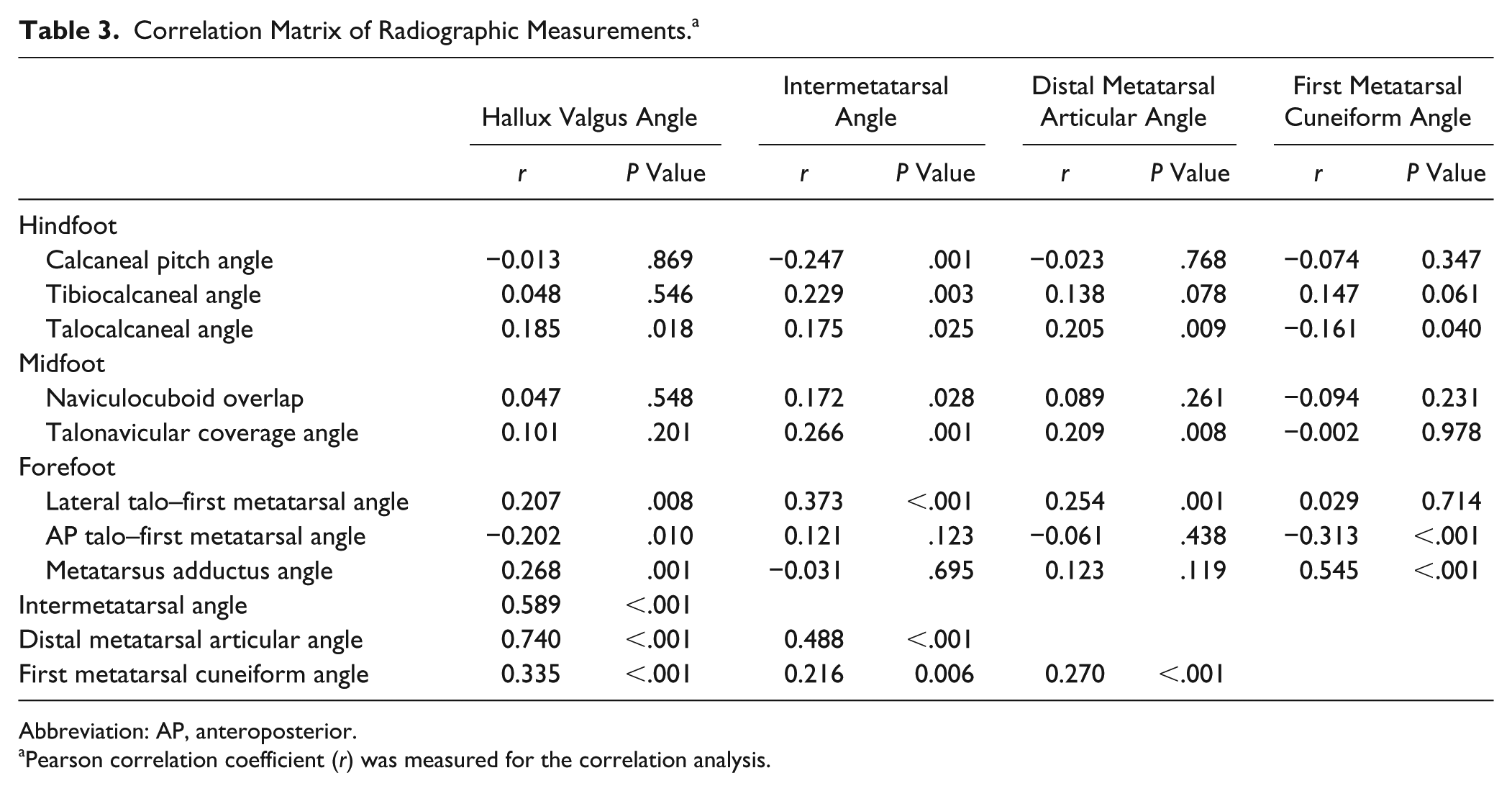
Correlations between radiologic parameters reflecting degree of hallux valgus and each aspect of foot alignment are presented in Table 3. Lateral talo–first metatarsal angle correlated weakly with 3 radiographic parameters: HVA (r=0.210, P = .007), IMA (r=0.373; P <.001), and DMAA (r=0.254; P = .001). The HVA had the highest correlation with the DMAA (r = 0.740, P <.001), followed by the intermetatarsal angle (r = 0.589, P <.001) and first metatarsal cuneiform angle (r = 0.335, P <.001). The IMA had the moderate correlation with the DMAA (r = 0.488, P <.001). The first metatarsal cuneiform angle was correlated with the metatarsus adductus angle (r = 0.545, P <.001) and AP talo–first metatarsal angle (r = −0.313, P <.001). Although there was very weak correlation between some radiologic parameters, there were no significant correlations overall. All measurements showed good intra- and interobserver reliability, with intraclass correlation coefficients ranging from 0.73-0.98.
Correlation Matrix of Radiographic Measurements. a
Abbreviation: AP, anteroposterior.
Pearson correlation coefficient (r) was measured for the correlation analysis.
Discussion
In the present study, the primary findings were not consistent with our hypothesis. The midfoot showed more pronation (higher naviculocuboid overlap), and there was more adduction (higher metatarsus adductus angle and lower AP talo–first metatarsal angle) and more pronation (higher lateral talo–first metatarsal angle) of the forefoot in patients with JHV than in normal controls. As for hindfoot alignment (defined as calcaneal pitch angle, tibiocalcaneal angle, and talocalcaneal angle), patients with JHV did not differ significantly from controls. Given that the term flatfoot implies a condition in which the hindfoot is in valgus, the midfoot is in planus, and the forefoot is abducted and supinated relative to hindfoot, our results indicate that the feet of patients with JHV were not typically flatfoot, substantiating at least some previous reports.3,17,20 However, because there is no universally accepted standard for diagnosis of flatfoot using the values of radiographic parameters measured in our study, determining the proportion of flatfoot in our patients with JHV was not really feasible. Others have cited a prevalence of flatfoot in patients with hallux valgus,3,16 but we believe it impossible to do so without definitive radiologic criteria.
The hindfoot alignment between JHV and normal controls did not differ. This finding was inconsistent with that of a previous paper reporting planus of hindfoot in adolescents with hallux valgus. 16 The reason for such discrepancy may be rooted in the study populations. Whereas one-third of patients in the latter report had neuromuscular disorders, we excluded patients with underlying diseases. We consider our results a more accurate depiction of alignment in patients with idiopathic JHV. In another study, simultaneous operative correction of hindfoot valgus was advised to prevent recurrence of hallux valgus in a child presenting with both hallux valgus and flatfoot. 12 In cerebral palsy patients, correction of hallux valgus is rarely performed in isolation and associated etiologic factors should be addressed simultaneously to prevent recurrence of deformity. 6 But our results do not validate this approach in patients with JHV, and overall, there is little agreement on the need for surgery of concurrent flatfoot.1,3,17 This operative strategy should be applied cautiously and only in particular instances of JHV, because hindfoot alignment in this setting is not associated with development of hallux valgus.
In patients with neuromuscular disease, such as cerebral palsy, the relationship between flat foot and hallux valgus may be different from that in patients with idiopathic hallux valgus. Hallux valgus is frequently seen in association with planovalgus foot. 6 Previously suggested etiologies were intrinsic muscle imbalance and abnormal extrinsic loading due to disruption of forefoot mechanics during the stance phase.8,27 The latter theory may be valid in the development of idiopathic hallux valgus. But, all patients with JHV did not have a flatfoot in our study. In addition, there was an opinion of some surgeons that flatfoot has clinical relevance only within the context of neuromuscular deficit. 4 We believe that a pronated midfoot, not valgus of the hindfoot, may be a primary factor in the development of idiopathic hallux valgus.
A pronated foot in the setting of JHV may impact the height of longitudinal arch, without changing hindfoot alignment. As the foot pronates, the first metatarsal bone rotates on its longitudinal axis and may reduce the longitudinal arch height, without a valgus heel. 11 A diagnosis of flatfoot in practice is based to a greater extent on clinical appearance than on radiographic measurements. Pronated feet in patients with JHV may have the appearance of flatfoot while lacking radiologic support.
The forefeet of our patients with JHV were more adducted and pronated than those of normal controls. To define forefoot alignment, we used AP and lateral talo–first metatarsal angles, and although hindfoot alignment may exert some influence, others have corroborated the relevance of these angles in forefoot alignment. 29 A deformity of the first metatarsal may have some effect as well, so we added the metatarsus adductus angle to ensure accuracy in assessing the forefoot. Consequently, the forefoot profiles in patients with JHV differed entirely from that of flatfoot, which previous reports have also shown,3,4 linking JHV with metatarsus adductus instead.
In the JHV group, DMMA and first metatarsal cuneiform angle were much greater than in control group. The higher DMMA indicates the distal valgus deformity of the first metatarsal and may be a distinctive characteristic of the JHV. 3 The higher first metatarsal cuneiform angle represents the proximal varus deformity of first metatarsal related to the flexibility of the first metatarsal cuneiform joint. 15 Increased first metatarsal cuneiform angle may be also a unique feature in JHV.
The radiologic parameters in symptomatic and asymptomatic subsets of our patients with JHV did not prove significantly different. Thus, foot alignment was unrelated to the presence of symptoms in these patients. Furthermore, there were no significant differences in HVA, IMA, DMAA and first metatarsal cuneiform angle in symptomatic and asymptomatic patient subsets, leading us to conclude that the degree of hallux valgus had no bearing on symptoms. We were then at a loss to explain why some patients with JHV experience pain. Although not statistically significant, naviculocuboid overlap was greater in symptomatic (vs asymptomatic) patients, implying that pronation deformity was more prominent in instances of painful JHV. It is likely that the degree of pronation may be a factor in patients with JHV who become symptomatic. These findings correlate well with current recommendations that rotational correction should be included as part of the surgery when performing a metatarsal osteotomy or a Lapidus procedure. 28
In our study, the lateral talo–first metatarsal angle weakly correlated with HVA, IMA, and DMAA, though the R-squared values were low. This result shows the weak relationship between the amount of forefoot pronation and degree of hallux valgus. 11 Additionally, the HVA strongly correlated with IMA and DMMA, consistent with previous report. 18 On this basis, we could reconfirm that the complex 3-dimensional nature of hallux valgus can include concurrent valgus and pronation of the first metatarsal bone.
The first metatarsal cuneiform angle was correlated with metatarsus adductus angle and AP talo–first metatarsal angle. This means that the medial deviation of the first metatarsal may be present in the forefoot. Further study is needed to establish the relationship between the flexibility of metatarsocuneiform joint and pronation of the midfoot and forefoot in JHV.
This study has several limitations, the first being its retrospective and cross-sectional design. We measured radiographic parameters at initial visits, with no follow-up of patients who were treated conservatively. Some may have undertaken the correctional surgery at other facilities as a result of later developing pain. Another issue is the disproportion between patients with symptomatic and asymptomatic JHV. Most patients with JHV have no symptoms, so the relatively few who were symptomatic may have lowered the power of statistical analysis. Finally, the pain levels in patients studied were measured subjectively. To accurately assess the degree of pain in patients with JHV, an objective means of measuring pain may be needed.
Conclusion
The radiographic parameters of patients with JHV were not characteristic of flatfoot. The hindfoot was in neutral alignment, midfoot was pronated, and forefoot was pronated and adducted. Furthermore, the foot alignment in patients with JHV seemed to be unrelated to the presence of symptoms or degree of hallux valgus.
Supplemental Material
FAI850148-ICMJE – Supplemental material for Radiographic Assessment of Foot Alignment in Juvenile Hallux Valgus and Its Relationship to Flatfoot
Supplemental material, FAI850148-ICMJE for Radiographic Assessment of Foot Alignment in Juvenile Hallux Valgus and Its Relationship to Flatfoot by Hyun Woo Kim, Kun Bo Park, Yoon Hae Kwak, Seokhwan Jin and Hoon Park in Foot & Ankle International
Footnotes
Acknowledgements
We thank Dr. Jung Woo Lee for the data collection of the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.